
Abstract
Background:
How Achilles tendon mechanics and plantar flexion strength and torque steadiness are altered in the intact leg of persons with trauma-related amputation is unknown. Understanding Achilles tendon mechanics following amputation will further inform rehabilitation approaches to enhance posture, balance, and force control.
Objective:
Conduct a pilot study to quantify plantar flexion maximal voluntary contraction torque, torque steadiness, and Achilles tendon mechanics in persons with unilateral trauma-related transfemoral amputation and controls without amputation.
Study design:
Cross-sectional study.
Methods:
Isometric plantar flexion maximal voluntary contractions were performed with the intact leg of ten males with transfemoral amputation (48 ± 14 years) and the dominant leg of age-matched male controls without amputation. Torque steadiness was calculated as the coefficient of variation in torque over 6 s during submaximal tracking tasks (5%, 10%, 25%, 50%, and 75% maximal voluntary contraction). Achilles tendon elongation and cross-sectional area were recorded with ultrasound to calculate strain, stress, and stiffness.
Results:
Maximal voluntary contraction and torque steadiness did not differ between persons with amputation (90.6 ± 31.6 N m, 3.7 ± 2.0%) and controls (95.8 ± 26.8 N m, 2.9 ± 1.2%; p > 0.05). Tendon stiffness (21.1 ± 18.2 N/mm) and strain (5.2 ± 1.3%) did not differ between groups (p > 0.05). Tendon cross-sectional area was 10% greater in persons with amputation leading to 29% lower stress (p = 0.021). Maximal voluntary contraction was a predictor of a lower coefficient of variation in torque (R2 = 0.11, p < 0.05).
Conclusion:
Persons with trauma-related transfemoral amputation do not differ in plantar flexion maximal voluntary contraction and torque steadiness of the intact leg compared with controls without amputation. Larger tendon cross-sectional area reduces stress and enables distribution of force across a greater area.
Background
Persons with lower limb amputation experience reductions in postural balance compared to persons without amputation, influencing overall mobility.1,2 To understand the underlying mechanisms that contribute to balance deficits and reduced mobility, isometric plantar flexion torque steadiness (TS) is a relevant model as the involved musculature contributes similarly and directly to isometric plantar flexion and standing balance.3,4 Isometric plantar flexion maximal voluntary contraction (MVC) torque and TS have been shown to be reduced in a group of largely vascular-related transfemoral amputation with low-physical activity levels compared to controls without amputation. 5 Persons with vascular-related amputation have also exhibited less efficient standing balance compared to controls and persons with trauma-related amputation. 6 It is unknown if MVC and TS are altered in physically-active persons with trauma-related transfemoral amputation. Higher activity levels could induce greater chronic loading of the intact leg during ambulation,7–9 leading to beneficial Achilles tendon (AT) adaptations for torque control.
Persons with amputation often exhibit leg-length discrepancies associated with prosthesis fit, and this imbalance combined with preferential use of their intact leg in daily life, increases loading of the intact leg.7,10,11 Relative to controls, increased loading might induce muscle and tendon adaptations through progressive overload. 12 Progressive overload influences tendon architecture, as seen in the amputated limb, as the higher load sustained by the patellar tendon inside the prosthesis leads to increased tendon thickness. 13 In the intact limb of persons with transfemoral amputation, it is unknown if the AT is altered following amputation, resulting in differences in tendon mechanics compared to persons without amputation. Given the contribution of the AT to balance 14 and gait, 15 understanding AT adaptations following amputation will further inform rehabilitation approaches to enhancing posture, balance, and force control in persons with trauma-related amputation.
In women without amputation who have worn high heels at least five times a week for greater than 2 years compared to women who did not wear high heels, tendon stiffness and cross-sectional area (CSA) increased. 16 These progressive changes were proposed as consequential to the shortening of the gastrocnemius-AT unit because of the constant plantar-flexed position of the foot inside the high heel shoe. Favoring their intact leg for mobility, persons with amputations often adopt a “hopping” gait strategy that requires repeated forceful plantar flexion contractions. 17 Repeated plantar flexion might culminate in repetitive contractile shortening and tendon elongation, and when combined with the potential for augmented unilateral loading, AT stiffness and CSA would likely increase in the intact leg for persons with transfemoral amputation.
In persons without amputation, higher AT stiffness enhances plantar flexion TS, as the stiffer tendon enhances transfer of force from muscle to bone.18–20 Similar to AT mechanics and lower limb TS, distal biceps brachii tendon mechanics influence elbow flexion TS such that lower tendon stress impairs TS at low-torque levels and benefits controlled contractions at higher levels.18,19 Understanding AT mechanics and TS following amputation will help to inform rehabilitation approaches to enhance posture, balance, and force control. If mechanical properties contribute similarly to TS in the lower limb as the upper limb, we hypothesize that lower tendon stress in persons with amputation is unlikely to contribute to enhanced TS at low-torque levels but may culminate in steadier contractions at high torques. In addition, a prior report suggested that chronic loading of the intact leg in active persons with amputation contributed to overuse muscle damage 20 and because long-term muscle damage may lead to reduced MVC as was observed in persons with transfemoral amputation, 5 we would expect TS to be less in persons with amputation compared to controls.21,22 To test our hypothesis of altered AT mechanics influencing TS in the intact leg, we investigated the contribution of AT mechanics to isometric plantar flexion TS in persons with trauma-related transfemoral amputation and age and sex-matched controls without amputation. This is the first study to our knowledge to investigate the contribution of AT mechanics to plantar flexion TS in persons with transfemoral amputation.
Methodology
Participants
Males with unilateral trauma-related transfemoral amputation and age-matched male controls without amputation were recruited. Persons with amputation were included if they were 2 years post-amputation and using a properly fitted prosthesis. Participants were excluded if they reported neurological, muscular, metabolic, cardiovascular, or orthopedic disorders of the intact leg or use of antipsychotic, antidepressant, or sedative medications. The Amputee Activity Survey was used to assess the activity of participants with amputation. The Survey derives a numerical activity score from the participant’s answers to a series of questions administered by an interviewer. The questions cover the ability to put on and take off the prosthesis, the length of time it is worn, stair climbing, details of employment, aids used, domestic responsibilities, regular walking habits, and social activity. Persons with amputation (90.6 ± 31.6 N m) and controls.
Anatomical measures
Anatomical measurements were performed with the knee and ankle angle at 90°. Lever arm length of the foot was measured from the medial malleolus to the head of the first metatarsal, and the AT moment arm was measured from the medial malleolus to the AT. Medial gastrocnemius and AT muscle–tendon junction and the AT’s insertion at the calcaneus were determined using ultrasound and used to measure AT length. Resting tendon CSA was recorded with ultrasound using a single static image, 4 cm superior to the calcaneal tuberosity.
Experimental setup and protocol
The intact (persons with amputation) or self-reported dominant (controls) leg was placed inside the Boot design, Open-unit device, Three-dimensional sensor, Transportable, Ergometer (B.O.T.T.E) device with the foot secured and the ankle at 10° plantar flexion to measure torque5,23 (Figure 1). Participants were seated with the hip at ~60°, with the testing limb extended forward. The non-tested leg rested on the ground with a knee angle of 90° and their arms were folded across their chest. 5 Participants received real-time visual feedback of the three-dimensional resultant torque signal on a computer monitor placed 1.5 m in front of them. Consistent visual feedback was maintained across participants and torque levels by scaling the feedback according to each participant’s MVC torque.
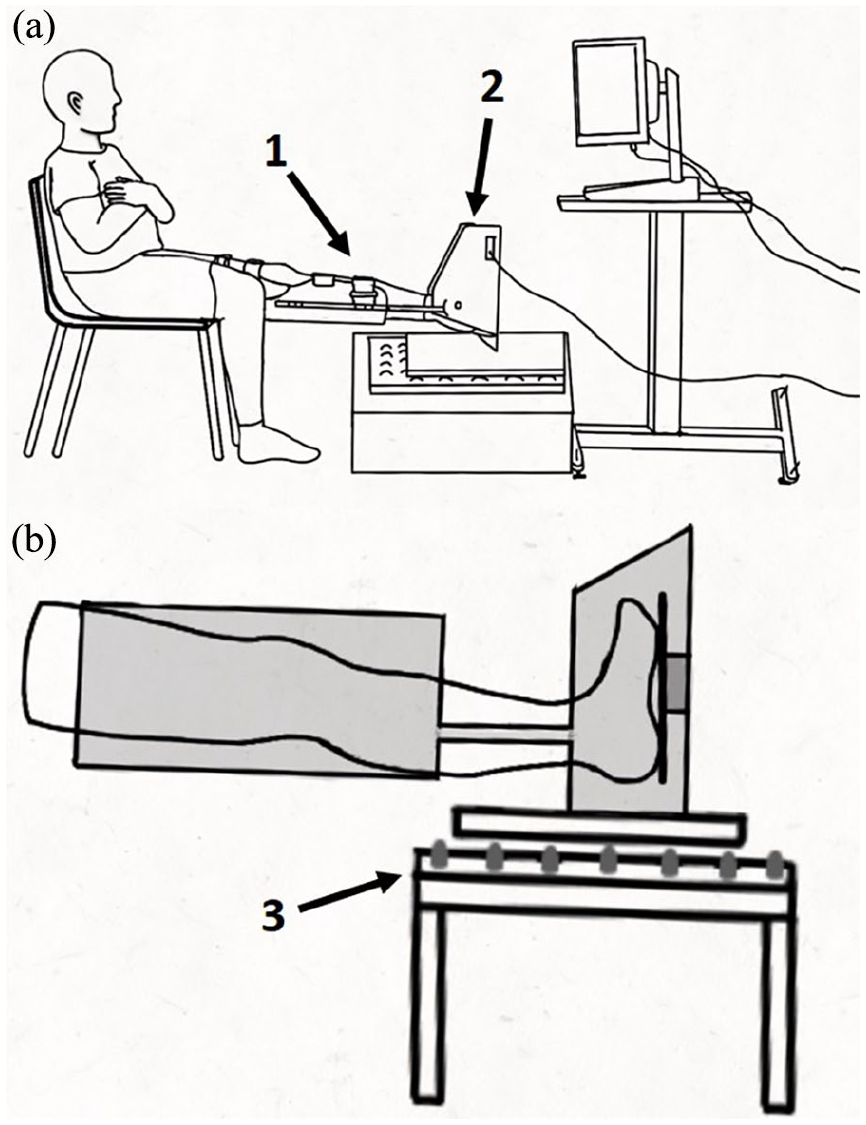
Representative schematic for the (a) B.O.T.T.E device composed of (1) an adjustable orthosis and (2) footplate mounted with a six-component force–torque sensor (Sensix, Poitiers, France). The B.O.T.T.E was used (b) in open-unit configuration with force plate placed onto (3) a ball-bearing housing.
Ag/AgCl surface electromyography (EMG) electrodes (3M Health Care, Canada) were placed on the medial gastrocnemius (MG) and lateral gastrocnemius (LG), soleus (SOL), and tibialis anterior (TA) in a bipolar configuration, 24 with an interelectrode distance of 30 mm. Torque and EMG were sampled at 2048 Hz using a 16-bit A/D board (National Instruments, TX, USA) interfaced with a custom-built MATLAB program (R2017b; MathWorks, Inc., Natick, MA, USA). An ultrasound probe (8 Hz, Echo Wave II; Telemed, St Leger en Yvelines, France) in a custom-built holder was secured to the tested leg to visualize the muscle–tendon junction of the MG and AT for recordings of tendon elongation. A hyperechoic marker visible on the ultrasound image was placed underneath the probe to ensure that the probe did not move during contractions.
Participants performed submaximal contractions to become accommodated to the device, and then performed three isometric plantar flexion MVCs, with 2–3 minutes’ rest between contractions to prevent fatigue. To obtain maximal EMG for the TA, a dorsiflexion MVC was subsequently performed. From the highest plantar flexion MVC, submaximal torque levels of 5%, 10%, 25%, 50%, and 75% MVC were calculated for the tracking tasks (3-s ramp, 8-s plateau, and 3-s de-ramp) and displayed as a template on the monitor with the same visual gain across trials and participants. Participants were required to match their torque production to the template. Each torque level was performed twice in a randomized order, and the average of the two contractions reported for TS and tendon elongation, an additional MVC was done to assess fatigue at the end of the protocol.
MVC and TS analysis
Torque was analyzed offline using custom MATLAB scripts. The torque signal was filtered with a 10-Hz low-pass filter (second-order Butterworth filter, zero lag) and corrected for gravity by subtracting the baseline. The highest torque achieved from the three MVCs was used. TS was measured as the coefficient of variation (CV) of torque for the middle 6 s of the submaximal plateau by normalizing the standard deviation (SD) of the torque signal to the mean torque produced during this contraction. For calculation of tendon mechanics, the resultant force values in Newtons (N) were used.
EMG analysis
The root mean square (RMS; the square root of the average power of the EMG signal for a given period of time) was used to measure the amplitude of the EMG and quantified for 0.5 s of the peak MVC and for a 6-s period during the plateau phase of the submaximal contractions. EMG of the MG, LG, and SOL was normalized to the plantar flexion MVC, while TA EMG was normalized to the dorsiflexion MVC. Coactivation ratio was calculated by dividing the EMG amplitude of the TA by the sum of EMG of the plantar flexor muscles (MG, LG, and SOL) recorded during the submaximal tracking tasks. Off-line data processing was performed in custom-built MATLAB programs.
Ultrasound analysis
Measurements of tendon CSA and elongation were performed using the inherent ultrasound analysis platform (Telemed Echo Wave II). To ensure that the probe remained stable, the distance from a hyperechoic marker to the edge of the image was measured repeatedly during the protocol. CSA of the AT was measured by tracing the outer border of the tendon (Figure 2(a)). Tendon elongation was measured as the differential length of the tendon between rest and contraction, where tendon length was measured from the edge of the ultrasound image to the muscle–tendon junction (Figure 2(b) and (c)). The average of two contractions at each torque level was reported for tendon elongation. Strain was quantified as the percentage of tendon elongation relative to resting length and tendon stress as the ratio of tendon force to resting tendon CSA at each torque level. Tendon force was calculated as the quotient of muscle moment and AT moment arm, with muscle moment obtained from the product of the absolute force produced at each force level and the lever arm length. Tendon stiffness was calculated as the slope of the tendon force–elongation relationship and Young’s modulus as the slope of the stress–strain relationship from 50% MVC to MVC.
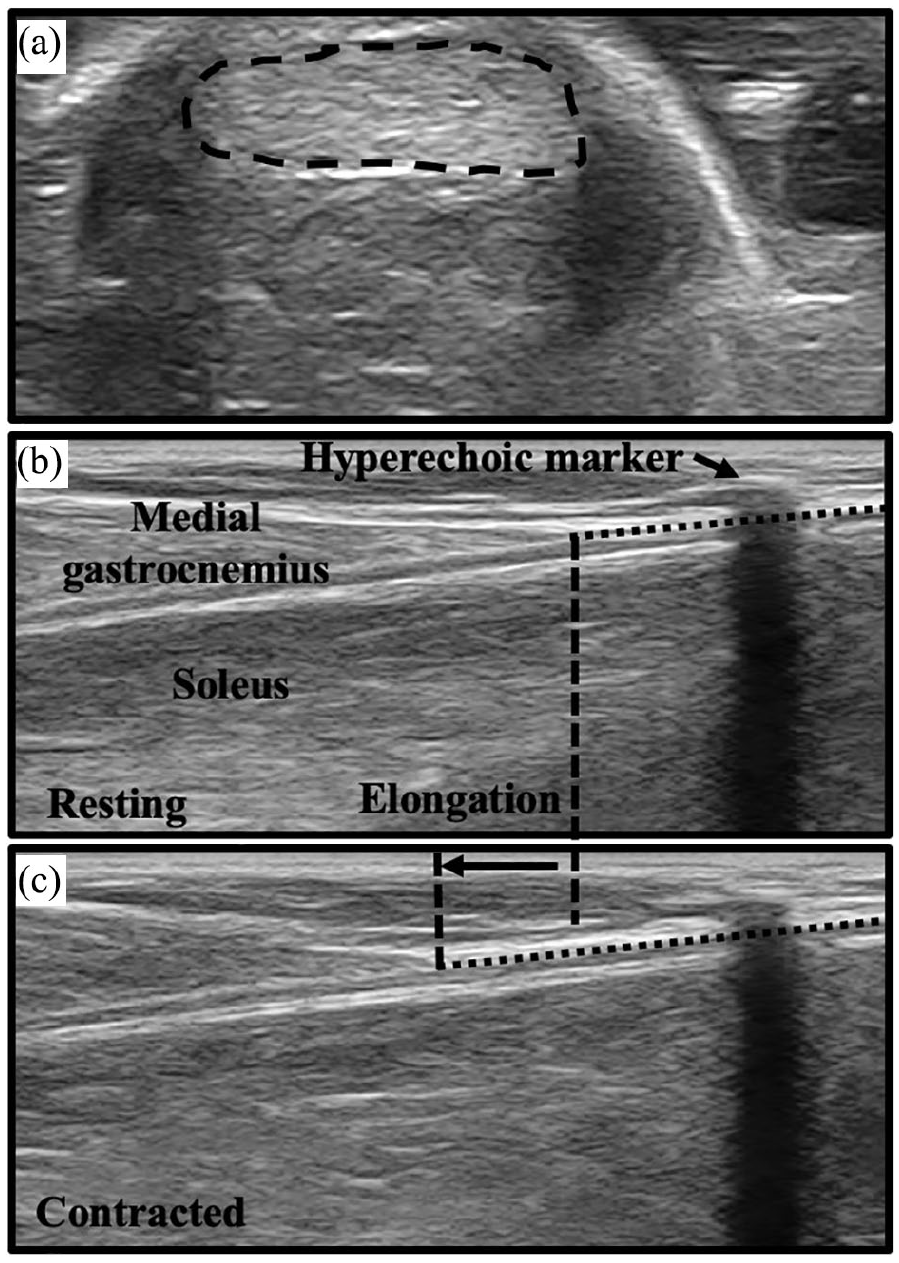
Representative ultrasound images of (a) resting Achilles tendon cross-sectional area (CSA), and measures of tendon length at (b) rest and (c) during contraction at 25% of maximal voluntary contraction (MVC) to quantify tendon elongation.
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM, Amrok, NY, USA). Resting measures of tendon length. CSA, and MVC; tendon stiffness; and Young’s modulus were compared using independent-samples t-tests. Normality of these variables was checked using the Shapiro–Wilks test. Variables that were not normally distributed were compared between groups using a Mann–Whitney U test. Submaximal TS (CV of torque) and EMG were compared between groups and across torque levels using a 2 (group: persons with amputation and controls) × 5 (torque level: 5%, 10%, 25%, 50%, and 75% MVC) repeated measures analysis of variance (ANOVA). Tendon mechanics of elongation, strain and stress were compared using a 2 (group: persons with amputation and controls) × 6 (torque level: 5%, 10%, 25%, 50%, 75% MVC, and MVC) repeated measures ANOVA. When the assumption of sphericity was violated for the repeated measures ANOVAs according to Mauchly’s test of sphericity (p ⩽ 0.05), degrees of freedom were corrected using Greenhouse–Geisser estimates. Correlations of tendon mechanics of strain, stress, and stiffness to CV of torque were assessed using Pearson’s correlations and multiple linear regressions at low (5% and 10% MVC) and high (25%, 50%, and 75% MVC) torque levels. For MVC, Spearman’s Rho was used because it was not normally distributed. Torque levels were split for low and high as CV of torque was significantly higher at 5% and 10% MVC compared to 25%, 50%, and 75% MVC. Tendon stiffness was not used in the low-torque regression model as it was calculated at high torques. Pearson’s correlation coefficients (r) were considered very weak (0–0.3), weak (0.3–0.5), moderate (0.5–0.7), and strong (0.7–1). Values are reported as means ± SD in text and means ± standard error (SE) in figures. Significance was set at an alpha value of 0.05.
Results
Ten males with unilateral trauma-related transfemoral amputation and ten age-matched male controls without amputation participated in this study (Table 1). Shapiro–Wilks test showed that MVC (W(9) = 0.76, p = 0.006) and moment arm (W(9) = 0.81, p = 0.03) were not normally distributed for persons with amputation, while tendon length (W(8) = 0.74, p = 0.006) was not normally distributed in controls.
Subject characteristics and group main effects for resting anatomical measures and Achilles tendon mechanics.
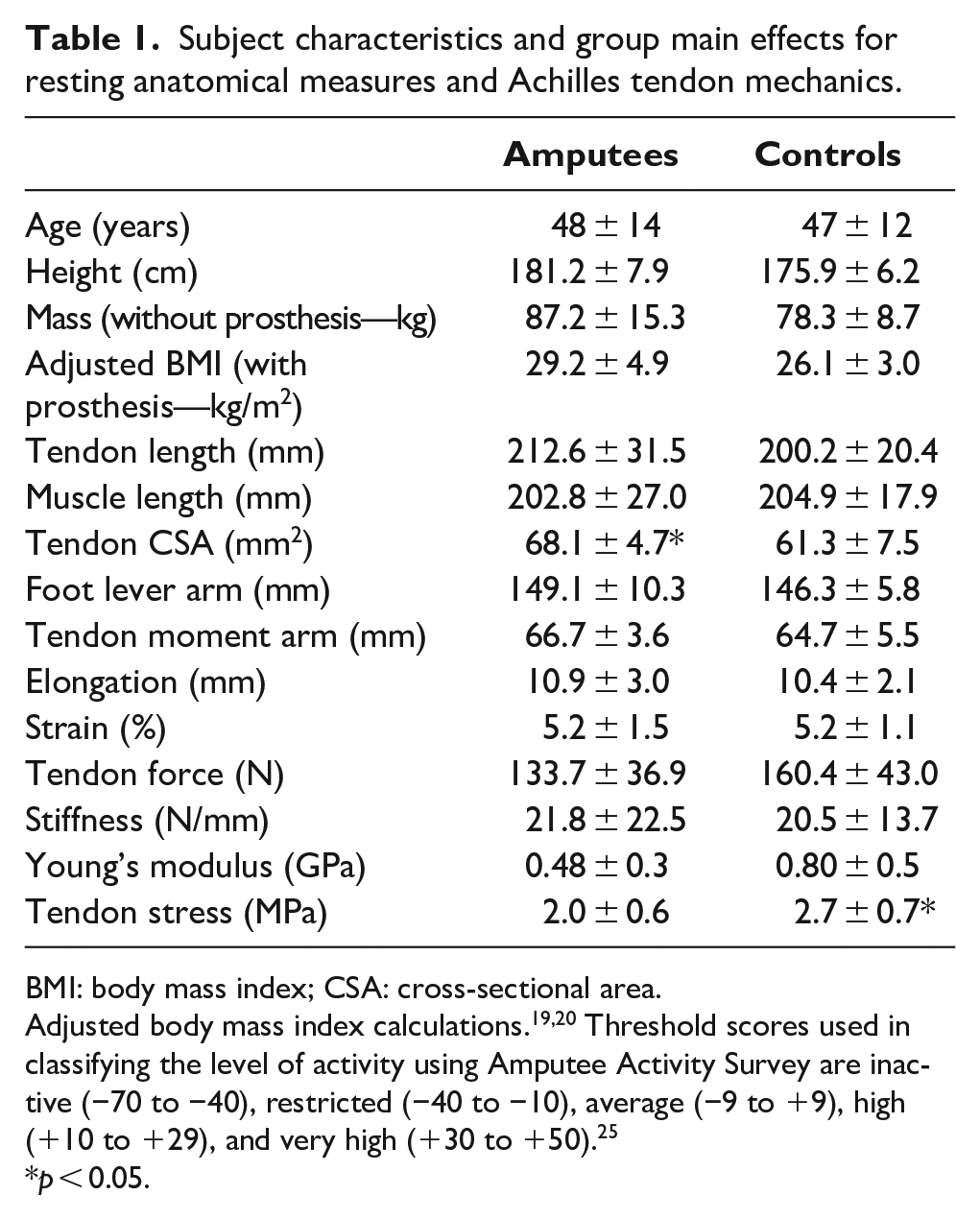
BMI: body mass index; CSA: cross-sectional area.
Adjusted body mass index calculations.19,20 Threshold scores used in classifying the level of activity using Amputee Activity Survey are inactive (−70 to −40), restricted (−40 to −10), average (−9 to +9), high (+10 to +29), and very high (+30 to +50). 25
p < 0.05.
MVC and TS
Persons with amputation were 14 ± 12 years since trauma-related amputation and were active according to the Amputee Activity Survey (27.3 ± 20.7).
25
Persons with amputation (90.6 ± 31.6 N m) and controls (95.8 ± 26.8 N m) did not significantly differ in plantar flexion MVC (U = 40.0, η2 = 0.03, p = 0.5) (Table 1). MVC normalized by height and weight, respectively, did not differ between persons with amputation (0.50 ± 0.16 N m/cm and 1.05 ± 0.34 N m/kg) and controls (0.54 ± 0.15 N m/cm and 1.23 ± 0.33 N m/kg) (p = 0.5 and p = 0.3, respectively). There was a main effect of torque for CV of torque (F(2,33) = 6.6,
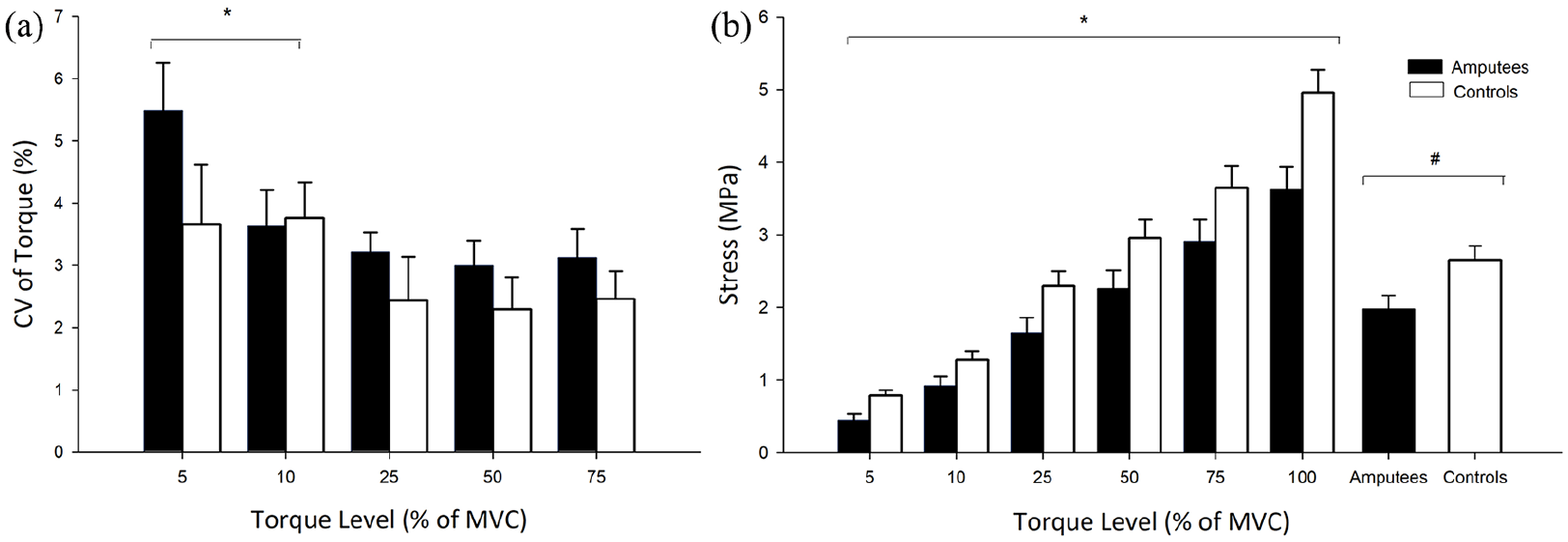
(a) Coefficient of variation (CV) of torque across torque levels for amputees and controls. (b) Tendon stress for amputees and controls across torque levels and the group main effect.
EMG
There was no interaction for EMG between torque level and group for LG (F(2,33) = 2.3,
Muscle EMG activation and coactivation across force levels (5%, 10%, 25%, 50%, and 75%) for persons with amputation and controls during plantar flexion isometric contraction.
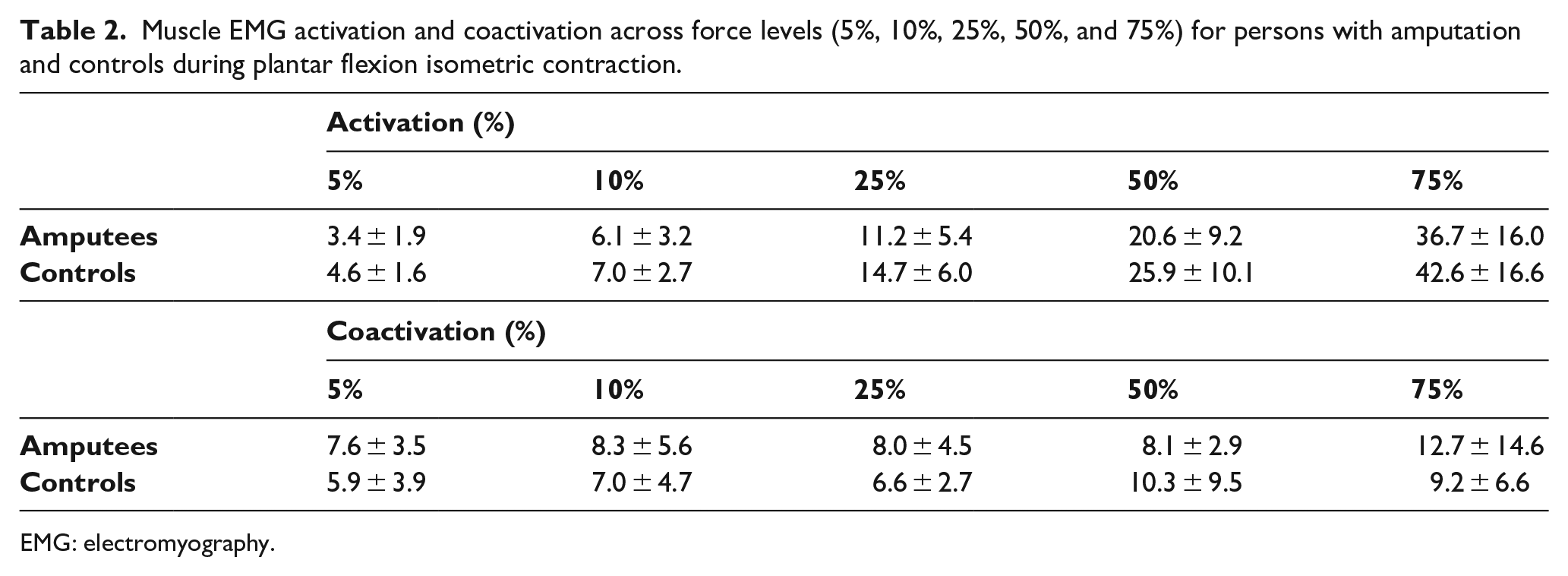
EMG: electromyography.
Muscle and tendon measures
Muscle (F(1,18) = 0.04, η2 = 0.002, p = 0.8) and tendon (U = 40.5, η2 = 0.03, p = 0.5) lengths did not significantly differ between groups, while AT CSA was greater in persons with amputation compared to controls (F(1,18) = 5.9, η2 = 0.3, p = 0.03). Foot lever arm length (F(1,18) = 0.6, η2 = 0.03, p = 0.5) and tendon moment arm length (U = 34.0, η2 = 0.08, p = 0.2) did not differ between groups (Table 1). There was no interaction between torque level and group for tendon elongation (F(2,35) = 1.2,
Correlation and regression analysis
Correlation and regression analyses were performed separately for low (5% and 10% MVC) and high (25%, 50%, and 75% MVC) torque levels on the combined data for persons with amputation and controls as they did not significantly differ in TS (Figure 3(a)). For the higher torques, MVC (rs = −0.43) and tendon strain (r = −0.25) had very weak negative correlations with CV of torque (p < 0.05). The multiple forward linear regressions indicated that a higher MVC was a predictor of reduced CV of torque (i.e. increased steadiness), explaining 9.6% of the variance in CV of torque (F(1,39) = 5.1,
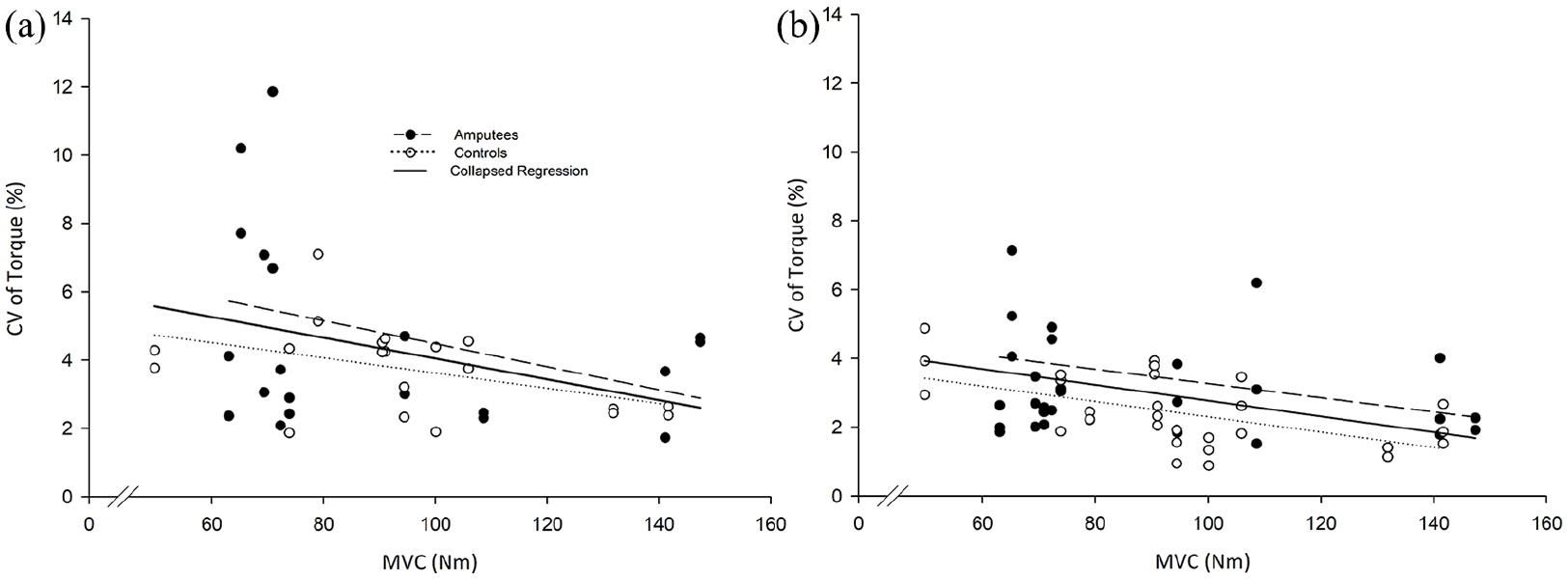
Linear regression of MVC and CV of torque for (a) low (R2 = 0.11, p = 0.03) (multiple regression equation y = 6.62–0.027 (MVC); beta weight coefficient = −0.35; R2 = 0.11; adjusted R2 = 0.096) and (b) high (R2 = 0.14, p = 0.003) (multiple regression equation y = 4.30–0.017 (MVC); beta weight coefficient = −0.38; R2 = 0.14; adjusted R2 = 0.13) torque levels for amputees and controls.
Discussion
The purpose of this pilot study was to determine how trauma-related transfemoral amputation alters AT mechanics and whether this influences plantar flexion torque and TS in the intact leg. MVC, tendon strain, and tendon stiffness were unaltered in persons with trauma-related transfemoral amputation, and this culminated in a similar ability to maintain steady isometric torque compared to controls. However, the CSA of the tendon was greater in persons with transfemoral amputation, which reduced tendon stress. These data suggest that the intact leg of persons with trauma-related transfemoral amputation does not differ in maximal plantar flexion strength, and thus, the control of steady contractions is similar to age- and sex-matched persons without amputation.
Contrary to expectations, no significant differences were found in MVC or TS between persons with amputation and controls. It was previously reported that MVC and TS are reduced in the intact leg of persons with transfemoral amputation during plantar flexion; 5 however, the cause of amputation in this previous study was either trauma or vascular dysfunction. In vasculature-related amputation, factors beyond the amputation likely associated with disease are a primary consideration in rehabilitation in order to increase strength and TS of the intact leg.
To compensate for the prosthesis during gait, vertical ground reaction force, net joint moments, and power output increase in the intact limb.7–10 This compensatory approach induces muscle asymmetry through progressive overload and may have culminated in greater AT CSA of the intact leg in persons with transfemoral amputation. Habitual loading is associated with robust changes in tendon size and mechanical properties. 26 If a “vaulting” style gait, as opposed to a typical swing style gait, is used to accommodate for the length discrepancy and motion limitations of the prosthesis, this could elevate tensile strength and increase AT CSA through habitual use, similar to increases seen following resistance training27,28 or high levels of physical activity. The physical activity levels in the amputee group of this study likely engendered increases in TS through associated increases in strength.22,29 Physical activity increases with time post-amputation. 30 In this study, the Amputee Activity Score (27.3 ± 20.0) was considerably higher compared to the previous study (1.6 ± 19.9) 5 and likely explained the enhanced TS. However, further testing is required for the Amputee Activity Survey to determine whether scores correlate with enhanced TS. The age of participants is also a likely factor in maintaining TS. Age at time of amputation may have allowed the younger group of persons with trauma-related amputation in our study (aged 47 years) to recover MVC and TS at a faster rate compared to persons with amputation in the published study that included older individuals with vascular-related amputation. 5
Prior studies reported that AT stiffness is maintained in adults who have larger tendon CSA;19,31 however, Young’s modulus was lower. We did not observe differences in stiffness or Young’s modulus with an increase in CSA, which is similar to observations in runners relative to untrained individuals. 32 The higher tendon CSA in persons with amputation is likely induced through increased loading of the tendon; however, this added load is insufficient to produce adaptations in tendon material properties of stiffness, strain, and Young’s modulus that would alter how torque is transferred through the tendon. This similarity between AT stiffness in persons with amputation and controls was a likely factor in TS not differing between groups. Prior studies suggest that greater variability in torque output is related to lower tendon stiffness. 31 Therefore, if tendon mechanics are altered in persons with amputation in the months following amputation due to bedrest, 33 it appears that years following amputation, tendon stiffness, strain, and elongation do not differ from controls and this enables TS to be similar to the dominant leg of able-body controls. This may contribute to increased functional daily activities such as balance 3 and gait. 15 Although plantar flexion TS has been shown to be a significant predictor of functional measures, such as balance, this requires further study.
The MVC torque capacity of the plantar flexor muscles is a primary factor contributing to TS in persons with amputation and controls. However, activation of LG and MG was lower in persons with amputation and, surprisingly, no differences were found in TA activation and coactivation ratio. In persons without amputation, properties of the motor neuron pool play a significant role in the ability to maintain steady contractions, 34 but it remains unknown if activation of the motor neuron pool is altered in persons with transfemoral amputation, contributing to their ability to maintain steady force production. Future investigations on muscle activation are required to fully understand factors contributing to force control in the intact leg of persons with unilateral amputation. Moreover, the participants of this study were males, which limite the generalization of these findings to females. Further studies are needed in males and females with amputation to ascertain sex-related differences in the neuromuscular adaptation of the intact ankle. A variety of sex-based factors, such as the types of motor units and population characteristics, agonist-antagonist muscle activity, strength, and tendon mechanics, should likely be considered to better understand TS in persons with vascular and trauma-related amputations. To further understand how adaptations of the AT to altered loading patterns following unilateral amputation contribute to functional torque control, longitudinal studies should be undertaken that evaluate tendon mechanics and TS from the time immediately following amputation to several years post-amputation. Knowledge on longitudinal adaptations in TS and tendon mechanics will aid to enhance rehabilitation approaches for persons with amputation by optimizing functional torque control.
Conclusion
This pilot study demonstrates that in a group of males with trauma-related transfemoral amputation, MVC, TS, AT strain, and tendon stiffness of the intact leg do not significantly differ from controls; however, tendon stress is less in males with amputation due to greater AT CSA. Findings in this study show that males with trauma-related transfemoral amputation do not differ in strength and tendon mechanics at the ankle in the years following amputation compared to males without amputation and this enables similar production of steady isometric plantar flexion contractions.
Footnotes
Author contributions
AT, RS: conducted experiment, data analysis, prepared manuscript.
JJ: project design, prepared manuscript.
ESB: project design, contributed to the final version of the manuscript.
DE: developed the coding program for data acquisition and analysis.
SL, JB: contributed to the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was granted by the French Research Ethics Committee of the University Polytechnique Hauts-de-France.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Natural Science and Engineering Research Council of Canada (NSERC) and Mitacs Globalink.