
Abstract
Strategies to reduce the adverse environmental costs of anaesthesia include choice of agent and fresh gas flows. The current preferences of Australian and New Zealand anaesthetists are unknown. We conducted a survey of Australian and New Zealand anaesthetists to determine the use of volatiles, nitrous oxide and intravenous anaesthesia, lowest fresh gas flow rates, automated end-tidal volatile control, and the rationales for these choices. The survey was answered by 359/1000 (36%), although not all questions and multiple responses within single questions were answered by all respondents. Sevoflurane was preferred by 246/342 (72%, 95% confidence interval (CI) 67%–77%), followed by propofol, 54/340 (16%, 95% CI 12%–20%), desflurane 39/339 (12%, 95% CI 8%–16%) and isoflurane 3/338(1%, 95% CI 0–3%). When asked about all anaesthetics, low-risk clinical profile was the most common reason given for using sevoflurane (129/301 (43%, 95% CI 37%–49%)), reduced postoperative nausea for propofol (297/318 (93%, 95% CI 90%–96%)) and faster induction/awakening times for desflurane (46/313 (79%, 95% CI 74%–83%)). Two-thirds (226/340 (66%, 95% CI 61%–71%)) of respondents used nitrous oxide in 0–20% of general anaesthetics. Low fresh gas flow rates for sevoflurane were used by 310/333 (93%, 95% CI 90%–95%) and for 262/268 (98%, 95% CI 95%–99%) for desflurane. Automated end-tidal control was used by 196/333 (59%, 95% CI 53%–64%). The majority of respondents (>70%) preferred sevoflurane at low flows. These data allow anaesthetists to consider further whether changes are required to the choices of anaesthetic agents for environmental, financial, or any other reasons.
Introduction
The environmental and financial impacts of anaesthesia, including those of anaesthetic gases, are increasingly recognised.1–3 Low-flow anaesthesia (fresh gas flow (FGF) rates less than two litres per minute) 4 is becoming increasingly popular with its environmental and economic benefits.5–8 A 2015 survey of anaesthetists in France indicated that 50% preferred sevoflurane, 24% desflurane and 17% propofol, with more than 90% using all volatiles at less than two litres/minute. 9 The use of nitrous oxide (N2O) in all Scandinavia was surveyed to fall to 12% of general anaesthetic cases by 2013, with the majority of anaesthetists aware of N2O’s global warming and ozone-depleting capacity. 10 In contrast, a 2016 USA survey with 2100 respondents found that few American anaesthesiologists considered environmental concerns when choosing anaesthetic agents. 11
Recent studies in Victoria, Australia investigated the volumes of inhalational agents used, 12 and the benefits of low-flow anaesthesia, particularly the use of automated end-tidal volatile monitoring. 7 In Australia and New Zealand, however, it was unclear what anaesthetic agents were being used. As there are financial and environmental effects of anaesthetic gas use we undertook a survey to identify the types of general anaesthetic agents being used and why.
We surveyed the opinions of Fellows of the Australian and New Zealand College of Anaesthetists (ANZCA) on their choice of, and reasons for, general anaesthetic agents, and the use of low-flow anaesthesia. We were particularly interested in knowing whether anaesthetists considered environmental and financial factors when making choices about what general anaesthetic agent they used. We asked the following questions:
What is the relative usage of, and reasons for, different general anaesthetic agents and how does this surveyed usage compared with actual usage obtained separately? What is the frequency of the use of N2O in general anaesthesia? What is the lowest tolerated maintenance FGF and why? How often is automated end-tidal volatile control used? Are there educational opportunities to reduce the environmental and financial impact of anaesthesia, including increasing the use of low FGF anaesthesia?
Methods
We obtained prospective ethical approval for our survey from the Western Health Human Research Ethics Committee, Melbourne, Australia (QA 2016.97). Initially we piloted the survey with ten Western Health anaesthetists, finding that the questions and the duration of the survey appeared reasonable. Consent was implied with survey completion. There were seven ‘best answer’ questions, three ‘multiple answers’ questions, and one ‘open-ended’ question (see Appendix 1, available online). Questions 1 to 3 collected demographic data (age, gender, public/private, metropolitan/rural). Questions 4 to 7 enquired about anaesthetic agent choice (volatiles, N2O and propofol). Questions 8 and 9 asked about low FGF practice, including what proportion of anaesthetists used low FGF sevoflurane given product manufacturer warnings 13 and, on the contrary, evidence that low FGF sevoflurane delivery is safe. 14 Question 10 asked about the use of end-tidal automated volatile concentration, and question 11 asked for further comments.
We surveyed with the online platform Survey Monkey (Portland, OR, USA). ANZCA surveys were aimed to take a sample size large enough to give adequate ANZCA Fellows’ representation. This standard ANZCA survey sample size of a minimum of 500 Fellows was based on the following assumptions: the acceptable margin of error (amount of inherent error from random sampling or the anticipated precision of the estimate) was ±5% for a proportion; ANZCA has 4500 Fellows; the response rate would be 60%; and the response distribution (the proportion that agree:disagree) was 50:50. 15 ANZCA representatives indicated that the 2017 population of active anaesthetic Fellows across Australia and New Zealand was 5310 (increased from 4482 Fellows in 2014). 16 The survey link was e-mailed to 1000 randomly selected ANZCA Fellows in August 2017, and reminder emails were sent a fortnight later.
Similar to the 2015 survey of anaesthetic volatile gas use in France by Benhamou et al. 9 we compared our survey data with actual volatile anaesthetic use. We obtained data of the total actual 2017 Australian (only) national anaesthetic gas use from the company IQVIA, 17 a multinational company that buys and sells healthcare information. The Australian Commonwealth Scientific and Industrial Organisation (CSIRO) paid for these data as part of an ongoing study of atmospheric anaesthetic gases. IQVIA does not collect N2O use. Propofol use was not collected as this would include all healthcare use.
We calculated proportions and percentages for all our quantitative results. For proportions that directly addressed our primary questions, we estimated 95% confidence intervals (CIs). We assumed normality and that our respondents were a random sample of all ANZCA Fellows. CIs were calculated using R statistical software (the R Foundation) (see Appendix 2, available online). For this survey research, and in the absence of a formal CONSORT (Consolidated Standards of Reporting Trials) diagram, we followed the advice of Story et al. 18
Results
Online responses for our August 2017 survey of choice of general anaesthetic were received from 359/1000 (36%) ANZCA Fellows. Not all of the 359 respondents answered all 11 questions; however, the lowest response rate was 326/359 (91%). The gender and age ratios of our respondents reflected the ANZCA Fellowship (Table 1).
Age and gender of survey respondents and all ANZCA Fellows.
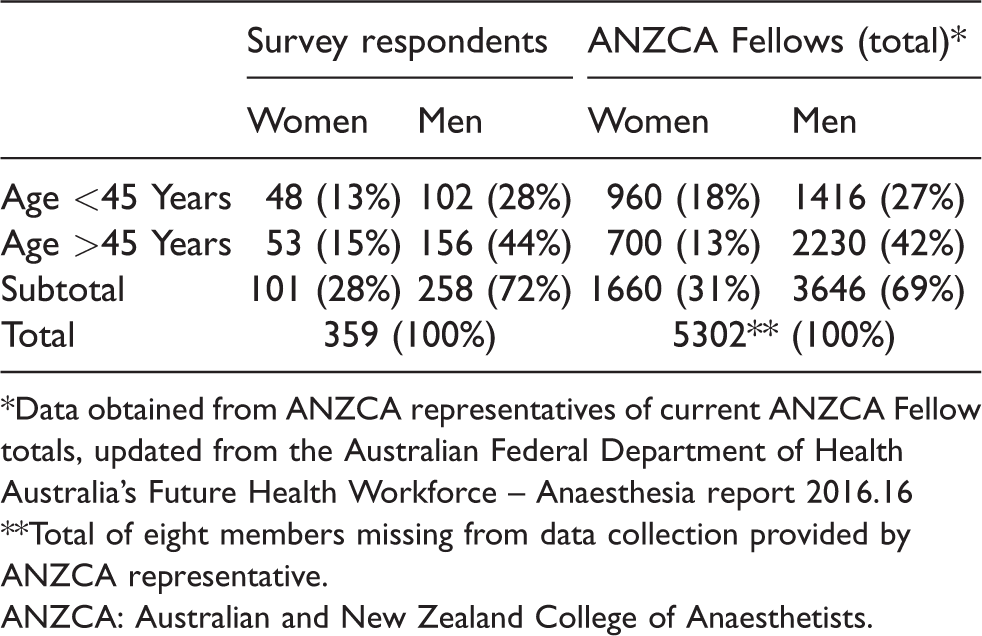
*Data obtained from ANZCA representatives of current ANZCA Fellow totals, updated from the Australian Federal Department of Health Australia’s Future Health Workforce – Anaesthesia report 2016.16
**Total of eight members missing from data collection provided by ANZCA representative.ANZCA: Australian and New Zealand College of Anaesthetists.
Of the question 2 survey respondents, 160/359 (45%) worked solely in a public hospital, 76/359 (21%) worked solely in private practice and 286/359 (80%) worked in a metropolitan area. The Australian Federal Department of Health in 2016 indicated that 51% of Australian anaesthetists worked in public hospitals and 49% in private hospitals (no clarification of the public/private split), 16 and 84% of anaesthetists were concentrated in metropolitan areas classified as major cities. 16 An ANZCA New Zealand workforce study indicated that 29% of anaesthetists worked purely in public hospitals, 7% purely in private hospitals and 65% in a combination of public/private hospitals 19 (no New Zealand data for metropolitan versus regional areas). 19
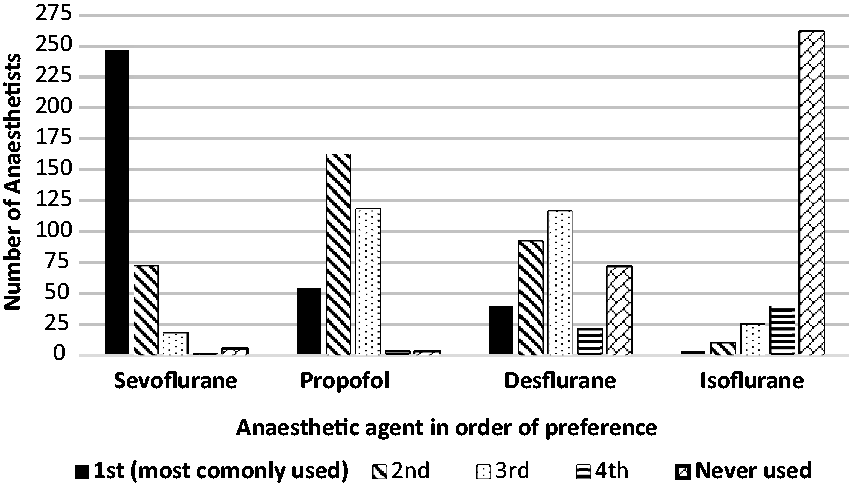
General anaesthetic agents in order of usage.
Question 4 asked respondents to rank general anaesthetic agents from one to four in order of usage. Most respondents (246/340 (72%, 95% CI 67%–77%)) selected sevoflurane as their anaesthetic agent of choice (Table 2), then propofol (54/338 (16%, 95% CI 12%–20%)), desflurane (39/337 (12%, 95% CI 8%–16%)) and isoflurane (3/336 (1%, 95% CI 0%–3%)). Propofol was the preferred second agent of choice (161/338 (48%)). Isoflurane was never used by 259/336 (77%) of respondents, and 71/337 (21%) never used desflurane, while 5/340 (1%) and 3/338 (1%) never used sevoflurane and propofol, respectively (Figure 1).
Rationale for the most frequently used general anaesthetic agent.
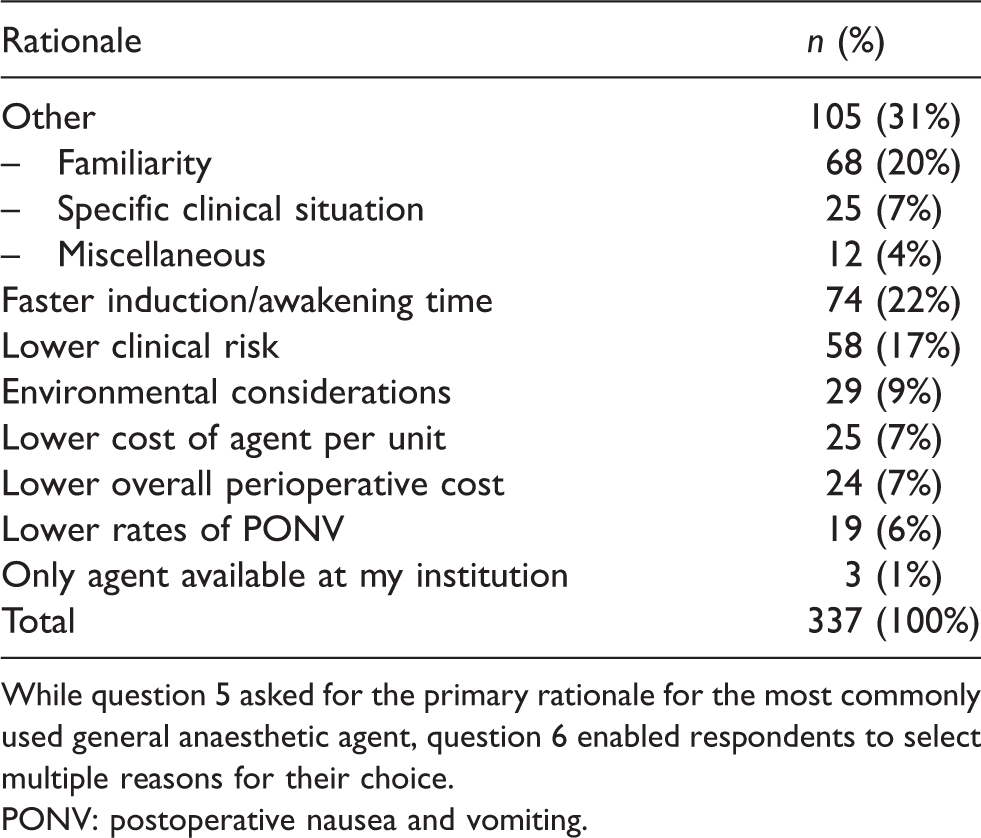
While question 5 asked for the primary rationale for the most commonly used general anaesthetic agent, question 6 enabled respondents to select multiple reasons for their choice.PONV: postoperative nausea and vomiting.
Question 5 asked respondents the primary reason for their chosen general anaesthetic agent (Table 3). ‘Other’ was the most common reason given (105/337 (31%, 95% CI 26%–36%), with ‘familiarity’ the most important explanation provided for ‘other’. ‘Faster induction/awakening time’ was the primary reason for 74/337 (22%, 95% CI 18%–27%)), ‘lower clinical risk’ for 58/337 (17%, 95% CI 13%–22%), ‘lower financial costs’ per unit for 25/339 (7%, 95% CI 5%–11%), ‘lower overall perioperative costs’ for 24/339 (7%, 95% CI 5%--10%), and ‘environmental considerations’ for 29/337 (9%, 95% CI 6%–12%) (Table 3).
Rationale for using each general anaesthetic agent.*
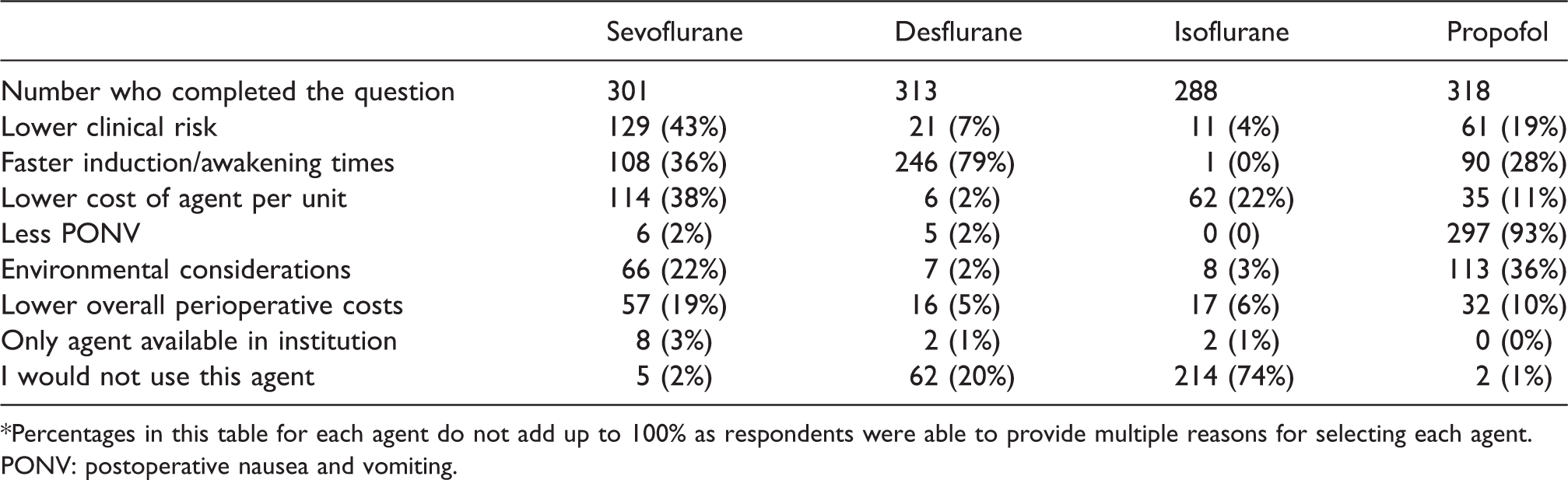
*Percentages in this table for each agent do not add up to 100% as respondents were able to provide multiple reasons for selecting each agent.PONV: postoperative nausea and vomiting.
While question 5 asked for the primary rationale for the most commonly used general anaesthetic agent, question 6 enabled respondents to select multiple reasons for their choice.
Sevoflurane was chosen for a low clinical risk profile (129/301 = 43%), lower cost of agent per unit (114/301 = 38%), faster induction/awakening times (108/301 = 36%) and environmental considerations (66/301 = 22%). Propofol was primarily favoured for a lower rate of postoperative nausea and vomiting (297/318 = 93%). Desflurane was mostly selected for its faster induction/awakening times (246/313 = 79%), while 62/313 (20%) never used desflurane. Most respondents (214/288 = 74%) never used isoflurane.
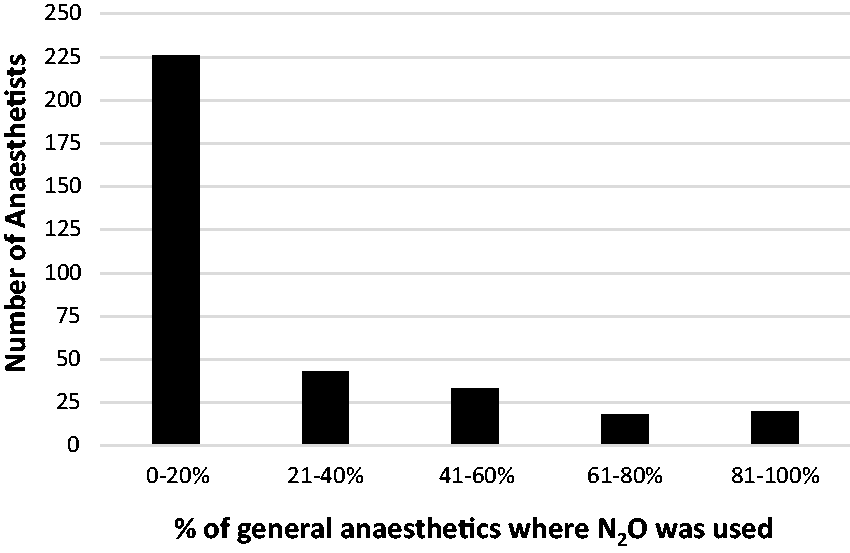
Nitrous oxide (N2O) use. Percentage of general anaesthetics in which N2O was used.
Question 7 asked respondents to estimate in what proportion of general anaesthetic cases N2O was used. Most respondents (226/340 (66%, 95% CI 61%–71%)) used N2O uncommonly (between 0 and 20%), although 38/340 (11%, 95% CI 8%–15%) used N2O for more than 60% of their general anaesthetics (Figure 2).
Questions 8 and 9 asked what was the lowest FGF administered and why they chose this FGF. ‘No use’ was recorded by 4/337 (1%) for sevoflurane, 70/338 (21%) for desflurane and 233/329 (71%) for isoflurane. Seven percent (23/333) of respondents used an FGF of greater than 2 L/minute for sevoflurane, 6/268 (2%) for desflurane and 5/96 (5%) for isoflurane. A minimum FGF of 1–2 L/minute was acceptable for 140/333 (42%) of respondents who used sevoflurane, 43/268 (16%) who used desflurane and 22/96 (23%) who used isoflurane. FGFs of less than 1 L/minute were used by 170/337 (50%) for sevoflurane, 219/268 (82%) for desflurane and 69/96 (72%) for isoflurane (Figure 3).
Question 9 asked for reasons for not using low FGFs (<2 L/minute). The responses given by those who reported using only high FGFs are shown in Figure 4. Thirty-nine out of 263 (12%) respondents indicated they would not administer sevoflurane at low flows primarily because the Australian Therapeutic Goods Administration (TGA) datasheets 13 recommended against low FGF sevoflurane or the Medsafe (NZ) 20 datasheets gave conflicting advice. Few respondents avoided low FGFs when desflurane (10/293 = 3%) or isoflurane (5/215 = 2%) was used.
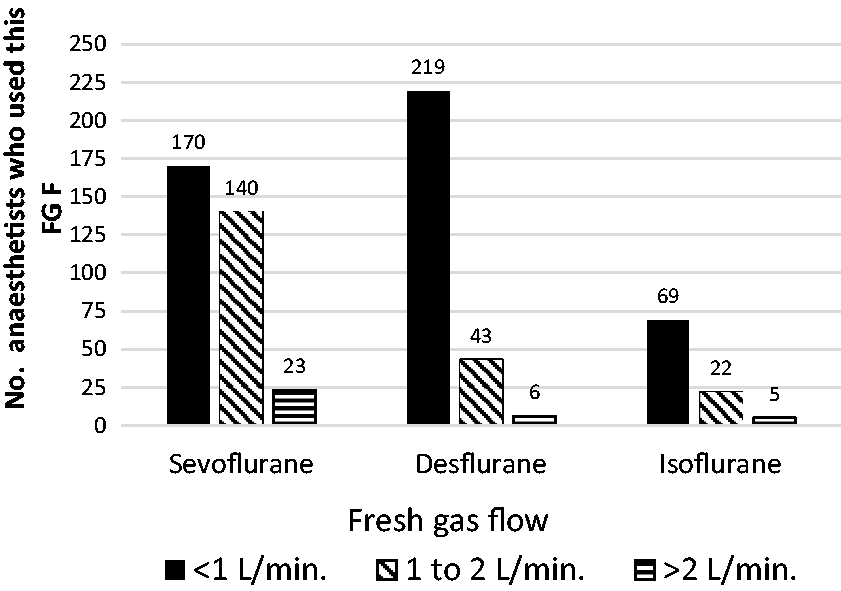
Lowest fresh gas flow (FGF) chosen.
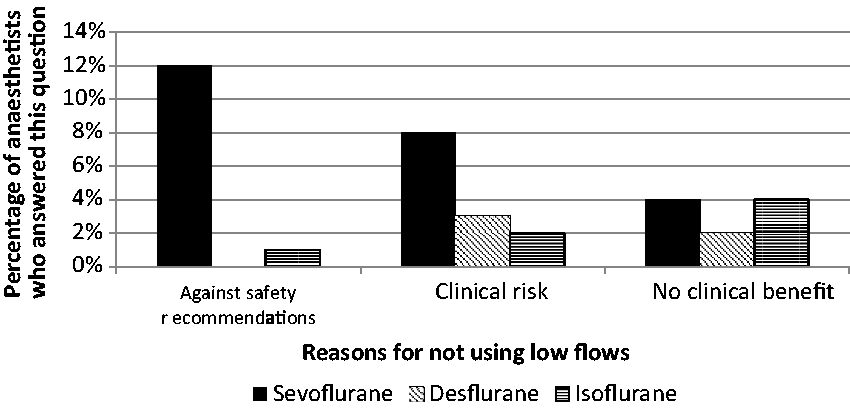
Reasons for not using low (<2 L/minute) fresh gas flow (FGF). Two anaesthetists responded ‘other’ for not using low FGF due to inadequate control of depth of anaesthesia, and circuit leakage.
Question 10 asked if respondents used automated end-tidal concentration control, and of the 333 respondents 196 (59%, 95% CI 53%–64%) did so. Question 11 (‘Further comments’) was answered by 79 respondents, including 10 who wrote ‘no further comments’. Thirty-three respondents wished to have a broader selection of reasons behind clinical choice (12 respondents), and have options tailored to specific clinical circumstances (17) (such as paediatric and neuroanaesthesia in which the use of N2O and propofol were mentioned often) and be allowed to choose more than one reason behind their preferred selection (4). A further nine respondents thought the survey’s questions were invalid or biased (reason for bias unstated), five discussed very low flows (<0.5 L/minute), four mentioned the environment as a factor in their practice, three commented on automated end-tidal control, three supported desflurane for rapid induction/emergence and 12 made other miscellaneous comments.
We were unable to obtain direct volatile marketing data. We obtained Australian (only) national inhalational volatile anaesthetic use for the year 2017 from a healthcare data company (IQVIA, Melbourne, Victoria, Australia). 17 In 2017, volatile use for Australia was: sevoflurane 148,808 bottles = 37,202 litres (70% total number of bottles), desflurane 62,630 bottles = 15,031 litres (29%) and isoflurane 2345 bottles (1%). IQVIA does not obtain N2O data. Despite repeated requests, we were unable to get N2O data from either Australian supplier. We did not seek propofol data as these would have included the total use of propofol beyond general anaesthesia.
Discussion
Our survey of Australian and New Zealand anaesthetists found that about three-quarters of respondents chose sevoflurane, with the remainder closely divided between propofol and desflurane. Desflurane was never used by approximately 20%, while isoflurane was rarely used. N2O was used by 10% of respondents in at least half of their general anaesthetics. Only half of the respondents used sevoflurane at less than 1 L/minute due to concerns about government recommendations and clinical risk, compared to 80% using desflurane at less than 1 L/minute. Approximately two-thirds used automated end-tidal gas control.
Quantitative data on Australian volatile (no N2O data) use in 2017 supported our survey results. Desflurane was the agent of choice for 12% of respondents. Given that desflurane has a potency one-third that of sevoflurane, 21 it was unsurprising that desflurane formed approximately 30% by volume of volatiles used in Australia. At Western Health, Melbourne, sevoflurane cost approximately one-fifth that of desflurane (accounting for potency), although this would vary between hospitals and countries. The global warming potentials of sevoflurane and desflurane are, respectively, 130 and 2540 times that of carbon dioxide (CO2), 3 and minimal for propofol. 22 N2O has a similar global warming potential to desflurane when used clinically by anaesthetists. 2 While there are other environmental considerations (e.g. water and terrestrial pollution from propofol) that add to the complexity of choice of general anaesthetic, we focused on climate change concerns 23 and healthcare’s impacts thereof. 24
Sevoflurane was popular because of the low risk profile, lower cost and faster induction/awakening times. Propofol was favoured for reducing postoperative nausea and vomiting (PONV), and desflurane for faster induction/awakening times. A 2012 French survey with 981 respondents found that general anaesthetic agents were used in different proportions to our findings, with less sevoflurane (50% of all anaesthetics) and more desflurane (24%), but a similar total intravenous anaesthesia (TIVA) percentage (17%). 9 A 2013 survey of Scandinavian anaesthetic departments 10 found that in Denmark less than one-quarter of general anaesthetics involved volatiles (most being TIVA), although in Iceland more than 90% involved volatiles. The use of any N2O varied from minimal (0.6% in Denmark) to almost 40% in Iceland, with an average of 12% N2O use. 25 A 2016 survey of Indian anaesthetists found that sevoflurane and isoflurane were both routinely used by about 55%, halothane 40% and desflurane 17%, and half routinely used N2O. 26 A 2016 USA survey indicated that sevoflurane was chosen by two-thirds of anaesthesiologists, followed by desflurane (22%) and isoflurane (11%). 11
An FGF of less than 1 L/minute was acceptable to 80% for desflurane, but only 50% for sevoflurane, primarily due to concerns that sevoflurane at less than 2 L/minute was not recommended by the Australian TGA. 13 Sevoflurane datasheets associated with Medsafe (NZ) gave conflicting information to either not mention low FGFs, or to avoid low FGFs. 20 Low-flow anaesthesia can maintain patient care, while improving economic and environmental outcomes. 5 A Korean study (2011) showed that the introduction of a maintenance sevoflurane FGF policy of less than 1 L/minute increased the hours per sevoflurane bottle by 38%. 27 A US study (2013) used an anaesthesia machine FGF feedback system that enabled average FGF reduction to 1.6 L/minute. 28 Reducing FGF by automated end-tidal control was used by 60% of our survey’s respondents. A 2013 Australian study showed that automated end-tidal control reduced volatile costs by 27% and greenhouse gas emissions by 44%. 7 Kennedy and French (2014, NZ) reduced all volatile flow rates to less than 1 L/minute for 70% of the time through automated end-tidal control, with the default sevoflurane minimum FGF reduced from 2.0 L to 0.5 L/minute. 29
Our survey of 1000 anaesthetists had a 36% response rate. While our answers are reasonably precise (±5%) there was a risk of non-responder bias. The gender and age of our respondents did reflect the broader ANZCA Fellowship. It is possible that anaesthetists uninterested in environmental anaesthesia did not respond to our questionnaire, causing a biased responder cohort (i.e. it is likely that our study underestimated the use of desflurane and high flow anaesthetic gas use). For these reasons our results should be interpreted with caution. While we did conduct pilot work, the free text comments indicated that many respondents would have preferred: (a) a broader selection of reasons behind clinical choice; (b) a choice of more than one reason behind their preferred selection; and (c) options tailored to specific clinical circumstances (such as paediatric and neuro-anaesthesia). Adding ‘never’ (vs. 0–20%) to whether N2O was ever used would have added clarity. We did not obtain quantitative individual hospital volatile data, and only obtained one year’s data for volatile use from IQVIA.
It is interesting to compare anaesthetic volatile use with everyday activities, e.g. the CO2 equivalent (CO2e) emissions of sevoflurane and desflurane use compared with car travel. An average Australian car travelled 13,716 km in 2016, 30 and produced 0.192 kg CO2e/km (2013 data). 31 In 2017 the 37,202 litres of sevoflurane used by Australian anaesthetists (70% as first preference) had similar CO2e emissions to 773 cars driven for that year, while the 15,031 litres of desflurane (12% as first preference) was equivalent to 14,500 cars on the road for 2017. Given that 90% of users of desflurane in our survey already used low flow, reducing desflurane use would mitigate both financial and environmental costs much more than encouraging low flow sevoflurane and automated end-tidal volatile control.
Our survey provides information about the choice of general anaesthetic agents used in Australia and New Zealand. A standard general anaesthetic would probably be with sevoflurane, at flows of 1–2 litres/minute, with automated end-tidal control, and without N2O. About a quarter of all respondents would choose either propofol or desflurane. Most respondents would choose a general anaesthetic agent according to familiarity, faster induction/awakening times and clinical risk, although uncommonly (10%) for environmental reasons. Our data allow anaesthetists in Australia and New Zealand to consider further whether there needs to be any change in our choices of anaesthetic agents for environmental, financial or any other reasons, and becomes a baseline to track future trends of anaesthetic gas use.
Supplemental Material
Supplemental material for A survey of the choice of general anaesthetic agents in Australia and New Zealand
Supplemental Material for A survey of the choice of general anaesthetic agents in Australia and New Zealand by Forbes McGain, Jason R Bishop, Laura M Elliot-Jones, David A Story and Georgina LL Imberger in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The authors would like to thank Karen Goulding, ANZCA Clinical Trials Network manager for assistance in managing the survey. They also thank the Commonwealth Scientific and Industrial Research Organisation (CSIRO) for funding the Australian national volatile use data sourced from the company IQVIA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.