
Abstract
Background:
Mobility clinics are designed to extend gait and mobility training beyond rehabilitation programmes. No research has been undertaken into participants’ experiences of attending these multidisciplinary, experience-based clinics. Research in this area is needed to ensure clinics meet intended goals, including understanding the motivation and experience of attendees. Insights may improve mobility clinics and inform strategies to encourage greater participation.
Objectives:
To explore the motivation of people with limb loss to attend a mobility clinic, the experience of participation and their perception of the clinic’s benefits.
Study design:
Qualitative methodology, naturalistic enquiry.
Methods:
Semi-structured interviews were conducted with nine clinic attendees during the clinic. Interviews were transcribed verbatim, data thematically analysed and emergent themes underwent member checking.
Results:
Three themes emerged from the data: facing the challenge captured how participants’ have adapted to amputation, valuing peers highlights the important role of peers in learning and support and improving mobility described the ongoing quest to improve mobility.
Conclusion:
The mobility clinic was attractive to those who liked challenges and was an invaluable source of learning for those wishing to improve their mobility. Future clinics should ensure that peer education is supported, and activities cater for a range of skills and fitness levels.
Clinical relevance
Findings of this study indicate that those who attended the mobility clinic liked to challenge themselves. Participation with peers was an important source of learning and support. Those participants who had previously attended a mobility clinic reported improvements in their overall daily function.
Background
Amputation is a life-changing event which alters the way people participate in activities that give meaning to life.1–3 While amputation often results in decreased confidence with balance, physical function and community engagement,4,5 most rehabilitation post amputation tends to focus on basic gait training, such as straight line walking or safe stair ascent with the intent of returning people home and to their community. 6 Higher level mobility training is not considered a requisite part of many rehabilitation programmes, and people are commonly discharged with some degree of mobility limitation. 7
Studies have addressed mobility for community-dwelling people with lower limb loss, and a recent narrative review examined strategies to improve balance and walking in this population. 8 They reviewed studies of sensory feedback, external perturbations, and stabilisation exercises programmes, and determined that these training modalities positively influenced mobility. However, in the extensive search method for their review, the authors did not identify studies providing training in other mobility skills, such as learning to fall, stepping sideways, jumping, hopping, skipping, stepping to recover, to name a few. This indicates that there appears to be a gap in research and/or conduct of this type of training.
In recent years, industry-led mobility clinics have been conducted in a number of countries to address this gap in mobility training. Through the use of lectures and physical training designed to improve confidence, balance, strength and prosthetic skill, these clinics are intended to extend gait and mobility training beyond that provided by most rehabilitation programmes. Learning opportunities in these clinics are structured to allow people with limb loss to hear from expert clinicians and therapists, and to be immersed in a peer learning environment. The peer environment enables participants to share their experiences and to learn new techniques developed from the experience of others. Utilising peers in this way is consistent with research in other areas of disability that reinforces the unique value of peers in contributing to health education. 9 Peer-delivered physical activity interventions have been found to be as effective as non-peer, professionally delivered interventions in increasing physical activity, while positively enhancing participants’ self-efficacy. 10
While these clinics have become increasingly popular in recent years, there has been no published research exploring participants’ experiences. Research would be useful to ensure that the clinics meet the mobility training needs of participants. In addition, in exploring participants’ motivations to, and expectations of attending the clinic, clinicians could gain an understanding of why people do not attend despite likely benefits to their mobility. In answering both these questions, clinicians might find ways to encourage greater participation, and thereby improve the ability to participate in activities that require high-level community mobility.
This qualitative study aimed to explore what motivated people to attend a mobility clinic, what the experience of participation was like and whether they perceived the clinic enhanced their mobility.
Method
Research design
This qualitative study used a naturalistic enquiry approach. A qualitative design was well suited to understand the events or situation from the perspectives of those with direct experience and knowledge. 11 The COREQ, 12 a 32-item checklist for reporting qualitative research, was used to guide reflexivity and study design.
Ethics approval for this research was obtained from La Trobe University Human Ethics Committee (HEC18068). All participants gave written informed consent to participate. The study was conducted with the approval of the company that ran the mobility clinic. The researchers who conducted this research project had no affiliation with the company running the mobility clinic, and the company had no role in data collection, analysis, interpretation or the decision to submit the research for publication.
Participants and setting
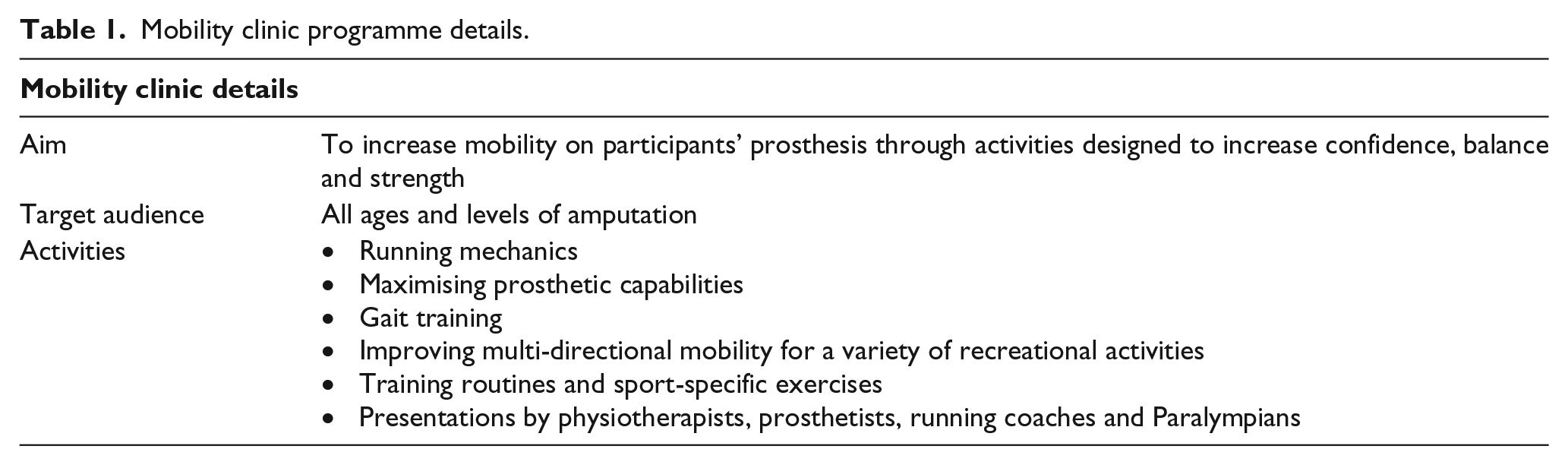
This study focussed on a 2-day mobility clinic run in a major metropolitan city in Australia (hereafter described as the clinic). The clinic was organised and run by an international orthotic and prosthetic company and involved formally structured education sessions with activity-based learning (Table 1). The clinic aims, intended audience, and activities are shown in Table 1. These clinics offer 2 days of tailored physical training sessions, lectures and peer support, teaching techniques to maximise prosthetic capabilities, improve running mechanics, speed, balance, multi-directional mobility including training routines and sport-specific exercises for a variety of recreational activities.
Mobility clinic programme details.
Eligibility criteria for inclusion in this study (but not the clinic itself) were attendance at the mobility clinic, age 18 years or above, able to participate in an interview in English and able to give informed consent in writing. Participants were recruited using convenience sampling.
Clinic organisers sent an email about the study to everyone who registered to attend. Participants who were willing to be interviewed contacted the researcher via email and, were sent information about the study prior to the clinic. The researcher then attended clinic registration and met those participants who had indicated willingness to participate to schedule an interview time. Everyone who was willing to participate in the study was interviewed. The final number of participants interviewed represented 50% of clinic attendees.
Data collection
An interview schedule was developed using ethnographic methodology from discussions with previous clinic attendees who contacted the researcher at the clinic organiser’s request. Using this type of emic ethnographic approach allowed for perspective of those who had attended the clinic to guide the development of the interview schedule. 13 The interview schedule included questions about demographic details, participants’ daily activities and experiences of the clinic, for example, questions about mobility included: ‘What are the most important aspects of mobility for you as someone who wears a prosthesis?’ and ‘What does it mean for you to be mobile on a good day? A bad day?’ (see Appendix 1 for interview schedule). Individual, face-to-face, semi-structured interviews were conducted by a researcher who is a prosthetist. Interviews occurred at the clinic, in a quiet area away from other participants. Interview duration was 47 min on average (range 21–51 min), and all interviews were audio-recorded.
Data analysis
Interviews were transcribed verbatim by a professional transcription company, and complete transcripts were entered into Nvivo 11 software 14 to manage, sort and analyse data. Thematic inductive analysis, as described by Liamputtong, 11 was used which included line-by-line coding, coding into a node structure, and then themes and subthemes were derived. Data were analysed by one author and themes and subthemes were reviewed by the other two authors to maximise rigour in concepts and theories derived from the data.15,16 No new themes were identified after the seventh of nine interviews were analysed, thus thematic saturation was reached. Five participants were randomly selected to be contacted to member check the emerging themes. Each was sent a copy of the themes, with a follow-up phone conversation from the original interviewer. No further data were suggested. The resultant themes identified the major concepts expressed in the interviews.
Results
Participants’ data were aggregated for presentation here due to the small, potentially identifiable cohort. Of the eighteen participants who attended the clinic, nine were interviewed. There were six women and three men. Ages ranged from 25 to 60 years, with an average of 43 years. Amputations resulted from trauma (four participants), medical reasons, such as diabetes or infection (four participants) and congenital insufficiency (one participant). One participant had unilateral transtibial amputations, five had bilateral transtibial amputations and three participants had unilateral transfemoral amputations. Time since amputations ranged from 2.5 to 24 years. This was the first clinic for four participants, the second clinic for two participants, and the third for three participants. Two participants had attended all four clinics run to date.
Themes
Three themes emerged from the data: facing the challenge, valuing peers and improving mobility. Each will be presented in turn.
Facing the challenge
Participants’ accounts of their lives all contained a strong undercurrent of facing challenges. The impact of amputation was felt across many aspects of participants’ daily lives and challenged participants’ views of a ‘normal’ life. They worked hard to maintain and create life roles, but that typically involved ceasing or changing activities. They saw this clinic as another opportunity to challenge themselves.
Regardless of the reason for amputation, all participants, with the exception of the participant with an amputation from a congenital cause, experienced changes in their daily lives. One participant described that her ‘normal was now challenged’ (Participant 9). Feeling different from others ‘I get self-conscious. I get tired. I get cranky. I don’t want to stand out in a crowd’ (Participant 1) and asking for help were two situations that were part of a new normal for participants I think the biggest thing with having a disability, . . . [is] having to tell somebody, I need some help . . . (Participant 5)
In adjusting to this new normal, participants worked hard to maintain their previous life roles and to create new ones. However, participants emphasised difficulties associated with amputation, particularly regarding parenting and employment. For example, employed participants reported being treated differently to other employees, and that their workplace typically did not understand fluctuations in their function, such as when they were unable to wear their prosthesis and required a wheelchair instead.
They’ll deny it, they would never ever admit to it. But I would say [the most difficult part of life is] work . . . I’ve noticed I don’t get asked to go to anything off site. Not one thing. (Participant 4)
Participants who were parents, listed activities they wanted to do with their children but they could not do.
I have raised my children differently because I don’t have legs . . . There’s a lot of things we don’t do, we don’t do camping, we don’t do anything water related really because that’s just too hard. We don’t go to the beach. I mean, we have gone to the beach but it’s not part of our life and I think I imagined we would do a lot more of that sort of thing. (Participant 3)
This clinic provided participants with another opportunity to challenge themselves. Participants cited other reasons to attend the clinic, such as providing support to others, seeking support themselves, increasing motivation to be active, challenge themselves and ‘being the best amputee [I] can be.’ (Participant 9) You sit in your little cocoon at home and you’re doing safe things and to me this wasn’t safe. This was like getting myself out there and challenging myself. Sometimes you need to get on a rollercoaster and scream your head off just to make yourself feel better and that’s how I saw the clinic. (Participant 8)
Participation in new activities posed a challenge to many participants who felt self-conscious or pressured participating in races, competitions or timed activities.
That relay was not super comfortable, doing that in front of everybody . . . because it was the obstacles, and because it’s supposed to be speed. If it was an obstacle and you were supposed to do it at walking pace that would be different. (Participant 6)
Valuing peers
Peers provided formal and informal support as well as learning opportunities during the clinic. Participants reported feeling as if they belonged to the group, and they could give and receive advice. They sought to continue building peer networks after the clinic. Some participants, however, felt self-conscious and daunted breaking into existing groups.
In general, peers played an important role for participants. Participants were comfortable around peers, learnt from them, and gave and received support. One participant described attending the clinics as ‘being part of the crew’ (Participant 4). Typically, participants reported having little contact with other people with amputation outside of these clinics.
What makes me feel comfortable is I’m with other amputees and I feel as though I can exhale. I feel as though I’m with my people kind of thing. The expectations are the same and no-one stares. Or if they stare it’s because they like your legs. (Participant 8)
Peer sessions, such as listening to Paralympic speakers, were part of the programme. However, participants looked for support from beyond these formal sessions. Peers provided informal learning opportunities during tasks, such as when participants watched others to see how they could improve their daily function.
I think it’s important for inclusiveness, for camaraderie. For learning techniques that aren’t in text books. You’re never going to publish how to brush your hair with one arm. There’s not a technical reason for it there’s just ways that you’re going to share practical skills. You don’t always get them in the forums. Not every state has an association, so that’s probably something to factor in. (Participant 2)
Being around peers at the clinic, participants felt encouraged, motivated and supported. Engagements with peers were positive and focused on future possibilities.
It’s nice to be with other amputees, with other amputees in a setting that’s very positive, very ability-focused rather than a support group with people sitting around . . . it’s absolutely forward-focused and it’s about, ‘this is what’s possible, let’s just do that’ . . . We all know how bad things can get, so we don’t, you know, we can share that privately, but I think situations like this are about that positivity is absolutely important. (Participant 9)
Several participants stated they would make an effort to maintain peer relationships and be active in the community of people with limb loss. Ongoing peer relationships were recognised as a way to relieve the isolation of amputation felt by some participants.
I think you need to be active and you need to contribute to the community around you or it’s isolating. I think for me amputation is isolating because it’s not recognised. So that’s why something like this is critical because the whole space isn’t recognised because it doesn’t fall under an umbrella. It’s not a disease, it’s not diabetes. It’s not epilepsy, it’s not cancer: It’s the result of. So because of that you need the camaraderie and the focused targeted workshops at things like this, to actually achieve specific results. (Participant 2)
Despite valuing peers, participants sometimes felt self-conscious in involving themselves in the clinic’s social aspects. They reported feeling daunted in breaking into ‘cliquey’ groups formed in previous clinics (Participant 2). The value and difficulty of participating in group activities is clearly described in the quote below:
do you think the group environment helps or hinders?
It can be a bit of both. It can help in the fact that you get to see other people and talk to other people and experience it with them. It can be a hinder if you’re not the kind of person that can handle doing those kind of things in front of others, it can sort of delay your process because you’re not quite as ready to put it out there. (Participant 5)
Improving mobility
Participants’ previous rehabilitation had largely focused on basic gait skills, while enhanced mobility was often self-taught. They saw this clinic as a way of improving their existing mobility skills.
While participants reported having sufficient mobility skills to manage in their daily lives, they looked to the clinic to improve their mobility skills and knowledge. In particular, they wanted to improve high-level mobility, such as walking on uneven surfaces, walking up and down stairs, moving in a crowd, and being able to move quickly in an emergency. They also wanted to improve mobility that would enhance their enjoyment of life such as taking their children to the beach, dancing, jogging, playing soccer with their children, riding a motorbike and sailing.
In terms of day-to-day, I can get to work, I can earn money, I can get home, I can pick my kids up. I’ve got the stamina to do all of that and turn around and do it all again the next day. So, in terms of my basic requirements, no. But in terms of adding value to my life, yeah, I’ve got a lot of [mobility] goals. (Participant 4)
All participants had undertaken hospital-based rehabilitation, either as an inpatient or an outpatient. However, most described this rehabilitation as basic and focused on gait training only. For many, formal rehabilitation ended when participants mastered the basics. More extended mobility skills were self-taught or learnt from informal sources, such as other people with similar amputations.
I think I only went to outpatient rehab like a total of four times. At that point my mindset was, I can do this, and their mindset was, well, if he’s not falling over in a heap then he’s good to go. We kind of mutually agreed that we don’t need any more help and off we went. (Participant 4) I taught myself . . . It didn’t feel comfortable and I didn’t like it to begin with, there were a few teething problems, so I just worked on it and worked on it and worked on it until I got past it. (Participant 5)
when you received your new components did you have any gait training or rehab training with them?
No . . . I finished my rehab. I was no longer an out-service rehab person, I just learnt from talking to other amputees?”
Participants described situations when their prosthesis did not meet their mobility needs to undertake specific tasks. This included where participants attempting to walk up hilly terrain without a prosthesis with a flexible ankle, go to the beach without a water-proof prosthesis, and run in a non-running prosthesis, the type of equipment reduced their ability to mobilise and participate.
I don’t do hikes and things because my feet aren’t great. There’s no great energy return in them . . . I’m not on [new funding scheme] yet . . . Even if my form went in today I’ve got to wait 12 months for them to think about it. So I’m in the process of asking how much it is to buy my own feet. (Participant 4)
Some participants sought to improve their mobility and thereby reduce concentration, mental effort and fatigue particular in activities that involved different terrains or moving through a crowd.
There have been technology changes that have vastly improved my mobility, but do I still feel like I struggle with mobility? Yeah, of course. In every amputee’s mind, there is a reserved compute space and memory space that is allocated to paying attention to things that other people don’t pay attention to. You have a much more limited energy budget. You have to spend it wisely. You have to be parsimonious at times and that can be frustrating. (Participant 4)
At times of lowered mobility, some participants were forced to curtail activities, while others chose to use mobility devices, such as a wheelchair or walking frame. However, several participants avoided using a wheelchair, particularly in the workplace, because they associated it with visible and increased disability, and therefore being treated differently to their colleagues. Participants showed the importance they placed on their mobility and the perceptions of being less mobile.
If you rock up to work in a wheelchair and they go, ‘Oh, what, you just couldn’t be bothered walking today’. Your employers don’t get it and that’s the hardest thing because you then have to justify to everyone else why you can’t get your leg on. (Participant 7)
Attending the clinic typically improved participants’ mobility skills. One participant explained that the clinic acted as a reminder of the skills she already had. Mostly, however, participants were enthusiastic about improving their mobility skills, commenting that clinic presenters were the first to show them specific exercises since their rehabilitation. Those participants who had attended previous clinics reflected on how their mobility had improved. Running was typically mentioned by participants as improving after the clinic. Whereas, one participant was unable to explain a specific improvement and described an increase in general movement.
It’s really subtle things like cleaning up around the house, so it’s partly stamina but also just movement that I do that I probably wouldn’t have done before, and it’s really hard to explain exactly what it is but there are just–it’s just the way I move is easier. (Participant 3)
Discussion
This research explored mobility clinic participants’ motivations to attend, experiences of the clinic and perceptions of enhancements to mobility skills. Unlike studies that focus on quantitative outcome measures, these individual interviews concentrate on the experience that may be missed, but which may also have an impact on the outcomes of a mobility clinic. As little is currently known about how individuals experience mobility clinics, our findings provide a novel insight into this under-researched area. Three key themes encapsulate the experience of clinic attendees: facing the challenge, valuing peers and improving mobility. Based on these results, several observations are worth highlighting.
First, participants’ motivations to attend the clinic appeared to be strongly linked to their willingness to take on challenges, that is, participants’ who desired to push themselves beyond their perceived limits showed a high level of motivation to achieve their best. This result is consistent with another qualitative study of people with limb loss, which identified that coping resources and the meaning associated with events determined whether participants saw their day, as ‘good’ or ‘bad’; 3 this held true even though they experienced pain and curtailed activities on most days. For participants in this study, facing ongoing challenges allowed them to participate in meaningful activities.
Despite being highly motivated, participants had limited prior opportunity to access any form of mobility, gait or prosthetic training outside of their prosthetic service. This lack of opportunity is concerning given the benefits training can have on mobility, participation, function and quality of life in people with limb loss.4–7,17 This finding also raises the possibility that people who choose not to enroll in a clinic may not be ready to seek challenges. Investigating the motivation and mobility needs of those who did not attend may enable a programme to be targeted to others who may also benefit from extended mobility training.
A second observation of note is that peers were frequently mentioned when participants spoke of their positive clinic experiences. The role of peers in gaining physical skills has had limited exploration within the amputation and prosthetics literature;18,19 however, our findings are consistent with research with a wider ‘disability’ lens,9,10 in which peers are seen to have knowledge beyond that of health staff. The findings of positive responses to informal peer education should be studied within other programmes and explored in a wider population with limb loss.
A final observation to highlight was that participants reported having enough mobility skills for basic daily living tasks, such as personal care and domestic tasks, but they enrolled in the clinic to advance or develop their skills to meet their life activity goals. The literature has shown that increased gait skill is linked to an improvement in mobility. 20 However, rarely is mobility seen as a skill that can be taught; instead, it is viewed as an outcome measure that is influenced by gait ability.18,20 The clinic appears to meet a key aspect of rehabilitation that is currently missing from the participants’ health experience which influences peoples’ ability to participate. Higher levels of physical participation have been shown to positively impact quality of life along with other key outcomes, such as greater community participation.4,5 This key finding suggests that higher level mobility training in rehabilitation programmes for people with limb loss may result in higher level functional goals and aims.
There are several recommendations that arise from this study. Future education and clinics should look to capitalise on and, create opportunities for both formal and informal peer learning. A variety of activities, including games and simulations of daily activities, that appeal to wide ranging demographics and fitness levels would be ideal. It is important that clinics that are run by manufacturers, follow the lead of this clinic and focus on these as a means to improve mobility for people with limb loss regardless of componentry. A final recommendation is that singular clinics left participants wanting more, so planning for regular events or additional training options would be beneficial.
There are several limitations that readers should keep in mind to contextualise the findings of this study. It is important to note that participants had chosen to attend the clinic. This group may be more motivated to improve their mobility than those who did not attend. While this is addressed in the discussion, it is important to note that the mobility of those interviewed varied. Some participants used assistive devices such as crutches along with their prosthesis, while others were capable of high-level and high-impact mobility independent of any gait aids. While the participants varied from 25 to 60 years, they were a relatively young and arguably healthy population without the long-term effects of age-related decline. The experience of participants may also vary depending on their level of amputation and the limb of limbs affected.
The fact that these experiences are based on one clinic could be seen as a limitation to this study. However, only one mobility clinic is run in Australia each year, with many repeat attendees. As such this is likely to be representative of experience at this clinic.
Conclusion
The aim of this study was to explore what motivated people to attend a mobility clinic, what the experience of participation was like, and whether they perceived that the clinic enhanced their mobility. This is the first study to address this area and identifies several important factors which may have an impact on future clinics. Findings of this study indicate that those who attended the clinic liked to challenge themselves, and they highlighted the importance of peer education and peers as a source of learning. Findings also indicate that participants identified that they felt their mobility improved as a result of attending. Future clinics should ensure that the importance of peer education is not overlooked, and a range of skills and fitness levels are catered for. Furthermore study is warranted to quantify mobility changes along with exploring reasons why people might not attend.
Footnotes
Appendix 1
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for this project was provided by Össur ehf, R&D, Medical Office, Iceland.