
Abstract
The transmuscular quadratus lumborum (TQL) block is one of the recently evolved myofascial blocks utilised in abdominal surgery. It involves injecting local anaesthetic into the fascial plane anterior to the thoracolumbar fascia. This block has previously been described with a transverse oblique paramedian approach at the L2 level in the sitting position. We describe a TQL block at the same level in the lateral position using a transverse posterolateral approach to provide analgesia for patients undergoing abdominal surgery. We elaborate on these two approaches of TQL block at the L2 level, in relation to the anatomy, sonoanatomy and technical aspects.
Keywords
Introduction
The transmuscular quadratus lumborum (TQL) block is one of the recently evolved myofascial blocks utilised in abdominal surgery. It involves injecting local anaesthetic (LA) into the fascial plane anterior to the thoracolumbar fascia (TLF). Børglum et al. first described the ultrasound-guided TQL block at the level of the fourth lumbar vertebra (L4). 1 It is also termed the anterior quadratus lumborum block because it involves injecting the LA at the anterior aspect of the quadratus lumborum (QL) muscle blocking dermatomes from T6 to L1. In comparison, to achieve sensory block covering the entire abdominal wall, a four point transversus abdominis plane block would be necessary. 2 Bilateral TQL can provide similar analgesia. Due to the presence of surgical drains at the flank level and poor visualisation of anatomical structures at this position, Dam et al. later used the transverse oblique paramedian (TOP) approach at the L2 level in the sitting position. 3 After encountering side-effects such as leg paresis with Børglum et al.’s L4 approach, we attempted TQL block at a higher level (L2 transverse process) with patients in the lateral position, using a transverse posterolateral (TPL) approach, in abdominal surgery.4–6 In this brief communication, we elaborate on these two approaches of TQL block at the L2 level, in terms of the anatomy, sonoanatomy and technical aspects.
Anatomy
Myofascial blocks around the QL plane are based on the anatomy of the TLF. It is a tubular connective tissue structure formed by the binding aponeuroses and fascia layers, which, by enveloping the back muscles, connects the anterolateral abdominal wall with the lumbar paravertebral region (Figure 1). 7 On its medial side, the TLF is attached to the thoracic and lumbar vertebrae, and continues cranially as the endothoracic fascia. The TLF divides into three layers (anterior, middle and posterior) around the muscles of the back. The posterior layer is posterior to the erector spinae muscles; the middle layer is sandwiched between the erector spinae and QL muscle (and is thus posterior to the QL); the anterior layer is anterior to the QL muscle. The anterior layer also blends medially with the fascia of psoas major and blends laterally with the transversalis fascia. Injection between the anterior layer and QL can spread cranially under the lateral arcuate ligament to the endothoracic fascia and reach the lower thoracic paravertebral space posterior to the endothoracic fascia. 8
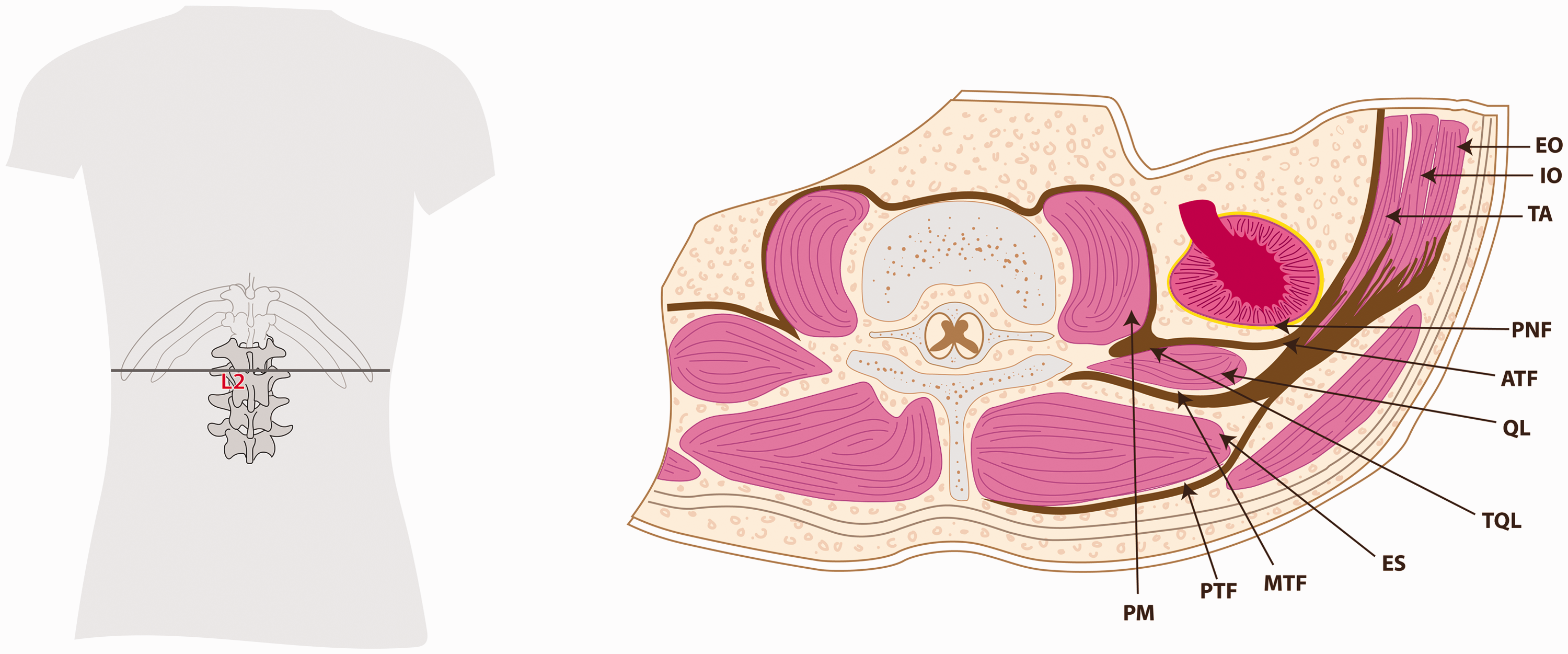
The anatomy of the thoracolumbar fascia at L2. EO: external oblique; IO: internal oblique; TA: transversus abdominis; PNF: perinephric fascia; ATF: anterior thoracolumbar fascia; QL: quadratus lumborum muscle; TQL: site of transmuscular quadratus lumborum block at L2; ES: erector spinae; MTF: middle thoracolumbar fascia; PTF: posterior thoracolumbar fascia; PM: psoas muscle.
Technical description
TPL TQL approach
This approach can be performed pre-, intra- and postoperatively. We focus on block performance at the end of the surgical procedure before extubating the patient with the therapeutic aim of enhancing postoperative analgesia. 5 It can be done unilaterally or bilaterally depending on the type of the incision. It is performed in the lateral decubitus position with the block side upwards. On the lower side a wedge is placed between the rib cage and the iliac crest to make the QL muscle prominent. To improve visualisation, anaesthetic assistants would need to retract the rib cage and the iliac crest to increase the gap. A curved low frequency probe 2–5 MHz is placed transversely between the iliac crest and the costal margin in the posterior axillary line. The structures visualised are the abdominal muscles, psoas muscle, peritoneum, kidney and QL muscle (Figure 2). After identifying the QL an 18 gauge Tuohy needle (with the tip pointing upwards) is introduced in plane and medial to the transducer probe and advanced posterior to anterior through QL muscle. Hydrodissection is carried out while the needle is above the L2 transverse process till it passes through the QL muscle. This will help to identify the muscle plane and reach the anterior TLF. The kidney is very close to the QL muscle, which is separated from it by perinephric adipose tissue and the posterior layer of renal fascia. The LA is injected in the myofascial plane between the QL muscle and the anterior TLF, close to the psoas muscle, where a tactile feel of layer penetration may also be appreciated. The hydrodissection with the Tuohy needle may avoid entry into the peritoneal cavity or perinephric area. After a test dose of saline 5 mL, 0.5% ropivacaine 20 mL is given in 5 mL aliquots after aspiration. This is followed by the catheter insertion.
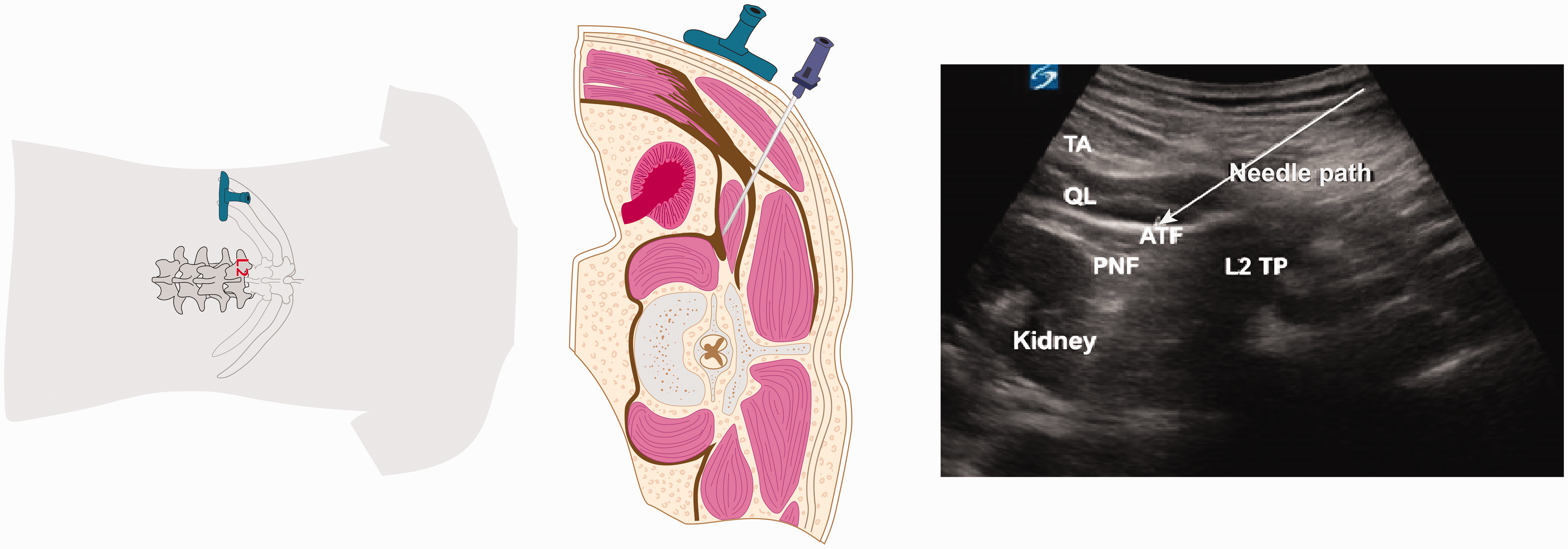
TPL (transverse posterolateral) TQL L2 approach showing transverse probe placement, in plane needle placement and ultrasound image. TA: transversus abdominis; QL: quadratus lumborum muscle; ATF: anterior thoracolumbar fascia; PNF: perinephric fascia; L2 TP: transverse process of L2; TQL: transmuscular quadratus lumborum.
In our view, the risk of puncture of intra-abdominal structures such as the kidney can be minimized by careful tactile feel of fascia, visualisation of the needle tip, the use of a blunt Tuohy needle and hydrodissection. We believe the risk is likely to be reduced by taking these measures.
Personal observations
Performing TQL block at a higher level (L2) will minimize the chance of lower lumbar nerve root blockade (femoral nerve). These roots are likely to get blocked if the injection point is close to the psoas muscle at L4 level, which is in close proximity to where the nerve roots join to form the femoral nerve. Hydrodissection above the L2 transverse process to the anterior TLF can avoid entry into the peritoneal cavity or perinephric area, thus preventing damage to the vital structures in the vicinity. Use of a blunt Tuohy needle and the tactile feel of fascial click may be a safer technique than the use of a sharp needle.
TOP TQL approach
This is a TOP approach of the TQL block, with the patient in a sitting position. The original sources used the hypoechoic shadow of the transverse processes as the primary proxy endpoint marker for injection. 3 The cephalad border of the iliac crest and the spinous processes of the lumbar vertebral column are palpated and marked on the skin. A curvilinear transducer 2–5 MHz is placed with a transverse oblique and paramedian orientation approximately 3 cm lateral to the L2 spinous process (Figure 3). The transducer is first shifted cephalad or caudad to identify the L2 transverse process and the adjoining QL muscle. The needle is then inserted in plane from the medial end of the transducer and advanced in plane laterally to enter the interfascial plane between the QL and psoas major muscles and LA is injected.
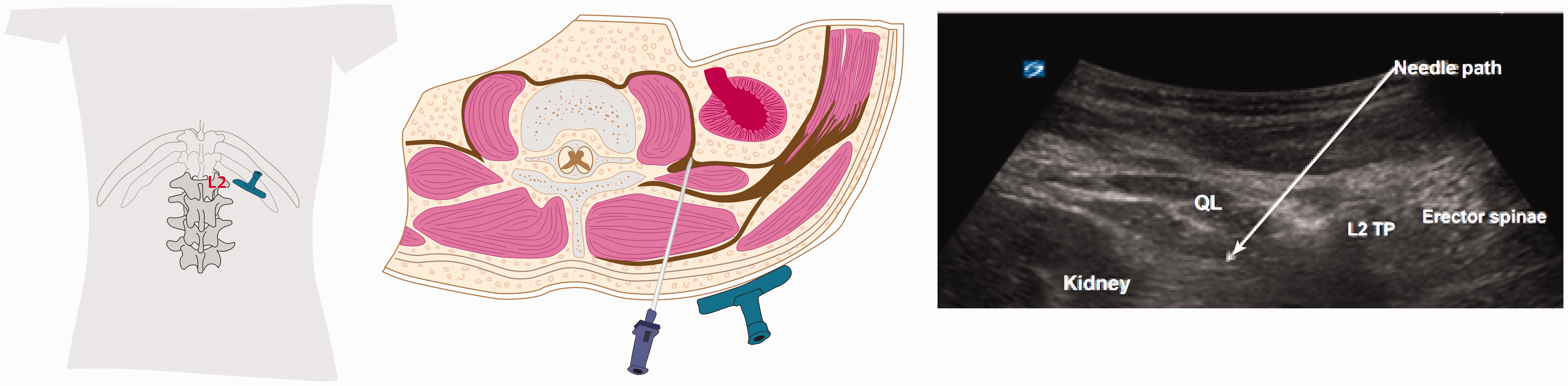
TOP (transverse oblique paramedian) TQL L2 approach showing transverse oblique probe placement, in-plane needle placement and ultrasound image. TQL: transmuscular quadratus lumborum; QL: quadratus lumborum; L2 TP: transverse process of L2.
Discussion
This short communication describes two recently developed variations of the TQL approach at the L2 level, with illustrated anatomy and related probe and needle positions to assist in understanding the sonoanatomy and performance of these blocks in abdominal surgery.
A comparison between the TPL and TOP approaches is given in Table 1. It should be noted that the endpoints in both approaches are similar; i.e. the myofascial plane between the QL muscle and the anterior TLF, close to the psoas muscle. Dam et al., using the TOP approach in a cadaver model, reported medial spread of dye limited to the lateral part of the psoas fascia and cranial spread into the thoracic paravertebral space 8 . It was noted in this cadaver study that injectate administered at the myofascial QL plane at L2 level could reach lower thoracic up to the T10 thoracic paravertebral space and T9–12 ventral rami. There was no spread of injectate into the psoas major muscle or the lumbar plexus, and a consistent spread of injectate into the thoracic paravertebral space and the thoracic sympathetic trunk was noted. This could possibly reduce both somatic and visceral pain although, as yet, data are limited in this regard.
Comparison of transverse posterolateral and transverse oblique paramedian approaches to transmuscular quadratus lumborum blockade.
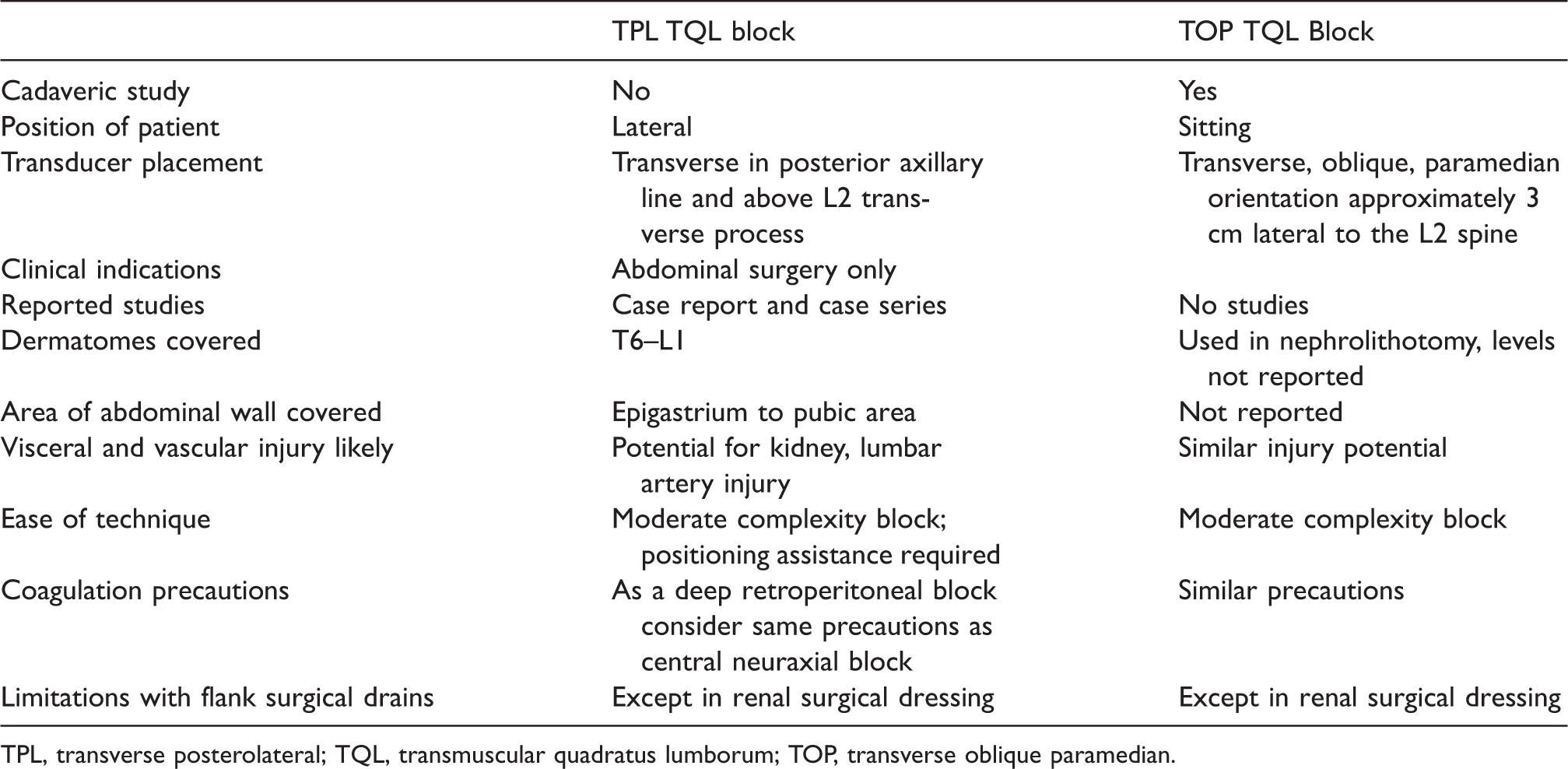
TPL, transverse posterolateral; TQL, transmuscular quadratus lumborum; TOP, transverse oblique paramedian.
This, and the favourable results reported in recent limited case series in major abdominal surgery, demonstrating cranial spread, without the occurrence of lumbar root blockade,4–6,9 make this approach appropriate in intra- and retroperitoneal abdominal surgery, either as a single-sided (e.g. nephrectomy) or double-sided (e.g. bowel surgery) block.
The needle skin entry points differ between a more posteromedial (TOP) and posterolateral (TPL) approach. Also, the patient position differs with Dam et al. advocating a sitting position and we suggest a lateral position with a wedge under the patient to enable better access.
Both, in their early publications, suggest administering the block postoperatively. However, from a pain management point of view, having a regional anaesthetic block in situ during surgery will be more advantageous. Other advantages include being able to use the block in patients who are unable to sit up, such as whilst anaesthetised or immediately postoperatively in the post-anaesthesia care unit or intensive care unit. From a patient comfort and safety perspective, inserting the catheter(s) prior to surgery would be preferable to doing so either with the patient sitting up in the post-anaesthesia care unit or moving the patient to one lateral position, and subsequently to the other, while still anaesthetised.
Unfortunately, no major clinical studies have been reported on this approach. In a case series of TPL for abdominal surgeries, a dermatomal spread as high as T6 was achieved. 6 It is unclear to what extent this technique covers intra-abdominal visceral pain. A randomized trial is underway in our institution exploring its use during open major abdominal surgery. Till now, there has been only a single case series comparing the needle position at the anterior aspect of the QL muscle, between the L2 and L4 level approach 6 . Anecdotally we have not observed lower limb weakness, but this was not formally studied. LA spread to the lumbar plexus is a possibility. We found no other adverse events at the L2 level. However, data is limited on the differences between these approaches 6 . Further studies should investigate the role of TQL in open upper gastrointestinal and colorectal surgeries using TQL at L2 level (higher) and for pelvic surgery at lower (L3–L4) level.
In conclusion, based on anatomical considerations and the limited clinical data available, both ultrasound-guided TQL approaches (TPL and TOP) at L2 level have theoretical advantages. However, these would need to be confirmed in prospective studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.