
Abstract
Background:
Clinicians use the Activities-specific Balance Confidence Scale to understand balance confidence. A short-form Activities-specific Balance Confidence scale, was developed using the six most difficult tasks from the original Activities-specific Balance Confidence scale; however, short-form the short-form scale psychometrics and agreement with the original scale have yet to be explored in people with lower extremity amputations.
Objective:
To determine the relative and absolute reliability, construct validity, and agreement of the short-form Activities-specific Balance Confidence scale.
Study design:
Test–retest with a 2-week interval.
Methods:
Analysis for relative reliability and internal consistency was intraclass correlation coefficient and Cronbach’s α, respectively. Absolute reliability was measured using standard error of measurement and minimal detectable change. Bland–Altman plots measured agreement between scales. Construct validity was evaluated against the L Test using a Pearson-product moment correlation.
Results:
The short-form Activities-specific Balance Confidence (intraclass correlation coefficient = 0.92) and Activities-specific Balance Confidence (intraclass correlation coefficient = 0.91) scales had excellent relative reliability. Both scales demonstrated good internal consistency. Worse absolute reliability was observed in the short-form Activities-specific Balance Confidence scale. Construct validity against the L Test was confirmed. Bland–Altman plots indicated poor agreement between scales.
Conclusion:
Both scales exhibit excellent relative reliability and good internal consistency and construct validity. Poor agreement between short-form Activities-specific Balance Confidence and Activities-specific Balance Confidence indicates the scales should not be used interchangeably. Inadequate absolute reliability of the short-form Activities-specific Balance Confidence scale suggests the Activities-specific Balance Confidence should be the balance confidence scale of choice.
Clinical relevance:
Balance confidence is an important metric for our understanding of rehabilitation and community re-integration in people with lower extremity amputations. Due to inferior absolute reliability and a lack of appropriate items composing the short-form Activities-specific Balance Confidence scale, the full-scale Activities-specific Balance Confidence is recommended for the assessment of balance confidence in this population.
Background
Falls are prevalent in people with lower extremity amputations (PLEA), with reports of 52.4% of community-dwelling PLEA falling each year. 1 Common consequences of falling for PLEA are physical injuries and developing a fear of falling. Importantly, a fear of falling for PLEA is associated with a reduction in daily activity levels and social participation, and can result in decreased quality of life. 2
Valid and reliable scales for measuring a concern of falling have been established; one of the most prominent is the Activities-specific Balance Confidence (ABC) Scale. 3 This scale was developed for use in community-dwelling older adults and includes 16 questions addressing balance confidence during the performance of daily activities. 4 Balance confidence is a balance specific type of self-efficacy used to measure fear of falling. 5 The validity and reliability of the ABC have been established in a number of populations,3,6–9 including transtibial and transfemoral PLEA. 10
The ABC is recommended as a tool to track rehabilitation progress in PLEAs; 11 however, the ABC can be time-consuming and in clinical settings clinicians may not have the time. For this reason, a shortened version, the ABC-6, was developed using the six most difficult questions from the ABC to provide a quantitative assessment of balance confidence. 12 Psychometric properties of the ABC-6 have been established in community-dwelling older adults 4 and older adults with diabetes. 13 It is important to establish the reliability of the ABC-6 in PLEA, as the relevance of the reduced number of items may not be consistent with community-dwelling older adults due to the impact of factors specific to PLEA, such as the level of amputation.
The objectives of this study were to determine (1) the test–retest, internal consistency, and absolute reliability of the ABC-6, (2) the agreement within the ABC-6 and between the ABC-6 and the ABC, and (3) the construct validity of the ABC-6 in PLEA. It was hypothesized that test–retest reliability and overall internal consistency would be excellent for the ABC-6, and that absolute reliability measures would be comparable to the ABC. Strong within and between scale agreement was hypothesized. Both scales were hypothesized to have a statistically significant, moderate negative correlation with walking tests, whereby a higher ABC-6 score would be associated with shorter times to complete tests.
Methods
Design and participants
This was a test–retest study of individuals attending a regularly scheduled appointment with their physician in the outpatient clinic for PLEA at Parkwood Institute in London, Ontario, Canada. The study was approved by the Health Sciences Research Ethics Board at the University of Western Ontario and by the Clinical Resources Impact Committee of Parkwood Institute (REB# 107472). All study participants provided written and signed informed consent. Recruitment took place from 24 March 2016 to 19 January 2017.
Eligibility criteria were 18 years or older, functional use of the English language, major lower extremity amputation (defined as a transtibial level or higher), using their prosthesis for walking, and using the prosthesis for at least 6 months as to ensure that participants were past acute phases of recovery and had enough experience walking. 14 Exclusion criteria were any physical or medical problem that significantly limited ambulation with a prosthesis (e.g. only using the prosthesis for transfers or current problems with the residual limb that limited ambulation) or if the individual did not have a prosthesis. Three groups of PLEA were recruited, those with (1) a unilateral transtibial amputation of vascular etiology (TTA-vas), (2) a unilateral transtibial amputation of nonvascular etiology (TTA-nonvas), and (3) complex amputations (transfemoral amputation (TFA) or bilateral amputation of any etiology). Groups were selected based on etiology and functional differences to ensure representation from a variety of PLEA subpopulations.15,16 Compared to transfemoral or bilateral PLEA, those with a transtibial level amputation demonstrate better walking abilities. 17 The specific group selection described allows for sensitivity analysis among the subgroups that has previously proven to be useful. 18
Eighty-one individuals were approached for inclusion, and 68 were enrolled. Of the 13 individuals not enrolled in the study, 61.5% (n = 8) lived too far from the center to return for the follow-up assessment, 23.1% (n = 3) did not have time to complete the initial testing, and 15.4% (n = 2) declined participation. In addition, 8 of the 68 participants enrolled were unable to return for the retest assessments within 14 days for the following reasons: illness (2), transportation (2), scheduling issues (1), or other reasons (3).
Self-reported demographic and medical history information from participants were age, sex, years of education (highest grade completed starting with grade one), primary etiology, number of comorbidities (determined using a standardized checklist), duration of amputation, mobility aid used, and history of falls in the past 12 months. Height and weight were collected by the clinic’s nurse while the participant was wearing their prosthesis, and the number of prescription medications was extracted from the participant’s medication list. When necessary, demographic and medical information was confirmed via medical charts. Global cognitive status was measured by the Montreal Cognitive Assessment (MoCA). 19 Falls were defined as “an unexpected event in which the participants come to rest on the ground, floor, or lower level.” 20
Measures of balance confidence
Balance confidence was measured using the ABC Scale 3 and the shortened version of the scale, the ABC-6. 12 The ABC was first developed for use in community-dwelling older adults. 21 The ABC asks participants to rate their level of confidence in completing 16 daily activities without losing their balance or falling, using a scale from 0% (no confidence) to 100% (completely confident). 4 A mean of the 16 items is taken as the overall score and reported as a percentage. 3 This scale has demonstrated reliability, validity and internal consistency in unilateral transtibial and transfemoral PLEA, aged 20 years or older, and experienced with the use of a prosthesis for walking. 10
The short-form Activities-specific Balance Confidence (ABC-6) Scale was developed by Peretz and colleagues and uses six items from the ABC. 12 The six tasks in the ABC-6 were chosen by identifying items that had the lowest scores, and therefore, the most difficulty, among individuals with Parkinson’s disease and healthy participants. 12 Balance confidence using the ABC-6 was calculated by taking the mean of participants’ scores on these six tasks and was reported as a percentage. In the present study, the ABC was administered via a face-to-face interview and ABC-6 scores were derived from the items completed in the ABC.
Measure of functional mobility
Functional mobility was measured using the L Test of Functional Mobility (L Test), a standardized assessment developed for PLEA. 22 Participants start from a seated position on a standard armless chair (height: 46 cm, arm height: 67 cm), and when instructed, stand from the chair, walk 3 m, turn 90°, walk 7 m, turn 180°, and walk back to the starting seated position. 22 Participants were asked to walk at their usual pace and were timed to the nearest hundredth of a second using a stop watch. The L Test was completed under two conditions: (1) single-task (walking alone) and (2) dual-task (walking while performing serial subtraction by threes). 18 Participants performed single-task trials prior to dual-task trials with a 5 min seated rest in-between conditions. Activities of daily living frequently involve simultaneous performance of two or more tasks; as such dual-task gait testing may better equate to performance on everyday activities, compared to the single-task. 23 Moreover, anxiety related to the fear of falls has been shown to act as a cognitive distractor in community-dwelling older adults, adversely affecting walking performance and increasing instability. 24 The dual-task L Test has demonstrated reliability in PLEA. 25 No instructions were given to the participant regarding task prioritization during dual-task testing.
Analysis
An a priori power analysis with α = 0.05 and β = 0.20 determined that a total sample of 20 participants was necessary if a target intraclass correlation coefficient (ICC) value of 0.90 with a lower confidence interval (CI) of 0.70 was desired. Normality was assessed for all continuous variables using the Shapiro–Wilks test, z-scores generated from indices of kurtosis and skewness, and visual inspections of histograms and normal Q–Q plots. Using boxplots, outliers were defined as values 1.5 times outside the interquartile range, while values 3.0 times outside were considered extreme outliers. Two outliers were identified for the ABC and ABC-6 prior to ICC analysis; however, there was no evidence of erroneous collections and their performance was consistent on both testing dates. The data from the outliers were kept as they were determined not to be extreme, and there was no indication that their inclusion would lead to drastically different results or interpretation. Participant demographic and clinical information were summarized using means and standard deviations (SDs) or frequencies and percentages, as appropriate.
The test–retest reliability of the ABC-6 and ABC was evaluated using the ICC. ICC values equal to or higher than 0.90 are considered excellent, 0.80–0.89 are considered good, 0.70–0.79 are considered fair, and values below 0.70 are considered clinically questionable. 26 Internal consistency was examined using Cronbach’s α. The impact of each item on the overall internal consistency was evaluated using a step-wise item deletion method. Cronbach α values above 0.80 are considered good, while values over 0.90 indicate item redundancy. 27 Two measures of absolute reliability were calculated: standard error of measurement (SEM) and minimal detectible change with a 95% confidence interval (MDC95). The SEM is the measurement error associated with a single value and is expressed in the same units as the scale, 28 in this case, balance confidence from 0% to 100%. The smaller the SEM, the greater the absolute reliability. 28 The MDC95 is an estimate of the smallest change in the score that can be detected beyond measurement error. 29 It is also measured in the same units as the measurement scale. For the present study, the SEM was calculated using pooled SD values and the generated ICC values for each group. 28 Calculations of SEM and MDC95 were:


Agreement within each scale and between the ABC-6 and ABC were quantified using Bland–Altman plots. 30 A Bland–Altman plot displays the difference in balance confidence scores between the two testing sessions or the two tests against the mean of the sample balance confidence scores. Construct validity was evaluated using a Pearson product-moment correlation analysis between both the ABC-6 and ABC scales and the L Test. All statistical analyses were performed using SPSS version 25.0 (IBM Inc., Chicago, IL, USA).
Results
A total of 60 participants completed the study (age = 58.2 ± 12.6 years, duration of amputation = 13.2 ± 15.2 years), 20 in each of the 3 groups described (Table 1). The complex amputations group consisted of 15 individuals with TFA (75.0%) and 5 with bilateral TTA (25.0%). For the total sample, 26 participants (43.3%) reported experiencing a fall in the previous 12 months. In addition, the average MoCA score was 26.5 ± 2.2 points (min: 21, max: 30) and indicate that 43 (71.7%) participants had a normal cognitive status, while 17 (28.3%) were considered to have mild cognitive impairment. 19 Single-task L Test took a shorter time to complete (30.3 ± 13.3 s) than the dual-task condition (35.6 ± 15.6 s).
Demographic characteristics of participants, people with a lower extremity amputation, for total study population and three subgroups based on etiology and level of amputation.
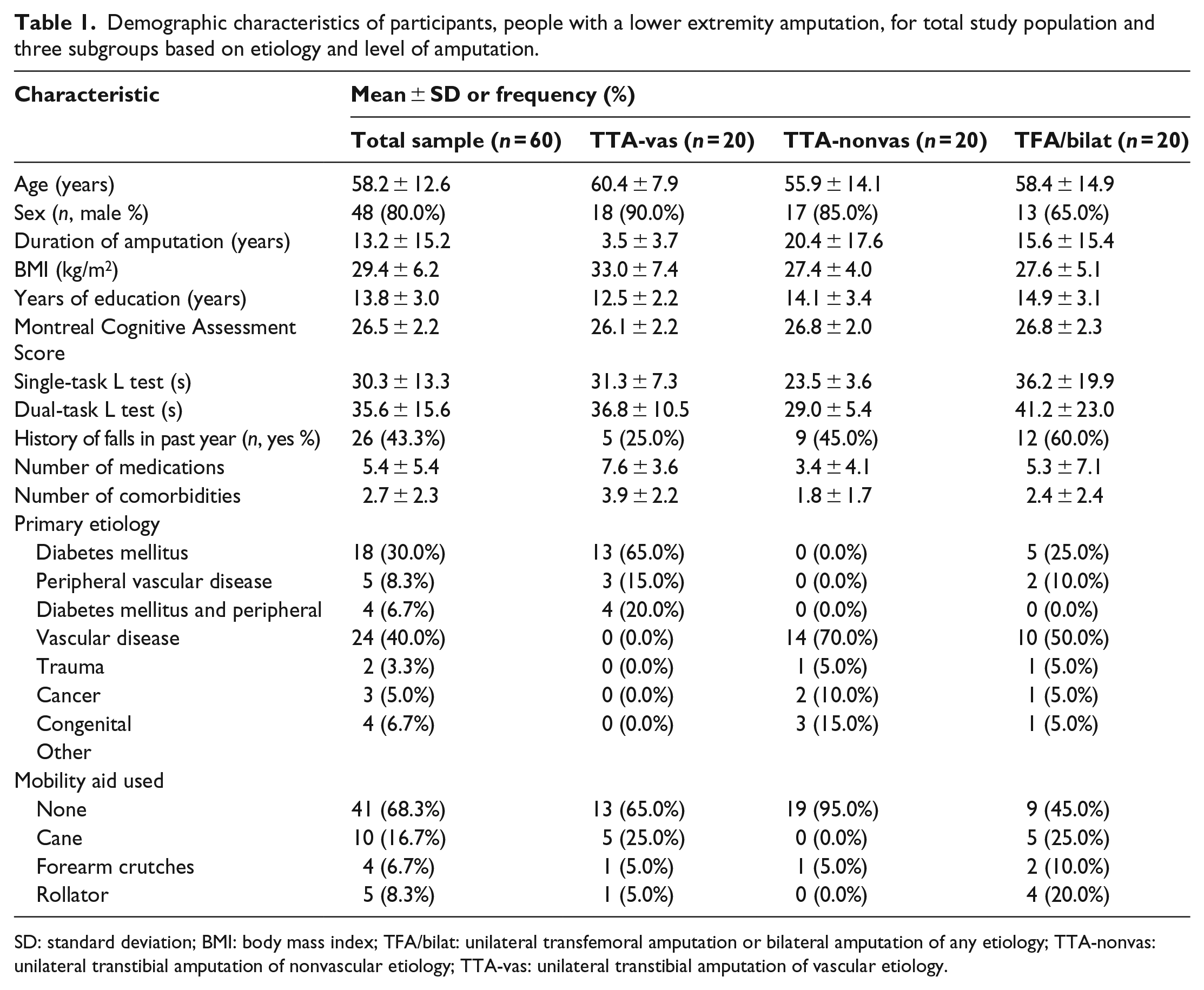
SD: standard deviation; BMI: body mass index; TFA/bilat: unilateral transfemoral amputation or bilateral amputation of any etiology; TTA-nonvas: unilateral transtibial amputation of nonvascular etiology; TTA-vas: unilateral transtibial amputation of vascular etiology.
The test–retest reliability values are presented in Table 2. On average, similar scores on the ABC-6 for the total sample were observed at the initial (63.90 ± 28.43, Min: 0.00, Max: 100.00) and retest (64.69 ± 26.32, Min: 3.33, Max: 100.00) assessments. The test–retest reliability was considered excellent for the ABC-6 in the total study population (ICC = 0.92, 95% CI: 0.87–0.95), the TTA-nonvas group (ICC = 0.95, 95% CI: 0.87–0.98), and the TFA/bilateral group (ICC = 0.90, 95% CI: 0.76–0.96), but was considered good in the TTA-vas group (ICC = 0.88, 95% CI: 0.72–0.95). Overall, the internal consistency of the ABC-6 was good (Cronbach’s α = 0.88), and step-wise item deletion resulted in Cronbach’s α values ranging from 0.83 to 0.88.
Scores, test–retest reliability, standard error of measurement, and minimal detectable change for the short-form Activities-specific Balance Confidence (ABC-6) and Activities-specific Balance Confidence (ABC) Scales.
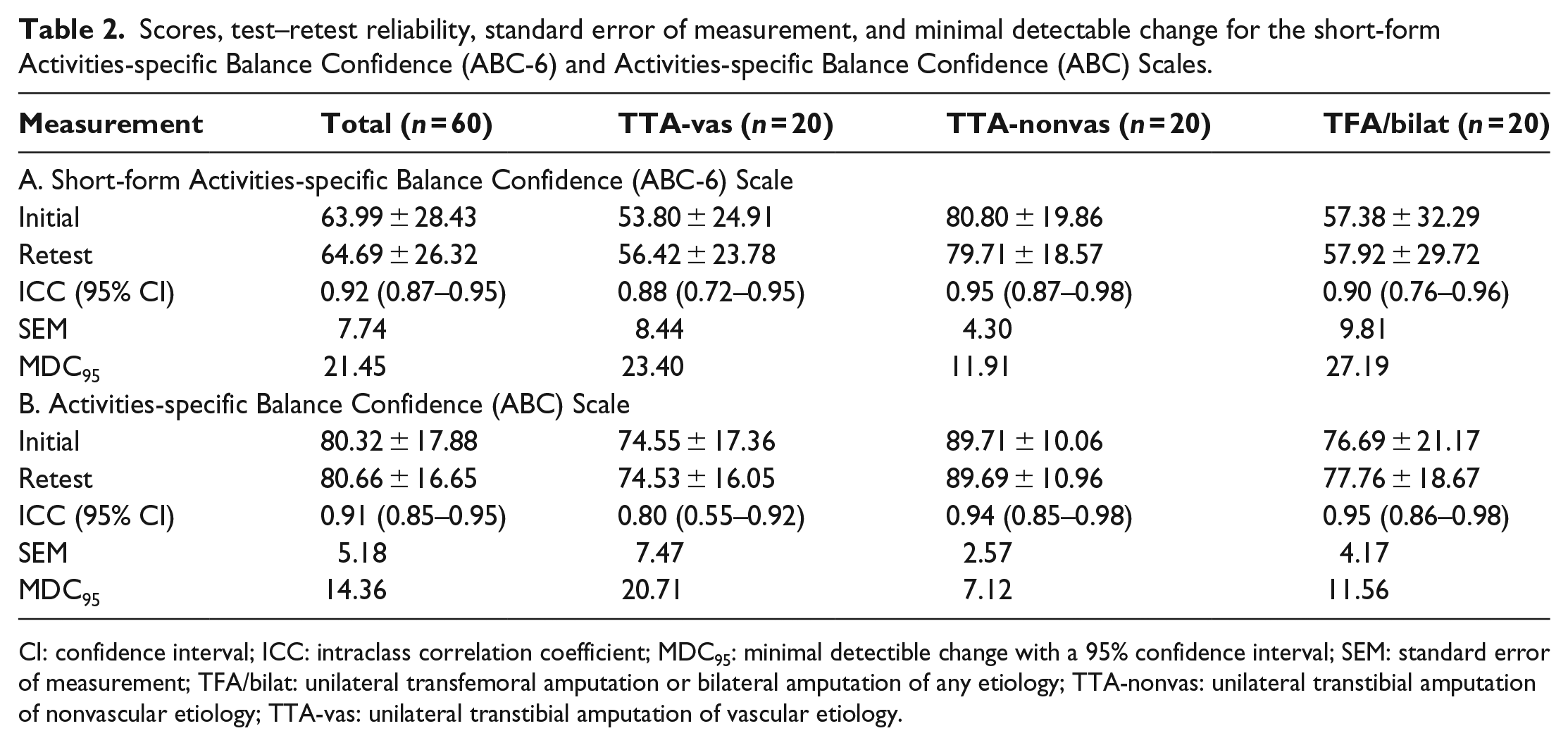
CI: confidence interval; ICC: intraclass correlation coefficient; MDC95: minimal detectible change with a 95% confidence interval; SEM: standard error of measurement; TFA/bilat: unilateral transfemoral amputation or bilateral amputation of any etiology; TTA-nonvas: unilateral transtibial amputation of nonvascular etiology; TTA-vas: unilateral transtibial amputation of vascular etiology.
For the total sample, the initial ABC score was 80.32 ± 17.88 (Min: 20.63, Max: 100.00) and retest was 80.66 ± 16.65 (Min: 35.31, Max: 100.00). The test–retest reliability for the ABC was considered excellent in the total study population with an ICC of 0.90 (95% CI: 0.85–0.95). Excellent test–retest reliability was also found in two of the subgroups: TTA-nonvas (ICC = 0.94, 95% CI: 0.85–0.98) and TFA/bilateral (ICC = 0.95, 95% CI: 0.86–0.98). The relative reliability of the ABC in the TTA-vas group was good (ICC = 0.80, 95% CI: 0.55–0.92). Internal consistency for the ABC was good (Cronbach’s α = 0.92), and step-wise item deletion resulted in Cronbach’s α values ranging from 0.91 to 0.92.
For the ABC-6, the SEM of the total study population was 7.74 points, with the highest SEM in the TFA/bilateral group and the lowest SEM in the TTA-nonvas group (Table 2). Results for the ABC demonstrated an SEM of 5.18 points for the total study population, with the TTA-vas group having the highest SEM and the TTA-nonvas group having the lowest SEM. For the ABC-6, the MDC95 of the total study population was 21.45 points, while for the ABC, the MDC95 was lower at 14.36 points. This trend was observed across all three groups tested with the greatest difference found within the TFA/bilateral group (ABC-6: 27.19 points, ABC: 11.56 points).
The Bland–Altman plot for the ABC-6 demonstrated good agreement (Figure 1(a)). Good agreement was also observed within the ABC (Figure 1(b)). This finding was exhibited for both the ABC-6 and ABC in each of the three groups (Supplemental Appendix 1, Figures i and ii). There was poor agreement between the ABC-6 and ABC for the total study population with the bias at 19.58 (Figure 1(c)). Poor agreement between the ABC-6 and ABC was also demonstrated for each of the three groups (Supplemental Appendix 1, Figure iii).
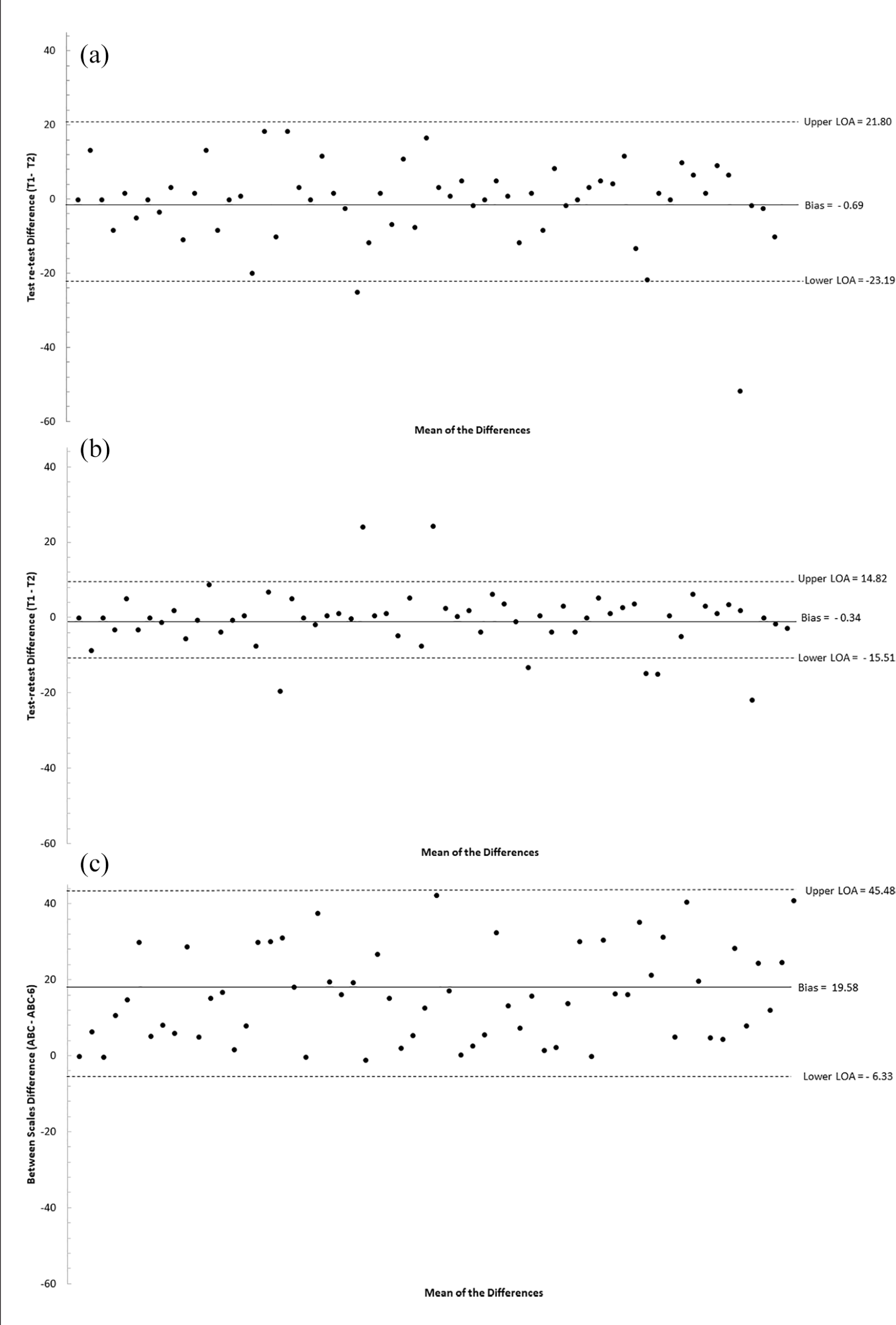
Bland–Altman plot for the agreement between (a) the ABC-6, (b) ABC, and (c) the ABC-6 and ABC in a sample of adults with a lower extremity amputation (n = 60).
Construct validity was statistically significant for both the ABC-6 and the ABC across the two L Test conditions. For the ABC-6, the hypothesized associations were observed for the single-task (r = −0.68, p < 0.001) and dual-task (r = −0.64, p < 0.001) conditions (Figure 2(a) and (b)). Similar values for the full-scale ABC were observed (single-task: r = −0.72, p < 0.001; dual-task: r = −0.68, p < 0.001).
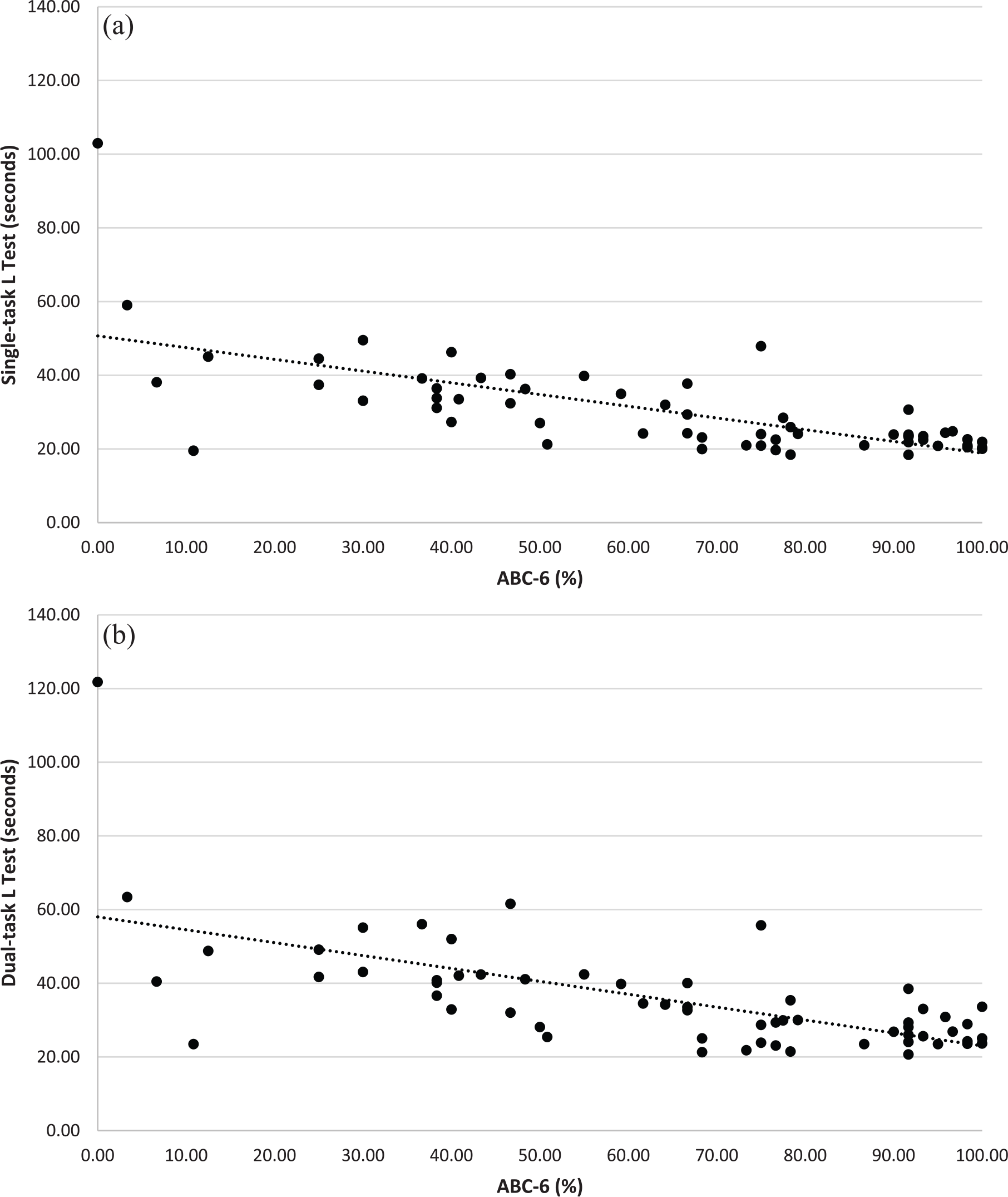
Scatterplot of the relationship between the ABC-6 and (a) single-task and (b) dual-task L Test scores in a sample of adults with a lower extremity amputation (n = 60).
Discussion
This study has demonstrated that the ABC-6 has good internal consistency and excellent relative reliability, yet worse absolute reliability than the ABC. The ABC-6 reliability values are a novel addition to the literature, while the values for the ABC were consistent with previous literature. 10 In addition, both scales demonstrated good construct validity. Agreement within each scale was good. However, the agreement between the ABC-6 and ABC was poor, indicating that one measure cannot be substituted for the other.
Using a 5-option response ABC scale in a sample of older adult PLEA, Sakakibara et al.’s work confirmed that the most difficult items of the ABC scale are those composing the ABC-6. 31 The resultant large ABC-6 SEM and MDC95 values observed in our study are likely a reflection of the difficulty of the items. It can be argued that items in the ABC-6 are not only the most difficult, but also the least likely to be performed by PLEA. For difficult items not performed by PLEA, such as stepping on/off an escalator while holding a parcel, a respondent would need to rely on mental imagery of a hypothetical scenario to estimate impact. No study to our knowledge has examined the relevance of items included in the ABC in PLEA.
Good agreement between the ABC-6 and the ABC has been found in individuals with higher-level gait disorders, Parkinson’s disease, and community-dwelling older adults. 12 The lack of agreement in our study indicates that the ABC-6 and ABC should not be used interchangeably. Prognostic thresholds for these scales have not been established in PLEA, though among community-dwelling older adults an ABC Score below 80.0% is associated with lower physical function and used as a clinical marker for intervention. 32 In our study, ABC scores were on average 19.58 points higher than ABC-6 scores. Therefore, the interpretation of ABC-6 scores with the ABC threshold would result in false positives, initiating clinical intervention that would not otherwise have been implemented had the testing been done using the ABC.
Higher balance confidence was related to faster times on the single and dual-task L Test conditions for both the ABC-6 and the ABC. The strength of the correlation between the ABC and the L Test was greater in our study (r = −0.72) than that observed by Deathe and Miller (r = −0.48). 22 This difference may be related to participant characteristics as our study included bilateral PLEA, while Deathe and Miller 22 recruited only unilateral transtibial or transfemoral PLEA. To our knowledge, this is the first time the ABC-6 and ABC scales have been validated against the L Test under a dual-task condition.
This study contains limitations worth noting. First, a convenience sample of PLEA attending an outpatient clinic was used, and therefore, it is not representative of all PLEA, specifically those non-ambulatory or that only use a prosthesis for transfers. While the majority of our sample population was male, which is representative of the sex distribution in PLEA,33,34 there is no evidence for difference in ABC scores by sex. 35 There were a number of strengths to this study, including the sample size of 60 participants and an a priori explicit recruitment of three groups based on etiology and level of amputation. Our sample size was adequately powered for the analyses in the complete sample and each of the three subgroups.
Conclusion
This study determined that there was good internal consistency and excellent relative reliability for both the ABC-6 and the ABC. In addition, the two scales demonstrated good construct validity against a functional mobility test under single- and dual-task conditions. Compared to the ABC, the ABC-6 had worse absolute reliability across all three subgroups. Particularly notable was the determination of poor agreement between the ABC-6 and ABC in this population. The main clinical implications are that these two measures should not be used interchangeably. Based on the lack of appropriate items for PLEA and the inferior ability to detect change using the ABC-6, the authors recommend only the use of the full-scale ABC for the examination of balance confidence in PLEA.
Supplemental Material
875623_APPENDIX_1 – Supplemental material for Reliability, validity, and agreement of the short-form Activities-specific Balance Confidence Scale in people with lower extremity amputations
Supplemental material, 875623_APPENDIX_1 for Reliability, validity, and agreement of the short-form Activities-specific Balance Confidence Scale in people with lower extremity amputations by Katherine Fuller, Humberto Adolfo Omaña Moreno, Courtney Frengopoulos, Michael W Payne, Ricardo Viana and Susan W Hunter in Prosthetics and Orthotics International
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Frederick Banting and Charles Best Canada Graduate Scholarships-Master’s award from the Canadian Institutes of Health Research and the Faculty Research Development Fund from the Faculty of Health Sciences at the University of Western Ontario.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.