
Abstract
Bilateral quadratus lumborum blockade (QLB) using ultrasound guidance has been introduced as an abdominal truncal block to improve postoperative analgesia and quality of recovery (QoR) after abdominal surgery, but efficacy remains controversial. The primary aim of this study was to evaluate the efficacy of posterior QLB on the postoperative QoR, and secondarily to evaluate postoperative pain after gynaecological laparoscopic surgery (LS). This study was a single-centre randomized controlled trial. QLB group patients underwent bilateral posterior quadratus lumborum injections with 25–30 mL of 0.25% levobupivacaine after induction of general anaesthesia; the control group underwent no block. Both groups were administered fentanyl-based intravenous patient-controlled analgesia postoperatively. The postoperative QoR was measured using the Quality of Recovery 40 (QoR-40) questionnaire score; postoperative pain was evaluated using the visual analogue scale (VAS) and the cumulative postoperative fentanyl dose. Thirty-one and 29 patients were randomised to the QLB and control groups, respectively. The intraoperative remifentanil dosage was significantly less in the QLB group. The median (interquartile range) for the QoR-40 score was not different between the groups: 154 (133–168) in the QLB group and 158 (144–172) in the control group. There were no statistically significant differences in secondary outcome variables. Single-shot QLB did not improve the QoR or postoperative pain in patients managed by multimodal analgesia after gynaecological LS.
Introduction
Bilateral quadratus lumborum blockade (QLB) using ultrasound guidance was introduced as an abdominal truncal block by Blanco in 2007. Since then, several case reports and a randomized controlled trial have demonstrated that QLB is effective in providing pain relief after various abdominal surgeries,1–4 although no study has examined the efficacy of QLB in terms of the postoperative quality of recovery (QoR).
Therefore, this study was conducted to evaluate the efficacy of posterior QLB on the postoperative QoR using the Quality of Recovery 40 (QoR-40) questionnaire in patients who underwent major gynaecological laparoscopic surgery (LS). Secondary objectives included assessment of postoperative analgesia as measured by postoperative visual analogue scale (VAS) pain score at rest, cumulative fentanyl dose, and the numbers of patients who used rescue non-steroidal anti-inflammatory drugs (NSAIDs) and antiemetics postoperatively. We hypothesized that QLB would improve the QoR and reduce pain after major gynaecological LS.
Methods
This study was approved by the Ethics Committee of Yokohama City University (ID: B160204004) on 24 February 2016 and registered with the University Hospital Medical Information Network Clinical Trials Registry (ID: UMIN000024161, https://upload.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000024693). The first patient recruitment started on 1 July 2016 with written informed consent.
Our single-centre randomized controlled trial was conducted between July 2016 and March 2017. Adult patients (≥20 years of age) with an American Society of Anesthesiologists physical status of 1 or 2 who were scheduled for elective gynaecologic LS were enrolled in our study. The exclusion criteria were cognitive dysfunction, obesity (body mass index ≥35 kg/m2), renal dysfunction (estimated glomerular filtration rate ≤50), coagulopathy, a drug allergy to NSAIDs, paracetamol or the local anaesthetic, a gastric ulcer, pregnancy, and regular opioid or steroid use.
Patients were allocated to the control group or the QLB group by using stratified block randomization. The type of surgery was used as a stratification factor as previous work had indicated that visceral pain after total laparoscopic hysterectomy or total laparoscopic modified radical hysterectomy was greater than other types of gynaecological LS, related to the effects of pelvic dissection, more tissue manipulation and longer operating time. 5 The randomization scheme was generated using a website (http://www.randomization.com) by an anaesthesiologist who was not involved in the study. No patient was administered premedication on the ward. Standard monitoring was connected on entry to the operating room. General anaesthesia was induced with propofol and fentanyl 3 µg/kg, followed by rocuronium to facilitate endotracheal intubation. All patients were administered dexamethasone 8 mg intravenously during induction to prevent postoperative nausea and vomiting. After general anaesthesia induction, QLB group patients underwent bilateral posterior QLB under ultrasonography guidance with 0.25% levobupivacaine 30 mL on each side. Three regional anaesthesiologists experienced in peripheral nerve blocks performed QLB or provided guidance. QLB was performed with a 22-gauge 80 mm epidural needle (Pelican®, B. Braun, Melsungen, Germany) utilising ultrasonography (Edge®, FUJIFILM-Sonosite, Tokyo, Japan) with a convex probe (2–5 MHz). With the patient in the supine position, we placed the ultrasonic transducer transversely at the level of the anterosuperior iliac spine first and slid it toward the cephalad side until the three abdominal wall muscles were clearly identified, as in a transversus abdominis plane (TAP) block. Next, we moved the transducer posteriorly and identified the quadratus lumborum muscle underneath the internal oblique muscle. Injections were performed dorsal to the quadratus lumborum muscle by hydrodissecting the lumbar interfascial triangle using an in-plane approach. Patients who weighed less than 50 kg were administered 0.25% levobupivacaine 25 mL on each side. Control group patients underwent no block. Anaesthesia was maintained with desflurane, remifentanil and rocuronium. The intraoperative medication dosage, except for fentanyl, was determined by the anaesthesiologist in charge. At the termination of pneumoperitoneum, all patients were administered flurbiprofen 50 mg and fentanyl 2 μg/kg intravenously, followed by fentanyl-based intravenous patient-controlled analgesia (IV-PCA). No other fentanyl was administered intraoperatively. The fentanyl IV-PCA was programmed to deliver a basal infusion of 10 µg/h and a bolus dose of 10 µg on demand with a lockout interval of 10 min. Sugammadex was administered to reverse the neuromuscular blockade. All patients were administered fentanyl IV-PCA for 24 h postoperatively. Patients were instructed to press the IV-PCA button when they experienced any pain. When the VAS score was higher than 50 mm even with the use of IV-PCA, rescue NSAIDs (flurbiprofen or loxoprofen) were administered.
The primary outcome of the study was the QoR evaluated using the QoR-40 questionnaire score on postoperative day 1. We used the Japanese version of the QoR-40, which has the characteristics of acceptable validity, reliability and responsiveness in clinical practice in Japan. 6 Patients completed the questionnaire themselves. Pain was assessed by using the VAS at rest at 2, 6 and 24 h after surgery. Staff undertaking this assessment were blinded to patient group allocation. The cumulative fentanyl dose, numbers of patients who used rescue NSAIDs and antiemetics, the length of stay in hospital and other complications were documented.
Sample size calculation and statistical analysis
A sample size of 24 patients per group was needed to provide 80% power at a target significance level of 0.05 (two-sided) to detect a 10-point difference in QoR-40 scores between the two groups (G*Power 3.1.9.2; Dusseldorf, Germany). A 10-point difference represents a clinically relevant improvement in the QoR in patients after anaesthesia and surgery. 7 We estimated an overall standard deviation of 12 points based on previous studies.8,9 To account for dropouts, 60 subjects were randomized.
Data were entered as numerical or categorical, as appropriate. Descriptive statistics were recorded for each variable including the minimum, maximum, range, mean, median and interquartile range (IQR). Data were analysed using the unpaired t test or the Mann–Whitney U test for continuous data, and Fisher’s exact test for categorical data. The 95% confidence interval of the median was analysed using bootstrap methods.
Results
Sixty-four patients were enrolled during the study period. Figure 1 shows the Consolidated Standards of Reporting Trials (CONSORT) flowchart for patient recruitment. Twenty-nine patients were randomized to the control group and 31 patients were randomized to the QLB group. Two patients in each group were excluded because of protocol violations (patients who underwent a conversion to laparotomy and those lost to follow-up).
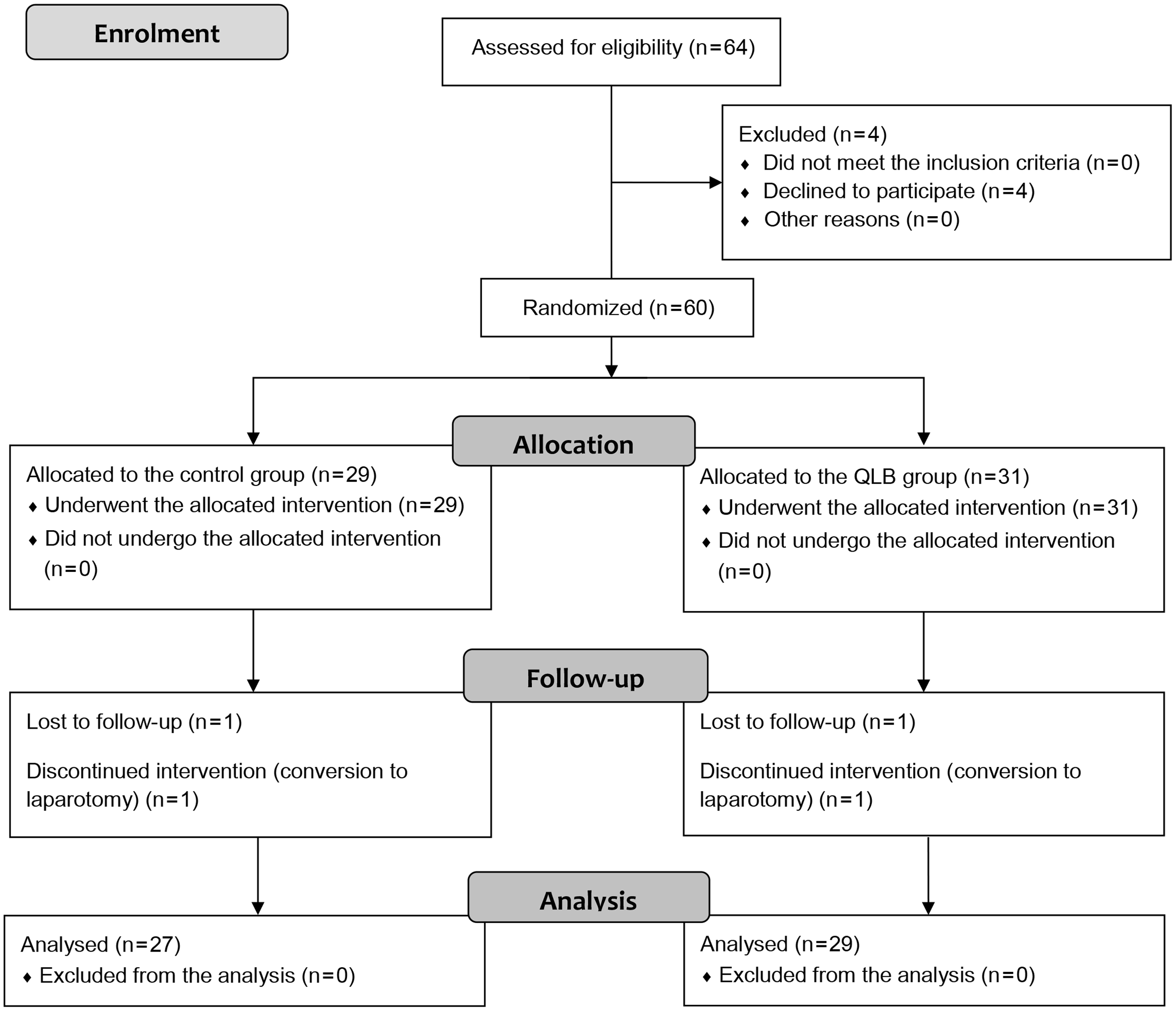
CONSORT flowchart.
There were no statistically significant differences between the groups in the patients’ demographics, type of surgery, or operation duration (Table 1). We defined the anaesthesia preparation time as the time from the beginning of anaesthesia to the completion of preparation of anaesthesia, including intubation, line placement, and block performance in the QLB group. The anaesthesia preparation time was significantly longer in the QLB group compared to control by several minutes (mean 18 (standard deviation, SD, 8.7) min versus 27 (6.6) min, P < 0.0001) however, total duration of anaesthesia was not significantly different (Table 1). The intraoperative remifentanil dose was significantly lower in the QLB group (P = 0.0082, Table 1).
Demographic and perioperative patient data.
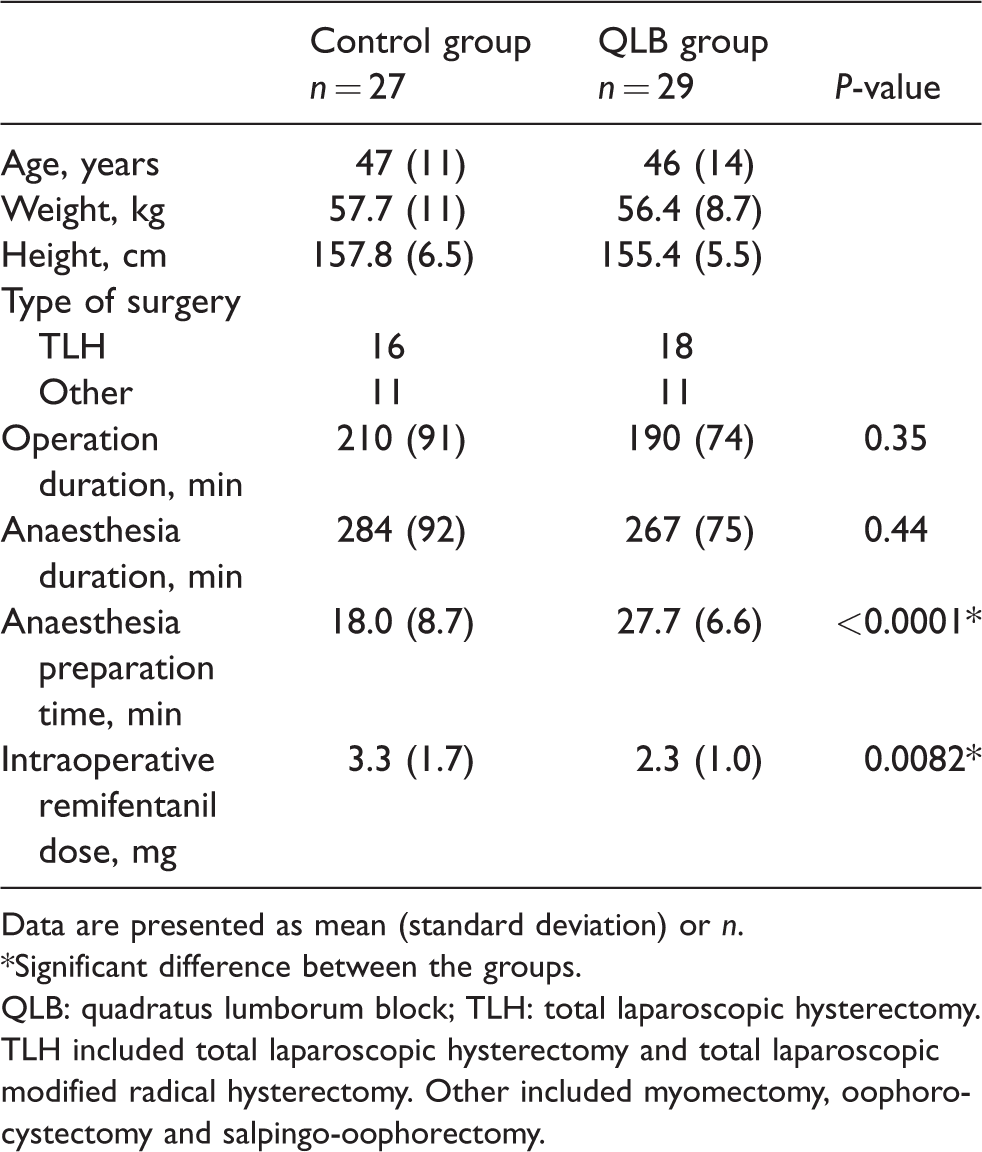
Data are presented as mean (standard deviation) or n.
*Significant difference between the groups.
QLB: quadratus lumborum block; TLH: total laparoscopic hysterectomy. TLH included total laparoscopic hysterectomy and total laparoscopic modified radical hysterectomy. Other included myomectomy, oophorocystectomy and salpingo-oophorectomy.
Primary outcome: QoR on postoperative day 1
The primary outcome, the QoR-40 score, was not statistically different between the groups. The median (IQR) QoR-40 score was 154 (133–168) in the QLB group and 158 (144–172) in the control group (P = 0.361, Figure 2).
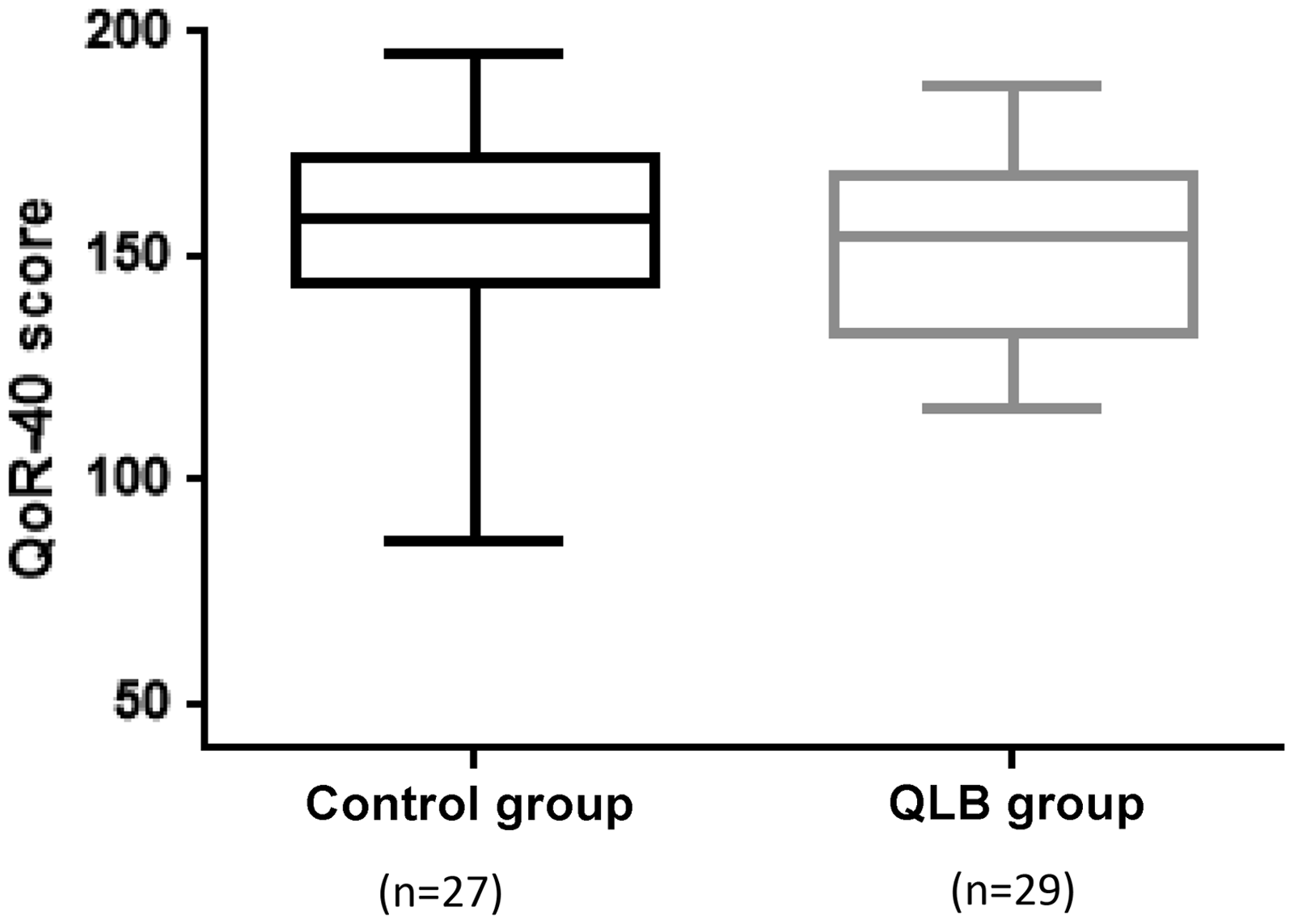
QoR-40 score at 24 h after surgery. The median (interquartile range) for the QoR-40 score was 158 (144–172) in the control group and 154 (133–168) in the QLB group. The median difference (95% confidence interval) = −6.7 (−17.1 to 6.3), P = 0.361 (bootstrap methods).
Secondary outcome: postoperative analgesia and complications
After surgery, no difference was observed in the outcome or measurement values. The cumulative fentanyl dose and numbers of patients who used rescue NSAIDs and antiemetics were not statistically significantly different between the two groups (Table 2). Five patients in the QLB group experienced numbness in their lower limbs at awakening; no patient in the control group experienced numbness. No other complication was observed in either group.
Outcome measures.
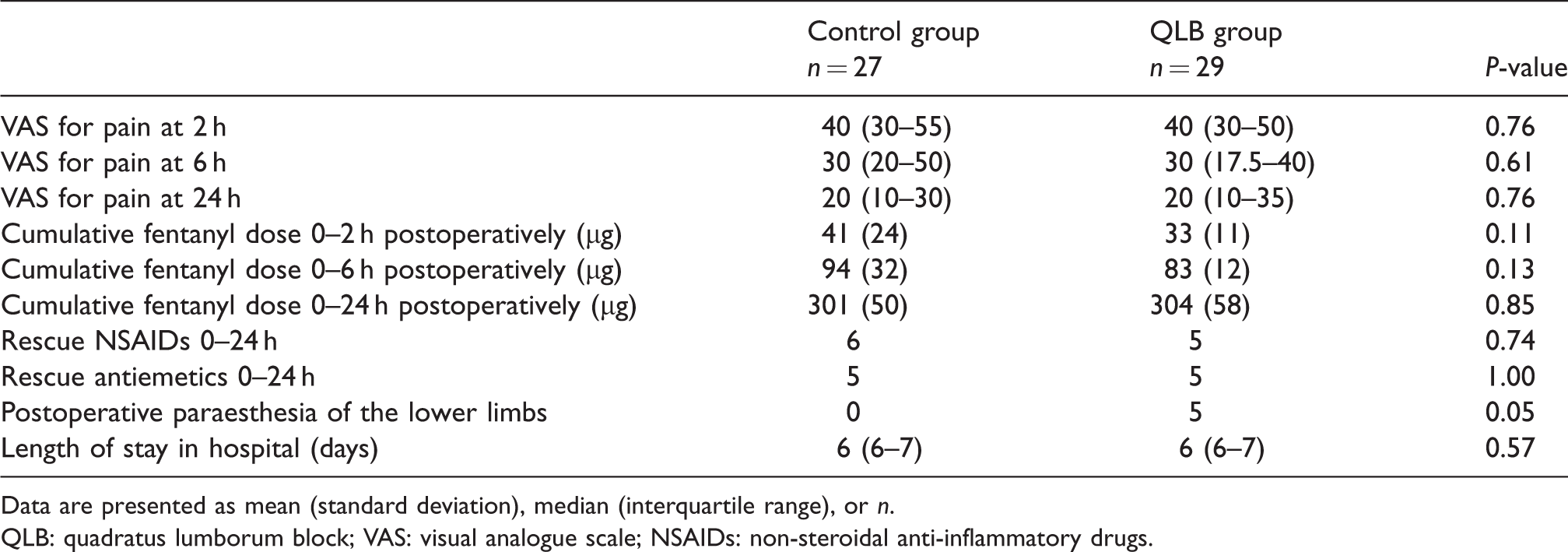
Data are presented as mean (standard deviation), median (interquartile range), or n.
QLB: quadratus lumborum block; VAS: visual analogue scale; NSAIDs: non-steroidal anti-inflammatory drugs.
Discussion
This study is the first to evaluate the efficacy of posterior QLB on the postoperative QoR after major gynaecological LS. It showed that QLB did not improve postoperative QoR in these gynaecological patients. Previous studies which have examined the efficacy of abdominal truncal blockade have shown improvement in postoperative QoR after gynaecological LS.8–10 However, these studies evaluated the effects using TAP blocks. QLB has been demonstrated to provide a superior postoperative analgesic effect compared to TAP block, in that it allows extended analgesia duration and reduces supplemental analgesia consumption.11,12 Therefore, we thought QLB could improve QoR after these laparoscopic surgeries, at least in part, as a consequence of improved postoperative analgesia. In our study, we could not demonstrate an improvement in postoperative analgesia using single-shot posterior QLB and this may have been a contributing factor in the failure to demonstrate improved recovery.
Pain after gynaecological LS includes somatic pain related to surgical trauma of the abdominal wall, and visceral pain related to peritoneal trauma and irritation. 13 Two studies have demonstrated the superior postoperative analgesic efficacy of QLB after gynaecological laparoscopic surgeries;12,14 however, both studied patients who underwent laparoscopic ovarian surgery, laparoscopic enucleation myomectomy, or laparoscopic oophorocystectomy. Postoperative visceral pain associated with these surgeries may be considered relatively weak. In contrast, more than half of the patients in our study underwent total laparoscopic hysterectomy, which is associated with strong visceral pain, 5 offering a possible basis as to why our results differed from those of previous studies. In addition, it is necessary to consider the persistence of the analgesic effect of QLB. In this study, we did not use a continuous block technique. Our posterior QLB comprised a single injection before surgery. QLB has been reported to yield a prolonged pain-free state (>24 h) compared to the TAP block,11,12 so we did not employ continuous QLB in our study. Intraoperative remifentanil dose was significantly smaller in the QLB group. Although this was not a blinded study in that the intraoperative remifentanil dose was determined by the attending anaesthesiologist, the reduction could be the result of an analgesic additive action of QLB during anaesthesia. The trend of lower fentanyl requirements during the short period after surgery might also be a result of QLB.
A previous meta-analysis, 15 which demonstrated the analgesic efficacy of TAP block after LS, excluded studies with concurrent use of an alternative multimodal analgesia regimen. However, postoperative analgesic strategy is currently undergoing a shift to multimodal analgesia. Our study also used multimodal analgesia postoperatively, comprising continuous infusion of fentanyl supplemented with rescue analgesic NSAIDs. We suspect that the efficacy of truncal blockade might be different under postoperative multimodal analgesia.
Considering the time consumption and economic aspects, the anaesthesia preparation time was significantly longer in the QLB group without advantages to the QoR-40. Avoiding QLB in patients undergoing these surgeries with postoperative multimodal analgesia may save time and money.
As a side-effect, five patients in the QLB group felt numbness in their lower limbs at awakening, whereas no patient in the control group experienced numbness. In all five patients, the numbness improved by 24 h after surgery. When we measured the QoR-40 24 h after surgery, as all patients showed improved numbness, this could not be detected as a score in the QoR-40. Sensory block and motor weakness after posterior QLB have been reported previously; 16 therefore, we suspect that QLB may have been the cause of numbness. There was no complication related to muscle weakness, and in particular no patient experienced a fall as a result of lower limb weakness, although it should be noted that patients were not allowed to stand up or walk until the next day according to the protocol in our institution. The mechanism of action of QLB is not entirely clear and the spread of local anaesthetic is quite varied according to technique. 17 Hence, clinicians should be aware of lower leg muscle weakness and sensory changes during post-anaesthesia care after performing QLB, and patients should be informed of the possibility of both numbness and weakness as potential side-effects as part of their preoperative consent.
Some limitations should be considered in this study. First, this was not a blinded study. This open-label approach may affect anaesthesia care and postoperative analgesia management. Secondly, it is a small study which limited the opportunity for post hoc subgroup analysis based on surgical type, however future studies may benefit from the prospective incorporation of subgroups based on surgical complexity.
Conclusion
In summary, women receiving multimodal postoperative analgesia after major gynaecological LS showed no improvement in QoR assessed by QoR-40, or in analgesia following bilateral single-shot QLB performed immediately after induction of general anaesthesia. Further research is required to help clarify the role of QLB on QoR especially in women undergoing more complex gynaecological LS.
Footnotes
Acknowledgement
The authors thank M. Kikuchi for assistance in performing the blocks. We also acknowledge the assistance of the nursing staff in the obstetric and gynaecological ward of Yokohama City University Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.