
Abstract
Follow-up for ongoing management and monitoring of patients is important in clinical practice and research. While common, telephone follow-up is resource intensive and, in our experience, yields low success rates. Electronic communication using mobile devices including smartphones and tablets can provide efficient alternatives — including SMS (text), online forms and mobile apps. To assess attitudes towards electronic follow-up, we surveyed 642 parents and carers at Perth Children’s Hospital, targeting demographics, device ownership and attitudes towards electronic follow-up. Mobile phone ownership was effectively universal. Almost all respondents were happy to communicate electronically with the hospital. Promisingly, 93.2% of respondents were happy to receive follow-up SMSs from the hospital and 80.3% were happy to reply to SMS questions. There was less enthusiasm regarding other modalities, with 59.9% happy to use a website and 69.0% happy to use a mobile app. The results support the introduction of electronic communication for follow-up in our paediatric population.
Background
Perth Children’s Hospital is the only tertiary paediatric hospital in Western Australia and therefore treats a broad patient demographic, including children who travel great distances to attend the hospital. In the Department of Anaesthesia and Pain Management our research and quality activities include monitoring how children recover at home following procedures. We usually do this by telephone, often with repeated follow-up calls (e.g. every two days for two weeks, or until pain has resolved).
In our experience telephone follow-up is resource intensive and yields low success rates. In one audit, despite 2339 attempts to contact 979 families only 810 (83%) were successfully contacted (author’s unpublished data). We currently allow up to ten attempts per family when following up trial participants.
Telephone follow-up is also used in the hospital as part of routine clinical care. Patients are more vulnerable to adverse events after discharge 1 and comprehensive telephone follow-up can improve children’s outcomes and parent satisfaction, and reduce re-presentation and re-admission.2–4 However, this is also subject to the same challenges we face when using telephone follow-up for audit purposes, which may limit this practice.
We propose that SMS messaging or mobile device applications may provide a more efficient alternative for both clinical and research follow-up. While generally children’s families are willing to receive electronic communications from hospitals and medical practitioners,5,6 we wished to assess the attitudes of our population. We therefore performed a prospective audit of the prevalence and types of mobile devices owned by parents of children receiving treatment at our hospital as well as the willingness of parents to use these devices to manage and monitor their child’s recovery.
Methods
This survey was reviewed and approved by our institutional Quality Improvement Committee (PRN 23625) and recognized by the Human Ethics Office at The University of Western Australia (RA/4/20/4629). Verbal consent was obtained from each participant by the researcher distributing the questionnaire.
A single-page paper questionnaire was developed addressing demographics (respondent age, child age, postcode), mobile device ownership (mobile phone type, mobile phone features, tablet device ownership), and attitudes (whether parents would be happy to be contacted and reply to the hospital by SMS, whether the cost of sending SMSs would prevent parents replying, whether parents would be happy to use a website or app on their mobile device to monitor their child’s recovery, the acceptability of SMS and app notification reminders, and whether the cost of mobile data would prevent parents from using a website or app).
The survey was conducted on five days (one of each weekday) over a two-week period between 15 and 26 January 2018 at our hospital (known at the time as Princess Margaret Hospital for Children). We asked the parents and carers of children receiving treatment at our institution (respondents) to complete our questionnaire. Potential respondents were identified from a broad range of hospital waiting areas in the emergency, medical imaging, and orthopaedics departments, the day surgery admission ward and general outpatient reception.
Questionnaires were scanned and coded using SDAPS (Scripts for data acquisition with paper-based surveys) 7 with each response independently verified by two researchers. Statistical analysis consisted of descriptive statistics. Analysis was performed with the R environment for statistical computing (version 3.3.2; R Foundation for Statistical Computing, Vienna, Austria) using Jupyter Notebooks (version 5.2.1; NumFOCUS, TX, USA).8,9
Postcodes were cross-referenced with remoteness areas using the Australian Standard Geographical Classification Remoteness Structure system. 10 When postcodes spanned multiple remoteness areas the remoteness area covering the largest proportion of that postcode was used. For questions with ‘Yes’, ‘Somewhat’ and ‘No’ options, only one response was permitted; when respondents answered with both ‘Yes’ or ‘No’ as well as ‘Somewhat’ their responses were counted as ‘Somewhat’, and when respondents answered with both ‘Yes’ and ‘No’ their response was discarded.
Results
Of 642 responses, three were blank except for demographic questions and were excluded, with 639 included for analysis. Demographics for respondents and their children are detailed in Table 1. Only two (0.3%) respondents did not own a mobile phone. Most owned an Apple iPhone (59.0%, 376) or an Android phone (39.4%, 251). A greater proportion had no tablet device (22.0%, 140) at home, with Apple iPad (59.0%, 376) being the most popular tablet.
Respondent demographics, mobile device ownership and features.
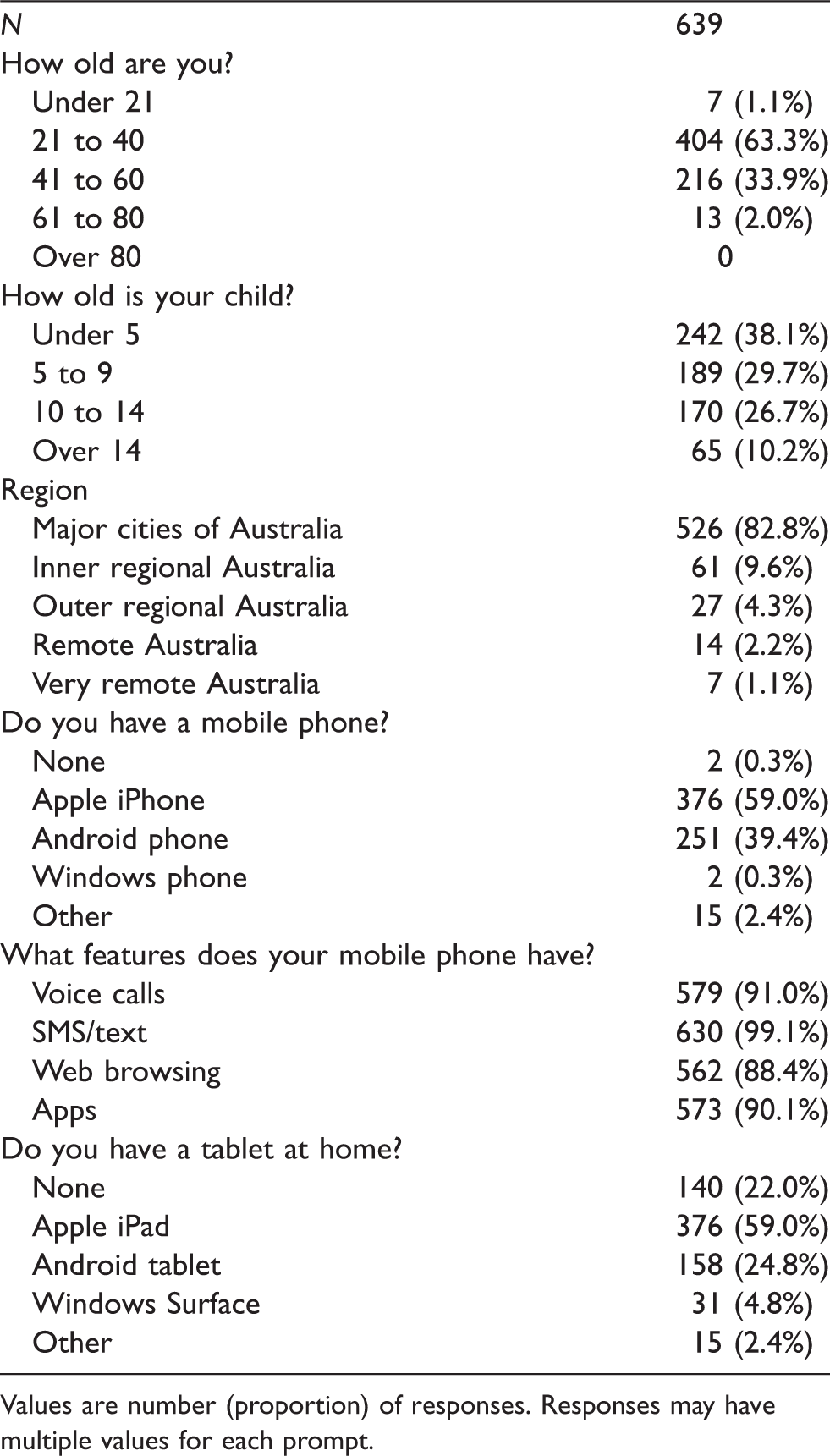
Values are number (proportion) of responses. Responses may have multiple values for each prompt.
Almost all respondents were happy to be contacted by the hospital regarding their child’s recovery (93.2%, 594), and to being contacted by SMS (94.3%, 599). Most were happy to receive medication reminders (73.3%, 464) or answer questions about their child’s recovery via SMS (80.3%, 508). Compared with SMS, respondents were less willing to use a website (59.9%, 379) or app (69.0%, 436) to log their child’s recovery (Table 2). A small number of respondents were concerned about the costs of replying to SMSs (9.5%, 61) and of mobile data (15.5%, 98).
Attitudes towards communicating with the hospital at home.
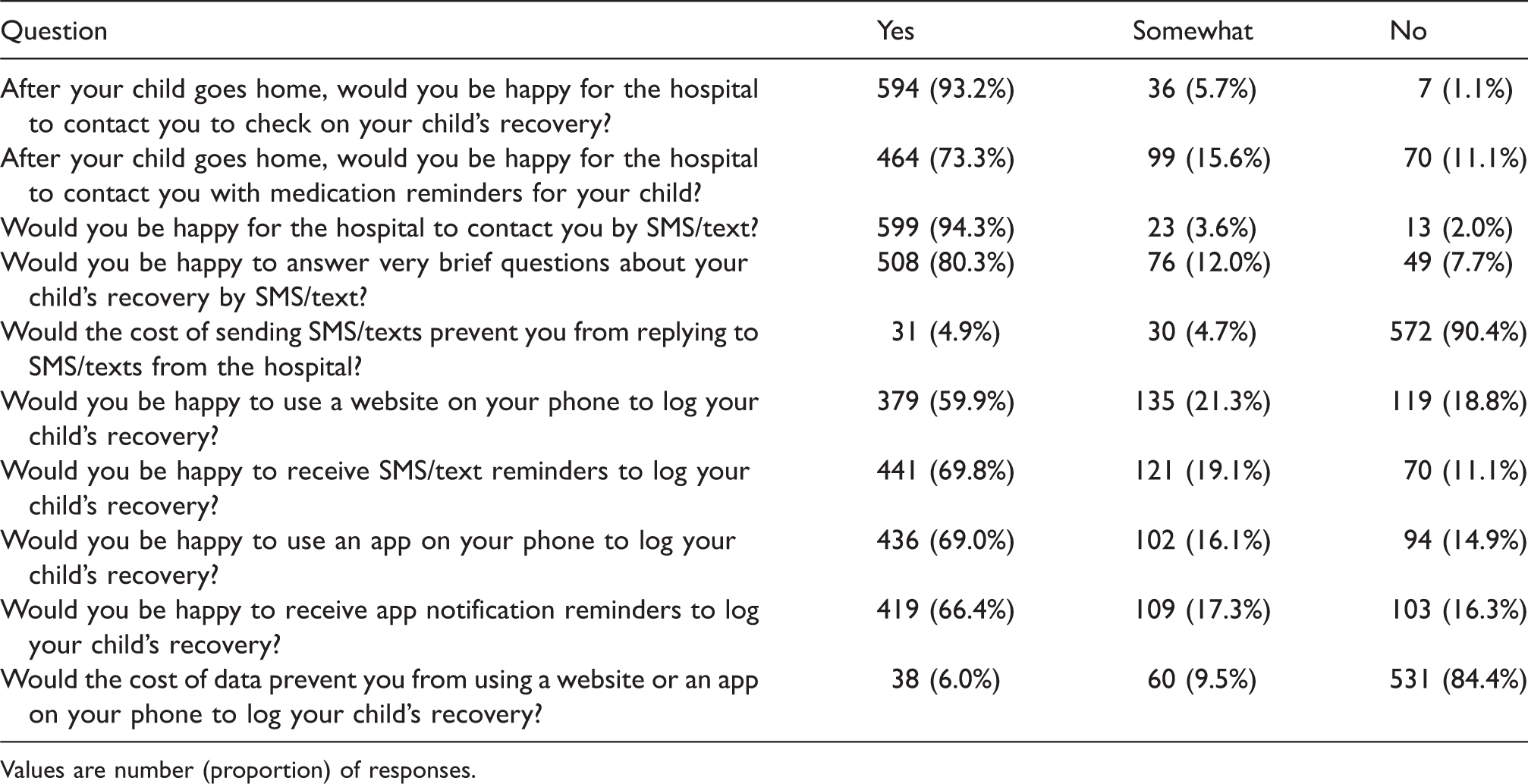
Values are number (proportion) of responses.
Discussion
This survey targeted the prevalence of mobile devices and attitudes regarding clinical and research follow-up in our patient population. Although we received some responses from regional and remote residents, most respondents were either metropolitan or inner regional residents, which is a reflection of our patient population.
As expected, mobile phones are effectively universal. We were also pleased to find positive attitudes towards using these devices in the clinical setting for follow-up and monitoring of children after discharge. The cost of responding to SMSs appears unlikely to significantly impact on willingness to participate in communication with the hospital. While our respondents were less enthusiastic about using websites or apps to monitor their child’s recovery, most parents and carers are still willing to use these tools. Significant rates of ‘Somewhat’ responses to questions about using a website or app might suggest that respondents are cautious about what exactly such a system might involve.
Any electronic follow-up solution would need to consider the different types of phones owned by parents and carers — particularly Apple iPhone and Android devices — or use a cross platform technology such as SMS messaging.
These results support piloting a SMS-based follow-up system as a replacement for our existing telephone-based follow-up after children leave hospital. We anticipate this will allow us to provide follow-up for a greater population of patients.
Footnotes
Acknowledgements
The authors wish to thank each of the families who took part in this survey, as well as our colleagues in the anaesthesia research team and across the hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BSvU-S was partly supported by the late Frank Callahan, the Perth Children’s Hospital Foundation and the Stan Perron Charitable Trust.