
Abstract
The use of herbal medicines by pregnant women varies among different countries, ranging from 4.3% in Sweden to 69% in Russia. The aim of this narrative review is to evaluate the benefits and safety of common herbal medicines used during pregnancy. A systematic literature search (from 1995 to February 2018) was performed using a variety of electronic databases. The levels of evidence of the clinical studies were graded using the Oxford Centre for Evidence-Based Medicine levels of evidence guidelines. From the 736 articles retrieved, 69 articles were used for this review. Ginger has been investigated extensively and has been consistently found to decrease nausea and vomiting associated with pregnancy (Level 2). There is insufficient evidence concerning the efficacy of other herbal medicines such as garlic, cranberry and raspberry in pregnancy (Level 3–4). Much of the literature is based on case reports with limited pharmacodynamic/kinetic studies. There are no clear data on the adverse herb–drug interactions during anaesthesia. As the risks of these interactions are unknown, it would be prudent for anaesthetists to explicitly ask their patients about their use of herbal medicines before surgery and prior to labour and birth. The European Society of Anaesthesiology and American Society of Anesthesiologists recommend that patients cease taking herbal medicines two weeks before surgery.
There is much diversity in the use and roles of traditional, complementary and alternative medicine as a result of cultural practices and beliefs. The consumption of herbal medicines has increased worldwide.1–3 Many consumers believe herbal medicines are of “natural” origin and therefore are safer alternatives to conventional medicines.1,2
Herbal medications have been associated with harmful effects as a result of direct toxicity, herb–drug interactions, toxic constituents, contamination or adulteration with toxic metals or even undisclosed conventional drugs (e.g. steroids, non-steroidal anti-inflammatory drugs (NSAIDs)). 4 In a cross-sectional study of 947 patients in Israel, Levy et al. reported that an adverse event occurred in 3.7% of patients who consumed dietary and herbal supplements. 5 In a cohort study of 601 general surgical patients consuming traditional Chinese herbal medicines (TCHM), Lee et al. reported that patients who had been prescribed TCHM were twice as likely to experience hypokalaemia and impaired haemostasis (as measured by prolonged International Normalized Ratio (INR) or activated partial thromboplastin time (aPTT)) preoperatively. 6
Parturients are apprehensive about the potential adverse effects of conventional medicines consumed during pregnancy, and so they take herbal products instead because they are believed to be harmless. 7 However, the belief of their efficacy and safety in pregnancy is not evidence-based.
The aim of this narrative review is to evaluate the evidence on the efficacy and adverse effects of the common herbs used in the peripartum period and perioperative anaesthetic considerations.
Search strategy
A systematic literature search was performed on MEDLINE, PubMed, CINAHL and AMED (Allied and Complementary Medicine Database) databases from 1995 to February 2018 using the following key words: herbs, herbal medicine and supplements, complementary medicine, alternative medicine, Chinese herbal medicine, Ayurvedic medicine, pregnancy, labour, obstetrics, and midwifery. The search was limited to articles published in the English language and human studies. Data from studies involving acupuncture, transcutaneous electrical nerve stimulation, massage therapy, reflexology, aromatherapy, hypnosis, vitamin supplements or animal and in vitro studies were excluded. The search results were imported into “Endnote”, a bibliographic management program, and duplicate items were removed. The bibliographies of the retrieved articles were examined for additional relevant articles. From a total of 736 articles retrieved, 69 articles were included in this review. The levels of evidence of the clinical studies were graded using the Oxford Centre for Evidence-Based Medicine levels of evidence guidelines 8 (Table 1).
Levels of evidence and grades of recommendation according to Oxford Centre for Evidence-Based Medicine 2011.
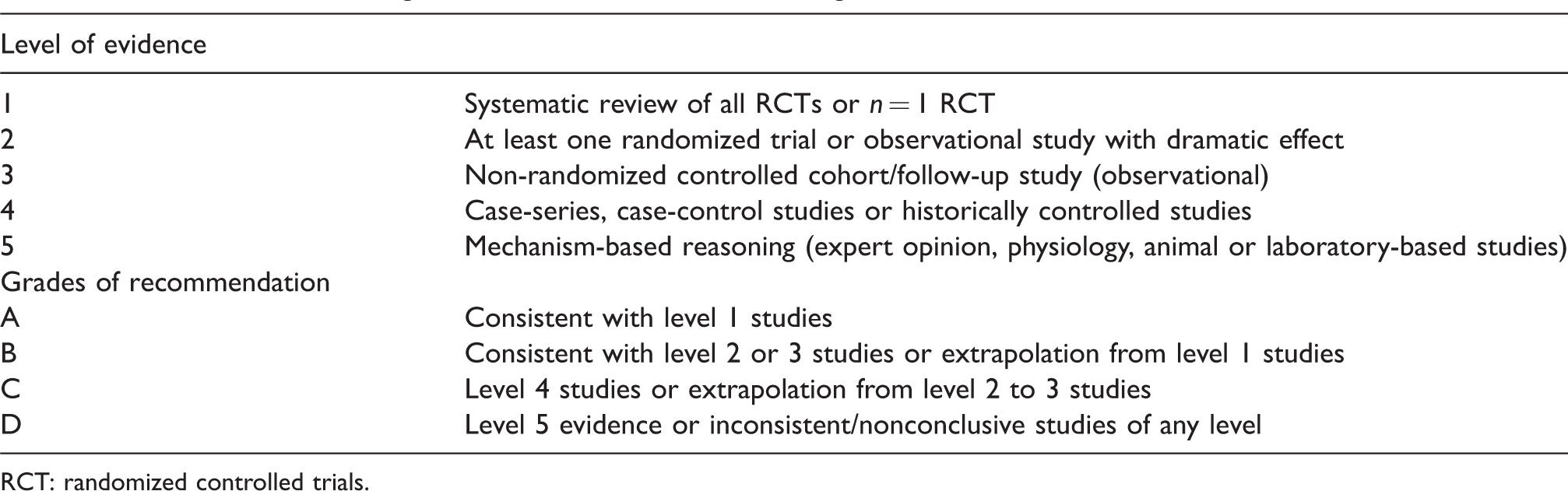
RCT: randomized controlled trials.
Prevalence
The prevalence of the consumption of herbal medicines by pregnant women ranged from 4.3% in Sweden up to 69% in Russia. 9 The prevalence was 52%–58% in Australia, 10 40%–48% in Norway and Italy,11–13 6%–9% in Canada and USA,14,15 58% in Malaysia 16 and 43%–45% in China. 17 Several surveys in Western countries have reported that consumption of herbal products was most frequent in parturients in the 41- to 50-year age group, and with higher education and income levels.18,19 In contrast, there is an inverse association between income and herbal consumption in China and Hong Kong. 17 This is attributed to the lower cost of herbal medicines in these countries making them more affordable to mothers with low family income. Other factors associated with consumption of herbal products include habitual or previous use of complementary medicine, primiparity, non-smoking and the desire for a natural birth. 20
In a survey in the United Kingdom, almost half of pregnant women were prescribed conventional medicines and almost half of these patients used herbal medicines. This raises concerns of potential drug–herb interactions. In early pregnancy, the herbal medicines most commonly used were ginger (35.6%), chamomile (23.2%) and raspberry (20.5%), whereas in late pregnancy the herbal medicines used were raspberry (42.5%), cranberry (26.7%), ginger (23.7%) and chamomile (11.8%). More than half of the parturients used more than one herbal product. 21 In Eastern countries, the types of herbs are more varied; Angelica sinensis (dong quai) is most popular among Chinese mothers as it ‘enriches’ the blood and circulation; and white atractylodes rhizome, Glycyrrhizae radix (liquorice root) and Ginseng radix are popular with Korean mothers. 22
Indications
Several complementary and alternative medicine approaches for nausea/vomiting, pain management, preconception, pregnancy or induction of labour have been used. 23 Several studies have described the use of herbal medicines for relief of stress and pregnancy-related symptoms, postpartum care, preparation for labour and for general health. 20 Other studies examined the efficacy of herbal medicines for nausea 24 and low back pain during pregnancy. 25
Preconception
The prevalence of the consumption of herbal drugs to enhance fertility is reported to be 8.3%–29% of patients attending infertility clinics in Australia. 26 Stankiewicz et al. found that green tea (27%, as an antioxidant), chamomile (13%), echinacea (8%), peppermint (7%), chaste tree berry, astragalus (5%), ginseng (4.2%) and horseradish (4%) were the herbal remedies used because it was believed that they enhanced fertility. 27
Herbal drugs used during pregnancy
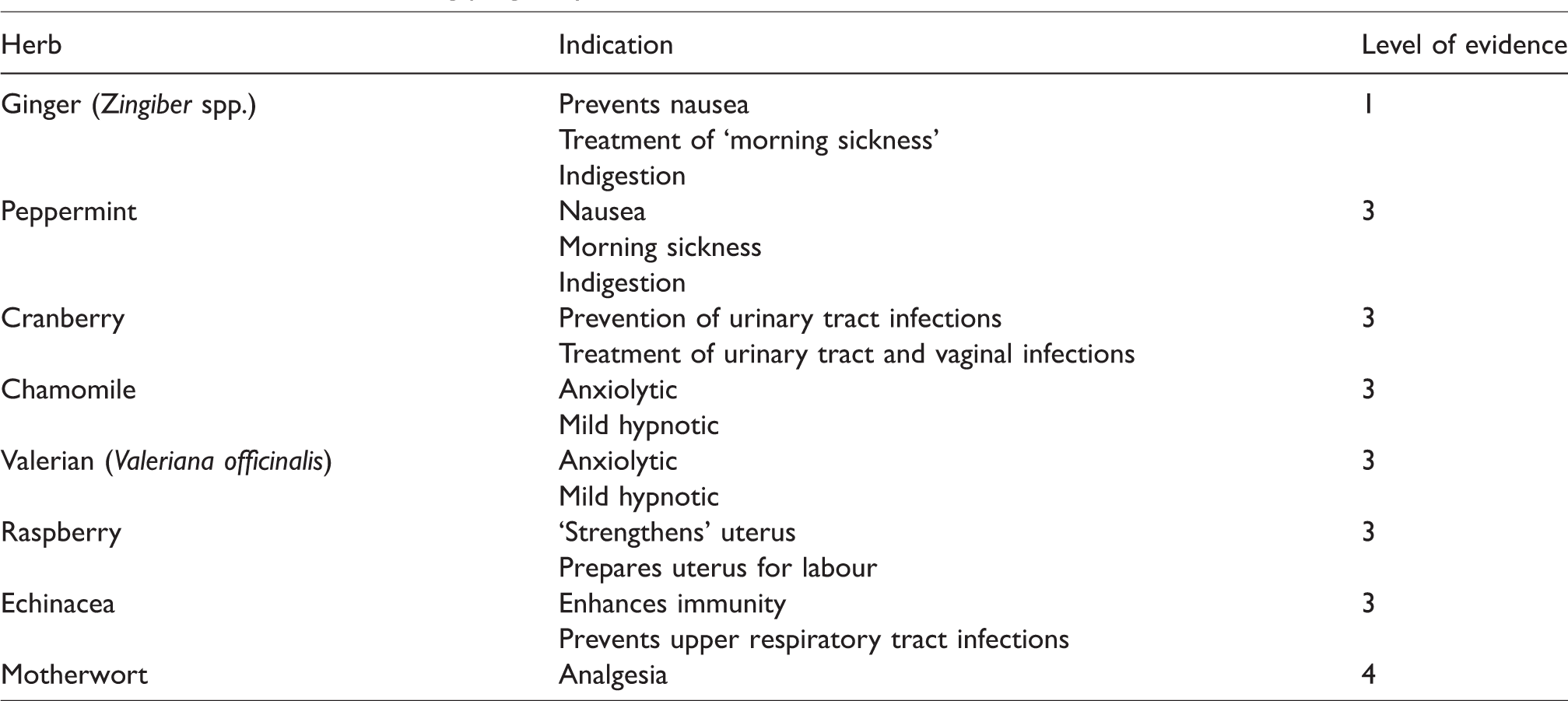
Herbal supplements are taken to reduce or treat minor symptoms such as nausea and vomiting, indigestion/dyspepsia, backache, bladder/urinary symptoms, anxiety and to ‘boost’ the immune system. 7 The choice and incidence of herbal medicine use varies during the different phases of pregnancy. Maats and Crowther 28 found that commonly used herbal medicines were ginger (42%) and chamomile (9%) in the first trimester, chamomile (13.6%) and ginger (9%) in the second trimester, and raspberry leaf tea (8%) and chamomile (6%) in the third trimester. Ginger is the most popular herb used to reduce or treat nausea and/or vomiting. Other antiemetics included wild yam (Dioscorea villosa) and red raspberry (Rubus idaeus) (Table 2).
Common herbs used during pregnancy.
Cervical ripening
Evening primrose oil is used by some midwives to trigger cervical ripening and therefore help initiate labour. In a retrospective study, evening primrose oil increased the incidence of prolonged rupture of membranes, oxytocin augmentation and vacuum extraction of the infant, shortening neither gestation nor duration of labour. 29 Other herbs used for cervical ripening include Lobelia inflata and Gossypium herbaceum (cotton root) (Table 3).
Herbs used prior to labour.
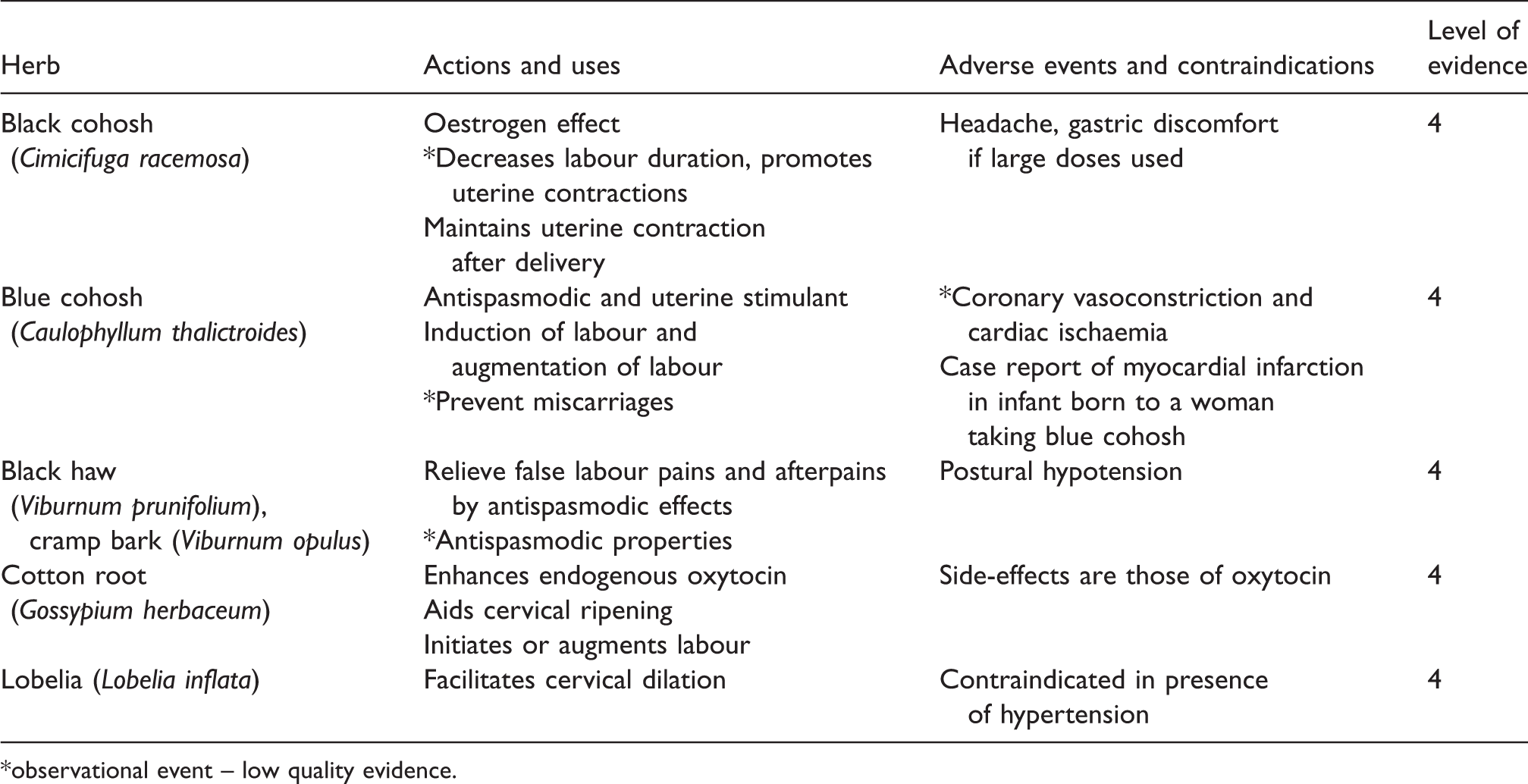
*observational event – low quality evidence.
Herbs used for induction of labour
Raspberry (usually taken as a tea), blue cohosh and castor oil are used in traditional midwifery either to ‘prepare’ the uterus for labour or stimulate the uterus. The mechanism of action of these herbal medicines in uterine stimulation is uncertain, although it has been proposed that they may have either a spasmolytic or stimulatory effect on the uterus. Although castor oil is commonly used as a laxative, midwives and parturients use it to initiate labour. Castor oil stimulates uterine contraction by increasing the production of prostaglandin F2 alpha in the uterus. 30 The mechanism of action of blue cohosh is mediated by glycosides (caulosaponin, caulophyllosaponin) and sparteine, which induce uterine contraction. However, they are not recommended as they have been associated with coronary vasospasm resulting in myocardial ischaemia in the fetus. 31
Herbs used to relieve anxiety and pain during labour
A combination of herbs that have anxiolytic properties is commonly recommended (Table 2). A variety of herbs are used as anxiolytics to facilitate a pleasant experience in labour. 32 Valerian, passionflower and chamomile are used for their calming and relaxation properties. 33
In the USA, independent midwives promoted the use of herbal remedies for the relief of labour pain and discomfort. In addition to massage therapy, hydrotherapy, breathing and relaxation techniques, they promoted herbal mixtures consisting of motherwort, wild ginger, lobelia, wild yam, blessed thistle, blue cohosh, squawvine, false unicorn and bayberry root to provide analgesia and relaxation. Most of the herbs either had anxiolytic effects or reduced dysfunctional labour by mild uterine stimulating effects. Labour pain was frequently treated with motherwort. 1
Herbs used in the postpartum period
Herbal medicines used to treat some of the symptoms during pregnancy may be continued into the postpartum period. Lavender oil is used to relieve perineal discomfort after vaginal delivery. A double-blind randomized clinical study failed to show any reduction in postnatal perineal discomfort. 34
There are different dietary practices in the postpartum period among different cultures. In Chinese culture, ‘ginger–vinegar soup’ is ingested to “enrich blood and strengthen internal organs”. The soup contains ginger, sweet vinegar, dates, chicken and pig trotters. 35 Large quantities of ginger may be consumed in the first month after delivery if this soup is consumed, which predisposes to the potential adverse effects of ginger.
St John’s wort is advocated for postnatal depression.36,37 In a prospective, observational cohort study in 33 breastfeeding women receiving St John’s wort for postnatal depression no significant adverse effects associated with lactation or breastfeeding were found. 38
Most studied herbal medicines
Ginger
Ginger is a popular herbal drug in many Asian countries. It has been used in Chinese and Ayurvedic (Indian) traditional medicine for thousands of years to stimulate digestion and for its antiemetic, antitussive and anti-inflammatory properties. During pregnancy it is mainly used as an antiemetic in the first trimester. The use of ginger during pregnancy has been extensively studied in 10 randomized controlled trials (RCTs) (Level 1; grade B recommendation) (Table 4).
Randomized controlled trials using ginger for nausea and vomiting.
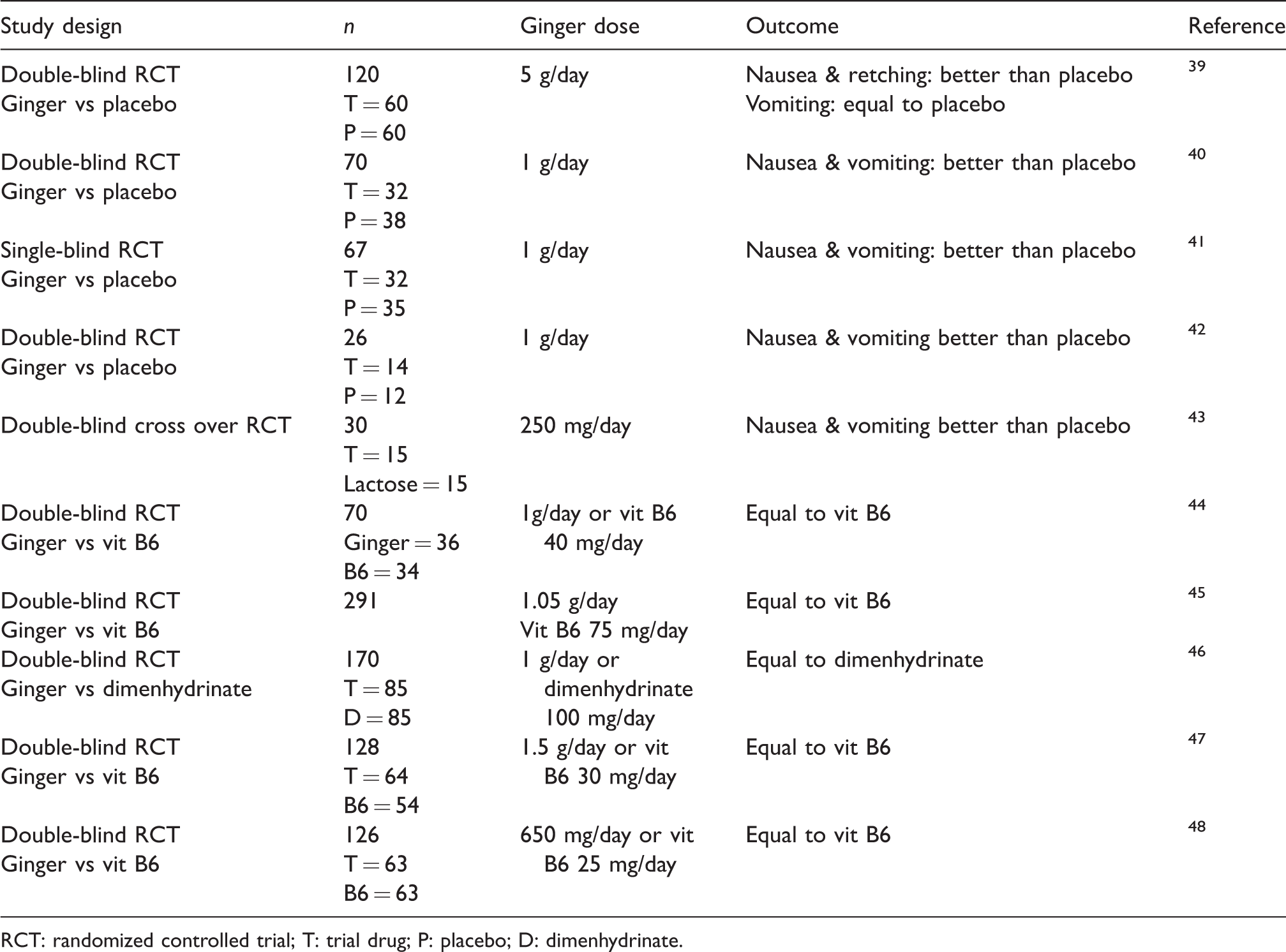
RCT: randomized controlled trial; T: trial drug; P: placebo; D: dimenhydrinate.
Out of the 10 RCTs that evaluated the antiemetic effects of ginger, five RCTs39–43 reported that ginger was superior in reducing nausea and vomiting compared with a placebo, whereas five44-48 found ginger equally effective when compared with dimenhydrinate or vitamin B6. There were no increased adverse events or risks to the fetus.49,50 The recommended daily dose of ginger for the treatment of nausea and vomiting is 1000 mg. It is proposed that the antiemetic properties of ginger are mediated by serotonin antagonism in the gut and the central nervous system (CNS). When the maximum daily dose of 4 g is exceeded, several adverse effects such as cardiac arrhythmias, CNS depression and coagulopathy may occur. 51 Coagulopathy is caused by antiplatelet effects due to inhibition of thromboxane synthetase. 52 Consequently, large doses of ginger should not be administered with antiplatelet drugs or warfarin. 53 Ginger should be used with caution in gestational diabetes because it has been reported to potentiate hypoglycaemia with insulin and the oral hypoglycaemic drugs. 51
Cranberry
The main indication for taking cranberry during pregnancy is to prevent or treat urinary tract infection. The mechanism by which cranberry prevents urinary tract infection is mediated by two compounds in the fruit, fructose and proanthocyanidin, that prevent Escherichia coli from adhering to the urethral epithelial lining. In an RCT, Wing et al. investigated the efficacy of cranberry extract with placebo in prevention of urinary tract infection in pregnant women and reported multiple daily dosing reduced frequency of asymptomatic bacteriuria (57%) and urinary tract infection (41%). 54 However, the study was underpowered because 38.8% of subjects withdrew, most for gastrointestinal symptoms. The authors concluded that cranberry may have a protective effect against urinary tract infection during pregnancy but further larger studies are required (Level 3; grade C recommendation).
Raspberry
Since the 6th century, raspberry has been taken during pregnancy to shorten labour by augmenting uterine contractions and to reduce uterine bleeding. In an RCT, Simpson et al. reported that raspberry ingestion did not shorten the first stage of labour but reduced the rate of forceps delivery (19.3% versus 30.4%) and the duration of the second stage of labour (mean difference −9.5 min) (Level 3; grade C recommendation). 55 It is not associated with any maternal or fetal adverse effects.
Garlic
The traditional indication for garlic is to prevent colds, influenza and gastroenteritis 56 (Level 3; grade C recommendation). It has been suggested that it inhibits platelet aggregation and oxidative stress. This led to the hypothesis that garlic may be beneficial in pre-eclampsia. However, one RCT showed that it was not efficacious in reducing the incidence of hypertension or pre-eclampsia. 57 Consumption of large doses of garlic is associated with platelet dysfunction. 58
Blue cohosh
Blue cohosh is used as a uterine stimulant to induce and augment labour 59 in the late stages of pregnancy (Level 4; grade C recommendation). However, animal studies have reported serious coronary vasoconstriction resulting in myocardial ischaemia. Myocardial infarction in an infant born to a mother who had been taking blue cohosh during the last month of pregnancy has been reported. 54
Black cohosh
Black cohosh, which has oestrogen-like properties, is used in the last few weeks of pregnancy to promote rhythmic uterine contractions and maintain a contracted uterus after delivery 59 (Level 4; grade C recommendation). Unlike blue cohosh, no adverse effects have been reported.
Castor oil
Castor oil is used to initiate labour. A prospective study by Garry et al. showed a significant increase in the rate of initiation/induction of labour 60 (Level 4; grade D recommendation). However, Boel et al. showed that it increased nausea and could not demonstrate any effect on initiation of labour. 61
Echinacea
Echinacea is used to promote the immune system to protect against upper respiratory tract infections. In a prospective cohort study of 206 pregnant women who used echinacea during the first trimester for upper respiratory tract ailments, respiratory symptoms in the treated group improved compared with the non-treated group (Level 3; grade C recommendation). 62 There were no fetal malformations. Prolonged consumption of echinacea (>8 weeks) can cause liver dysfunction. 63
Chinese herbal medicines
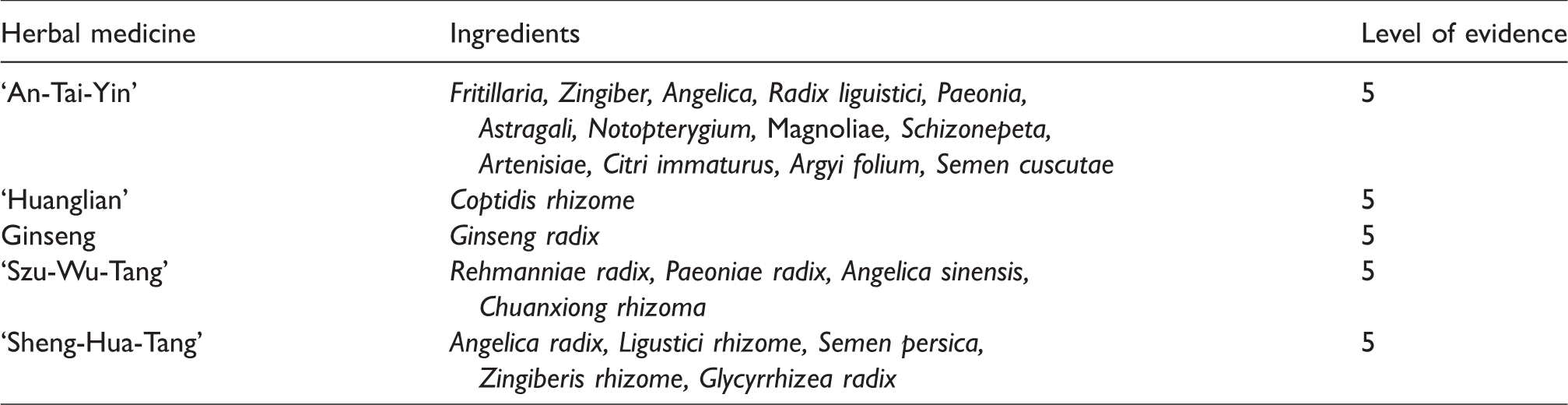
Chinese herbal medicines usually contain either raw or processed ingredients from one or more plants. Animal or inorganic substances are sometimes added to the herbs. In some instances, conventional drugs such as steroids and NSAIDs are added but not disclosed. 3 The common Chinese herbal products include An-Tai-Yin, Pearl power, Huanglian, Szu-Wu-Tang and Ginseng during pregnancy, and Sheng-Hua-Tang and Szu-Wu-Tang in the postpartum period. 64 Dong quai (Angelica sinensis) is taken as a powder contained in capsules by Chinese women for postpartum weakness and uterine hypotonia (Table 5). There are no good-quality studies on the safety and efficacy of the use of TCHMs (Level 5; grade D recommendation). Green tea (Melissa officinalis) can induce early maternal hypothyroidism, as the isoflavanoids inhibit thyroperoxidase and deiodinases resulting in low T3 levels. 65 Hypotension and delayed recovery from general anaesthesia may result from this unexpected hypothyroidism (Level 4 evidence).
Examples of Chinese herbal medicines used in pregnancy.
Anaesthetic considerations
There are currently no clear data on the specific adverse interactions between herbal medicines and anaesthetic drugs. The available data on the risks and probable herb–anaesthetic drug interactions is based on case reports and limited pharmacodynamic/kinetic studies.
Self-prescription of herbal medicines is common. A high proportion of pregnant women (76%) fail to disclose to their midwife or obstetrician that they are taking herbal medicines. 11 A common reason for this lack of disclosure is simply because the women are not asked by their care providers. 66
As regional anaesthesia is advocated in obstetrics, the potential for coagulopathy and haemodynamic instability are major concerns. Large doses of garlic, ginseng and ginger impair platelet function by inhibiting thromboxane synthetase. Coagulopathy is only a concern when large doses of garlic, ginseng and ginger are consumed in the peripartum period (Level 4). Caution should be undertaken when managing postpartum Chinese women, as they may take large doses of ginger (>4 g) in the ‘ginger–vinegar soup’. In a study investigating the incidence and risk of perioperative events among surgical patients taking TCHMs, Lee et al. found that ginger consumption was not associated with prolonged aPTT or INR. 6 They found no spinal or epidural haematomas in 133 patients who were taking TCHMs and who underwent regional anaesthesia. This supports the recommendations of the American Society of Regional Anesthesia Consensus on Neuraxial Anesthesia and Antithrombotic Therapy, which states that “herbal drugs, by themselves, appear to represent no significant risk for the development of spinal hematoma in patients having epidural or spinal anesthesia”. 67
When pregnant women take traditional Chinese or Ayurvedic medicines, the potential for adverse effects of contamination or undeclared added metals, steroids or NSAIDs should be considered. Lead and arsenic added to these traditional medicines can cause bone marrow depression, and the addition of NSAIDs can cause excessive bleeding.
Limitations of review
There are several limitations of this narrative review. As it was restricted to English language publications, issues related to publication bias arise especially as different cultures use different herbal medicines. Moreover, some medicinal plants are used as food and not as medicines. Much of the evidence comes from case reports and low-quality studies. The active constituents of the herbal medicines may vary in concentration and composition as they are not regulated.
Conclusion
Despite the popularity and widespread use of herbal medicines during pregnancy, there are very few good-quality studies of these drugs and their adverse effects. No definitive recommendations concerning the perioperative safety of these herbal medicines can be made because randomized double-blind placebo-controlled studies are not available. The American Society of Anesthesiologists 68 and the European Society of Anaesthesiology 69 guidelines on preoperative evaluation of adults undergoing elective non-cardiac surgery suggest that herbal medicines are stopped two weeks prior to surgery and that patients should be explicitly asked about their intake of herbal drugs (e.g. ginger, ginseng, garlic and gingko) that may impair coagulation. There is no evidence to postpone elective surgery, but for obstetric surgical procedures associated with massive haemorrhage it may be prudent to perform preoperative coagulation screening tests and use intraoperative point-of-care coagulation monitoring. Further research and longitudinal observational studies are required to provide clear data on the safety of herbal medicines in regard to anaesthesia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.