
Abstract
Background:
Socioeconomic status has been shown to be an important factor in the disparate prevalence and selected treatment of limb loss, but how personal financial difficulty affects patients’ health outcomes is currently unclear.
Objective:
Examining how presence and experience of personal financial difficulty affects perceived health and wellbeing in individuals with lower limb loss.
Study Design:
Cross-sectional study.
Methods:
A total of 90 participants (68 males, mean age 58.7 ± 16.7 years) were recruited from local physical therapy and prosthetic and orthotic clinics, rehabilitation hospitals, and a regional amputee patient support group. All participants were community-dwelling, non-military adults with amputation involving at least one major lower limb joint. Participants were interviewed, and each completed a survey that included basic demographic/medical information, self-reported health and wellbeing (Short-Form Health Survey, SF-36v2), and a question to determine their financial situation after limb loss. Multiple regression analyses were used to examine the effect of financial difficulty on the eight subscales of SF-36v2 while accounting for age, gender, and amputation level.
Results:
Experiencing financial difficulty significantly and negatively affected Role-Physical and Role-Emotional subscale scores (p < 0.01 and p = 0.02, respectively). Individuals with financial difficulty scored approximately 60% lower in these two specific subscales.
Conclusion:
Experiencing financial difficulty is a significant predictor for diminished work or daily activity participation due to physical and emotional stresses. Clinicians and health policy makers need to understand how socioeconomic factors may prevent individuals with lower limb loss from achieving higher levels of functional recovery and community re-integration after amputation.
Clinical relevance
Our findings showed that presence or experience of financial difficulty was significantly associated with diminished community re-integration in community-dwelling, non-military adults with lower limb loss. It affects both physical and emotional aspects of wellbeing. Clinicians should be aware how socioeconomic factors may affect social re-integration after amputation.
Background
Previous studies have shown that certain socioeconomic status and variables are significantly associated with elevated risk of limb loss. Those of ethnic minority account for a disproportionately large percentage of the limb loss population in the United States and other countries.1 –4 Comorbidities that are commonly associated with lower limb amputation, such as diabetes mellitus and other dysvascular diseases, are also strongly related to socioeconomic status. For example, Gaskin et al. 5 identified low socioeconomic status (i.e. living in high-poverty neighborhoods with inadequate access to health care services) as a key risk factor for type 2 diabetes. While the causes of the health disparity in limb loss have been extensively investigated and debated,6 –9 there is strong evidence suggesting that socioeconomic factors play a major role in the health of persons at risk of and with limb loss. 4
Sheehan and Gondo 10 eloquently described the fragmentation of current US health care system in which patients easily get lost during the process of amputation and subsequent rehabilitation. Managing care after limb loss is challenging primarily due to the complex coordination between the many care providers including surgeons, physicians, physiatrists, prosthetists, physical therapists, occupational therapists, wound care specialists, pain management specialists, case managers, and potentially many others. 11 While members of the post-amputation rehabilitation team generally recognize the benefits of providing well-coordinated care to a patient, in most cases the patient and family members are left with the responsibility of navigating the difficult health care landscape including health insurance. Furthermore, accessing proper care after amputation can be a substantial financial burden.11,12 Custodio outlined environmental factors, including political, familial, structural, and economic factors as the most likely barriers to effective rehabilitation for patients with limb loss due to extremity sarcomas. 13 It is reasonable to hypothesize that when compared to persons with higher socioeconomic status, those with lower socioeconomic status may face many forms of difficulty in their post-amputation recovery that collectively result in diminished long-term health outcomes and quality of life. For example, Miller et al. 14 showed that higher income (>US$40,000) persons with limb loss exhibit significantly lower fear of falling (a 58% reduction) when compared to those with lower income. The fear avoidance behaviors associated with low income can have negative consequences on long-term function. This problem is also likely exacerbated for non-military, non-Veteran patients since they are not eligible for the comprehensive post-amputation care provided by the military and Veteran’s health care systems.
Despite the accumulating evidence, it is currently unclear how socioeconomic status, specifically personal financial difficulty experienced after limb loss affects long-term health outcomes. This topic has remained an under-researched one, despite its significance as applied to this population. Therefore, the purpose of this study was to examine the effects of personal financial difficulty on self-reported health and wellbeing outcomes in community-dwelling, non-military, non-Veteran individuals with lower limb loss. We focused on income-related poverty status as our main measure of socioeconomic status.15,16
Methods
Participants
Ninety participants with lower limb loss volunteered to participate in this cross-sectional study. Participants were recruited as a sample of convenience from local physical therapy and prosthetics and orthotics clinics, rehabilitation hospitals, and a regional amputee patient support group (Las Vegas Amputee Support Group). Eligible participants were at least 18 years of age and had a significant limb loss (defined as losing at least one major lower limb joint) for at least 6 months. The main exclusion criteria were as follows: significant cognitive/mental illness, inability to understand or respond to the survey questions, or unwillingness to be interviewed. Participants who received care from the VA or military health care systems were also excluded from the analysis. This study is part of a larger, ongoing study on mobility in community-dwelling adults in the Southern Nevada region. Ethics approval was granted by the University of Nevada, Las Vegas, Institutional Review Board for Biomedical Research. Data collection took place between 2016 and 2019.
Procedure
Written informed consent was collected from each participant prior to data collection. Each person was individually interviewed and completed a standardized survey that included questions related to personal information (gender, age, height, weight, ethnicity, and date, level, and cause of amputation), a self-reported health and wellbeing survey, and a question about personal financial status.
Self-reported health and wellbeing were assessed using all eight subscales of the Short-Form Health Survey (SF-36v2; subscales: Physical Functioning, Role-Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role-Emotional, and Mental Health). This measure was selected for its short time requirement to complete and established reliability in the limb loss population.17,18 Specifically, the “Role-Emotional,” “Role-Physical,” and “Social Functioning” subscales were recommended by Resnik et al. 19 as valid and reliable instruments for measuring community integration in persons with limb loss. Each participant’s personal financial status was assessed using the question: “Do you (ever) have difficulty making ends meet at the end of the month?” This question was adopted from a study by Brcic et al. 16 showing it to be 98% sensitive for detecting people living below the poverty line in a field-test setting. When needed, participants were verbally guided by trained interviewers to complete the surveys with a standardized interview script (Supplemental Material). 20 The participants were also informed of their rights to not answer questions that made them feel uncomfortable.
Data and statistical analysis
Descriptive statistics and correlation coefficients were calculated to characterize the participants and the linear dependence among the variables. SF-36v2 item responses were recoded and then transformed to a 0–100 scale in accordance with the survey’s standard scoring instruction.21,22 We chose not to transform the scores to the T-scores since all of our participants had limb loss and the population norm for the score transformation in this specific population was not available. Multiple regression analyses (i.e. general linear mixed model) were conducted to evaluate whether participant’s gender (male vs female), age, financial difficulty (yes vs no), and amputation level (below- vs above-the-knee) affected the eight subscale scores of SF-36v2. Each of the eight-item scores served the dependent variable in their respective model. Individuals with bilateral amputations were included and categorized based on their highest level of amputation. Individuals with knee disarticulation were categorized into the above-the-knee group. Participants with missing data, such as those who did not answer the financial difficulty question, were excluded from these analyses (Table 1). Because the residual analysis showed patterns between the predicted values and residuals, and skewed residual distribution, we transformed age by a logarithmic function to avoid the violations of independence and normality assumptions. Because of the data transformation, we transformed the estimated coefficient (
Characteristics of the participants.
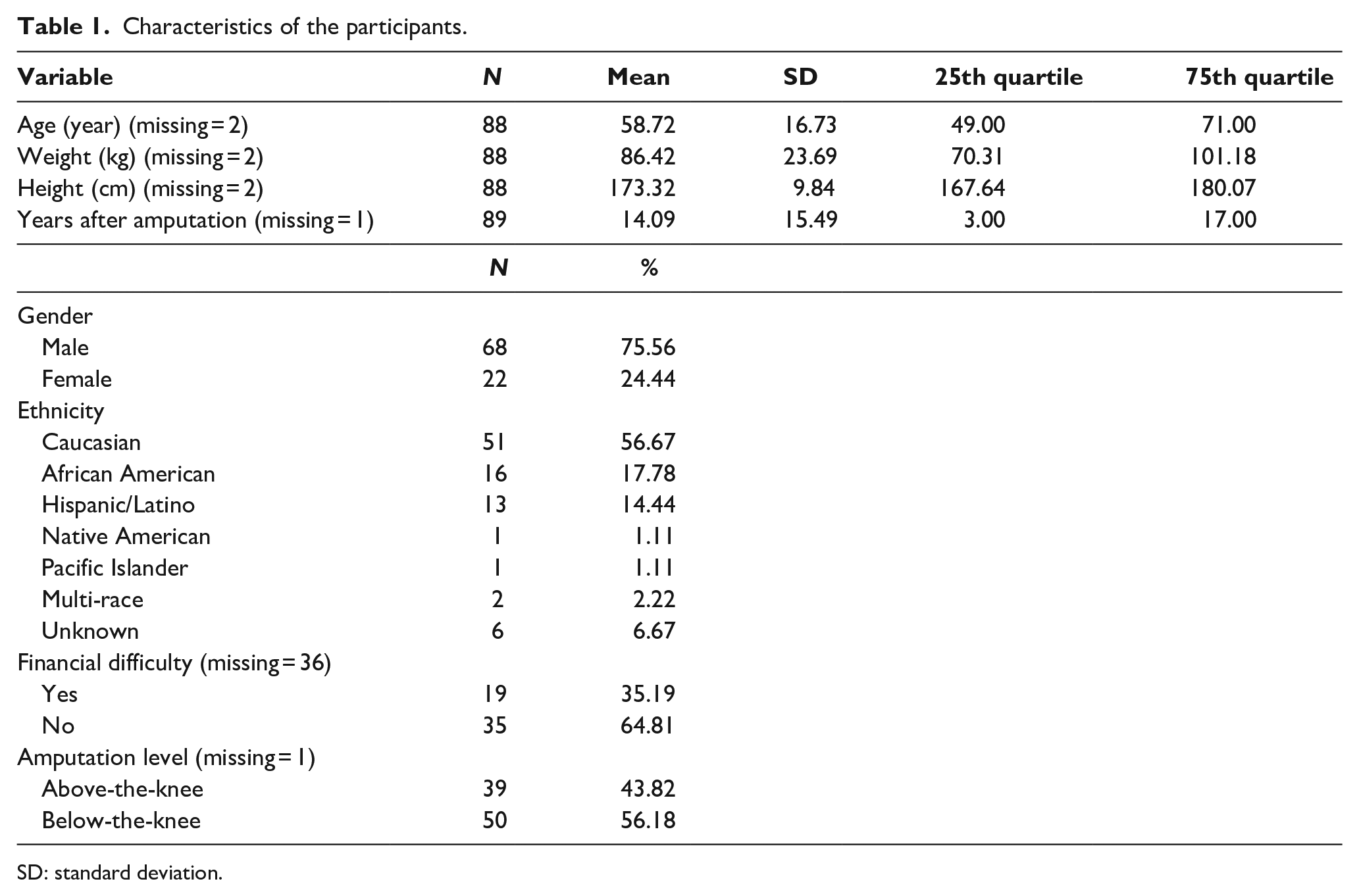
SD: standard deviation.
Power analysis was conducted to calculate the achieved statistical power of each model. The variance of inflation factor (VIF) was calculated for each independent variable within each model to evaluate multicollinearity. All statistical analyses were performed in SAS v9.4 (SAS Institute, Cary, NC). The significance level was set at 0.05.
Results
Table 1 shows the summary characteristics among the 90 participants; 75.56% (N = 68) of them were male, 56.67% (N = 51) were Caucasian, and 56.18% (N = 50) had amputation below the knee. The participants’ average age was 58.72 (standard deviation (SD) = 16.73) with an average weight of 86.42 kg (SD = 23.69) and an average height of 173.32 cm (SD = 9.84). The average time after amputation was 14.09 years (SD = 15.49). More than a third of the participants (35.16%, N = 19) reported experiencing financial difficulties. It should be noted that more than a third of the study participants (N = 36) chose not to answer the financial difficulty question and were excluded from the statistical analyses. Additional exclusions were due to missing data on age (N = 2) and amputation level (N = 1).
Accounting for gender, age, and amputee level, multiple linear regression models revealed significant effects of financial difficulty on Role-Physical and Role-Emotional subscale scores (Table 2). Specifically, those reporting financial difficulties exhibited lower Role-Physical score by 61.99% (p < 0.01; 95% confidence interval (CI) = −79.62, −29.09) and lower Role-Emotional score by 53.98% (p = 0.02; 95% CI = −75.66, −12.99). Males exhibited significantly higher Vitality score (34.88%, p = 0.04; 95% CI = 1.03, 80.07). Age was found to be predictive of Mental Health score where 1-year increase in age significantly increased the score by 0.83 points (p = 0.01; 95% CI = 0.24, 1.41). The power analyses showed that models for both Role-Physical and Role-Emotional achieved adequate statistical power (0.896 and 0.715, respectively). Multicollinearity was examined and did not appear in the covariates for all models (all VIFs < 10, range = 1.02–1.10).
Factors associated with subscales of health and wellbeing in individuals with lower limb amputation (N = 46 in all models).
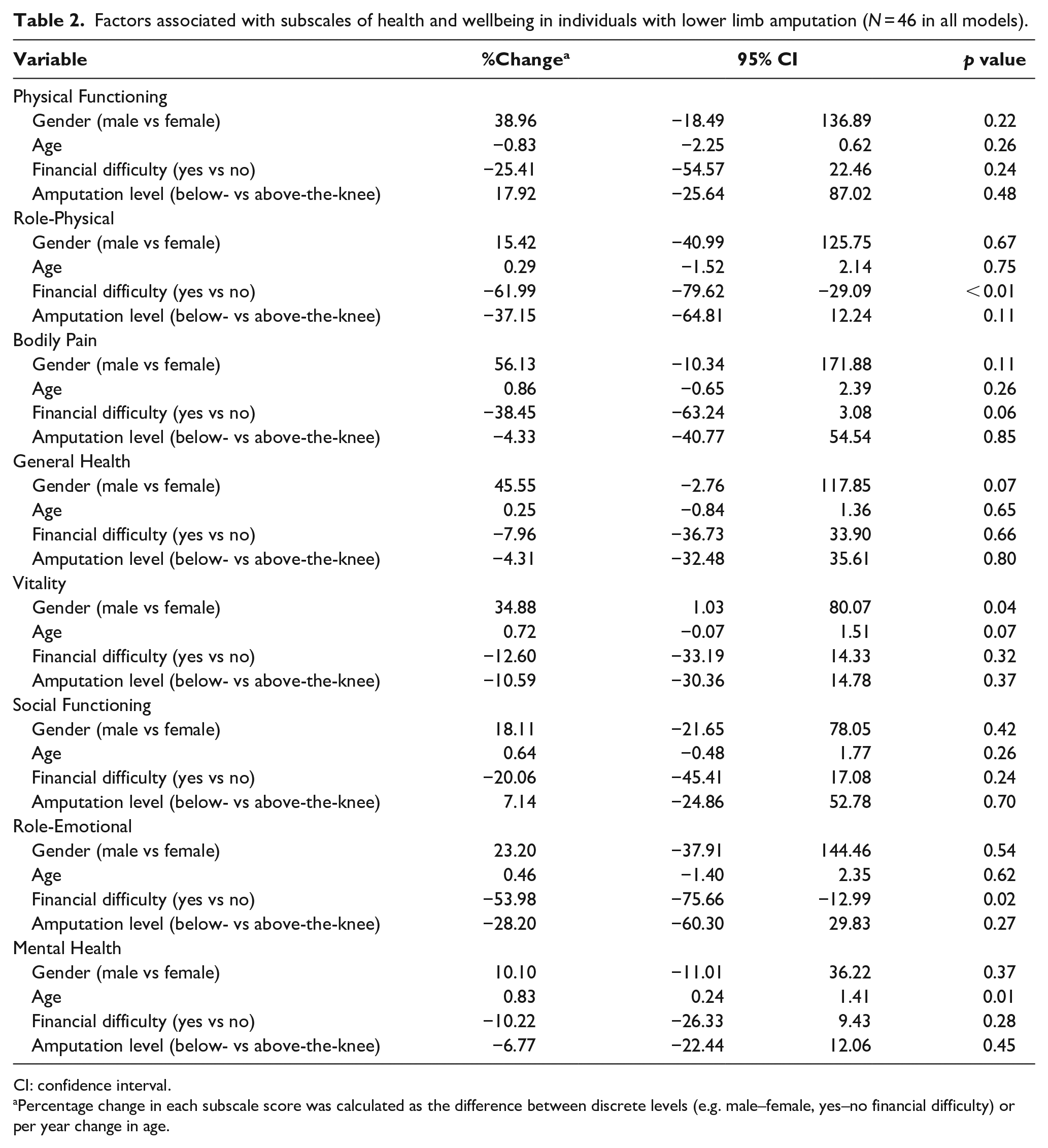
CI: confidence interval.
Percentage change in each subscale score was calculated as the difference between discrete levels (e.g. male–female, yes–no financial difficulty) or per year change in age.
Discussion
This study provided a rare opportunity to explore the associations between personal financial difficulty and different aspects of health and wellbeing in community-dwelling persons with limb loss. Our results indicated that presence or experience of financial difficulty was significantly predictive of specific health and wellbeing outcomes. Those who reported financial difficulty exhibited lower scores in all eight subscales of SF-36v2, and up to 60% lower in two of the three participation-related subscales (i.e. Role-Physical and Role-Emotional). These findings partially supported our hypothesis that personal financial difficulty is associated with diminished function after limb loss.
When compared to age-matched counterparts, it is well established that individuals with lower limb loss exhibited significantly reduced physical function.23,24 This loss of function has been generally attributed to the bodily structural changes inherent to amputation, but a number of studies showed that non-physical stressors disproportionately affected individuals with limb loss. For example, a prognostic study by Melcer et al. 25 showed that patients with limb loss exhibited significantly greater odds of mental health disorders even when compared to those with severe lower extremity trauma but not amputation at comparable disability levels. Furthermore, in a series of studies, Miller et al.26 –28 observed that confidence in performing activities to be the most important predictor of mobility and social activity in individuals with lower limb loss. These findings demonstrated that non-physical factors, such as psychological stress and confidence level, can interact with physical disability and play an important role in predicting health outcomes in individuals with limb loss.
In this study, we chose to use the Short-Form Health Survey (SF-36v2) as the primary measure for health-related quality of life. We made this choice based not only on the survey’s reliability in this population 17 but also its usefulness in capturing community integration at the participation level under the International Classification of Functioning, Disability and Health (ICF) framework. 19 Under the ICF framework, successful participation in personal, family, community, and societal roles can be viewed as the highest level of functional recovery from disability-inducing conditions. This approach has been recognized as essential in assessing rehabilitation outcome after amputation. 29 Participation restrictions in one’s myriad roles in life encompasses many aspects of health, including senses of independence and self-esteem, quality of life, work, and social engagement. Two sets of questions in the SF-36v2 survey focus on patient’s self-perceived extent of restriction that physical health or emotional problems impose on their work and daily activities. For example, question 4a asks, “. . . how much have you cut down on the amount of time you spent on work or regular daily activities as a result of your physical health?” Our finding that participants who reported personal financial difficulty scored on average 61.99% and 53.98% lower in the Role-Physical and Role-Emotional subscales clearly demonstrated the impact of socioeconomic hardship on health and wellbeing. It is worth noting that during our interviews, some participants who experienced financial difficulty commented that the problems they encountered during work or other daily activities are an extension of their physical and emotional health problems presumably associated with amputation. This is consistent with a previous report that almost 80% of the persons who stopped working after their amputation said that amputation-related factors played a major role in their decision. 30 However, while statistically significant, these results should be interpreted with caution given the sizable person-to-person variability evident in the large CI in the SF-36v2 scores.
Presence or experience of financial difficulty did not appear to significantly affect other aspects of health and wellbeing that were more objectively measured, including Physical Functioning, Bodily Pain, Vitality, and Mental Health (p = 0.24, 0.23, 0.32, and 0.28, respectively). For example, questions 3a-j (Physical Functioning Subscale) ask the respondent to rate the degree to which their health limits their ability (from a 3-point scale) to perform daily activities such as carrying groceries, climbing stairs, walking different distances, and bathing. No significant difference was detected between those with and without experiencing financial difficulty. This result seemed to agree with the findings by Miller et al. 14 that after limb loss, persons with lower income exhibit significantly higher fear of falling, but did not have higher actual incidences of falls when compared to those with higher income. In other words, individuals with lower socioeconomic status may perceive their level of functioning (i.e. participation) as being lower when compared to those with higher socioeconomic status. Future research is needed to examine the longitudinal effects of financial difficulty and the associated stress on higher levels of recovery including participation and community re-integration after limb loss.
The ultimate objective of post-amputation rehabilitation is to enable individuals to recover as independent, productive members of their respective communities. For many persons with limb loss, this means a return to meaningful employment.31,32 In addition to financial necessity, a high percentage of people with limb loss cited social contacts at the workplace as a main motive for returning to work. 33 Those who were able to return to work also tended to exhibit better health outcomes. 30 However, current data suggest that after lower limb amputation, the return-to-work rate is only 50% to 66% with even lower rates for those with higher levels and/or bilateral lower limb amputation.32,34 Even for those who successfully returned to work, most had to shift to different jobs or significantly reduce their working time,30,32 which logically presents a financial impact. Fernandez et al. 35 reported that men who had gone through an amputation early in life also tended to attain lower levels of education, contributing to a lower socioeconomic status. Clearly, limb loss is a life-changing event that inevitably affects a person’s life experiences including educational achievement, financial outlook, and/or other aspects of life. These factors are also likely inter-related in their effects on functioning and participating in societal roles for individuals with limb loss. Members of the post-amputation rehabilitation team should not overlook these aspects when providing care.
The benefits of receiving specialized care after limb loss are well established in the current literature.36 –38 Post-amputation rehabilitation has been shown to improve overall gait performance and shorten the time required to regain independent ambulation.39,40 In addition to improving physical functioning outcomes such as gait performance, patients receiving post-amputation care also reported improved senses of freedom, self-confidence, and quality of life. 41 While post-amputation care is clearly beneficial, access to such care may be limited due to many factors. To date, specific examination of barriers to care after limb loss is limited to mostly military and Veteran’s health care systems in the United States. Resnik et al. conducted a series of studies to examine predictors of receiving health care services associated with amputation within the VA Health Care System. They found that Veterans of African American minority descent 42 and those who were older than 65 43 were significantly less likely to receive post-amputation rehabilitation care including prosthetic prescription and/or rehabilitation. Furthermore, Resnik and Borgia found that geographical region and hospital size, but not patient characteristics, were more predictive of whether a Veteran patient received rehabilitation care after amputation. 44 While these studies are informative, the authors recognized that the results may not be generalizable to non-Veteran persons with limb loss. 44 This same group of authors also pointed out that the cost of prosthetic care alone likely exceeds the annual and lifetime cap of most civilian health insurance policies, which would be a significant financial burden for those outside of the government-provided comprehensive health care coverage. 43 It is imperative for future research to further investigate barriers to recovery after limb loss, including how access to care and health outcomes differ in individuals with different ethnicity, income level, employment, education, and prosthetic insurance coverage (i.e. military and VA vs civilian).
Limitations
Findings of this study should be interpreted with consideration of the following limitations. The relatively small sample size was an obvious limitation despite achieving proper statistical power levels in both the Role-Physical and Role-Emotional models. Studies utilizing aggregated health care data may achieve much larger sample sizes which may be needed to detect changes in selected other subscales of SF-36 (e.g. we calculated that it will require a sample of 1823 to detect a potential difference in the General Health subscale). However, we believe findings from the current study are still valuable in that the face-to-face data collection provides better control for variations in assessment and response when compared to aggregated secondary data. In addition, while the specific question we used to detect poverty in a clinical setting has been shown to be highly sensitive (98%), its specificity is low (40%).15,16 False-positive identification of individuals with financial difficulty may be a concern. About a third of the participants also chose not to answer this question, perhaps due to the question’s sensitive nature. Because we did not know specifically the reasons why these participants chose not to answer the question, this may have led to a selection bias. A better understanding of the lived reality of poverty, such as including queries regarding food and housing security, may be helpful in painting a more complete picture.16,45 Furthermore, the poverty-identifying question used in this study, even when answered, does not provide information on the timing and cause of financial difficulty in relation to the person’s amputation. Personal financial burdens caused specifically by amputation and the associated complications should be examined in future research.
Conclusion
Using the Short-Form Health Survey (SF-36v2) as the primary outcome measure, presence or experience of financial difficulty was identified as a significant predictor to diminished work and daily activity participation due to physical and emotional stresses. In addition to recognizing socioeconomic status as an important factor underlying the disparate prevalence of limb loss, health policy makers and clinicians need to understand how financial hardship may prevent individuals with limb loss from achieving higher levels of functional recovery and community re-integration. For example, clinicians should recognize that financial difficulty may lead to higher levels of perceived disability in certain functions. Health policy makers should also consider the impact of personal financial stress associated with the cost of care in those with limb loss. Future research is needed to identify the inter-relationships between socioeconomic status, health care access, insurance coverage, employment, and long-term outcomes after limb loss.
Supplemental Material
10.1177_0309364620921756_Supplementary_material – Supplemental material for Financial difficulty in community-dwelling persons with lower limb loss is associated with reduced self-perceived health and wellbeing
Supplemental material, 10.1177_0309364620921756_Supplementary_material for Financial difficulty in community-dwelling persons with lower limb loss is associated with reduced self-perceived health and wellbeing by Szu-Ping Lee, Lung-Chang Chien, Tyler Chin, Heather Fox and Juan Gutierrez in Prosthetics and Orthotics International
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Lee reports grants from Encompass Health Corporation, during the conduct of the study and grants from National Institute of Health, personal fees from Department of Defense CDMRP-DMRDP review panel, outside the submitted work; in addition, Dr Lee has a patent Method and Apparatus for Performing Timed Up-And-Go Test issued.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the UNLV Department of Physical Therapy and Encompass Health Corporation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.