
Abstract
Background:
Different types of foot orthoses have been prescribed for patients with flatfoot. Results of several studies have shown that orthoses were able to change balance parameters in people with flatfoot. However, the possible effect of orthosis flexibility on balance has not yet been investigated.
Objectives:
The aim of the current study was to investigate the immediate effect of a rigid University of California Berkeley Laboratory (UCBL) foot orthosis, a modified foot orthosis, and a normal shoe on the postural sway of people with flexible flatfoot.
Study design:
Quasi-experimental.
Methods:
In all, 20 young adults with flatfoot (aged 23.5 ± 2.8 years) were invited to participate in this study. The Biodex Stability System was employed to perform standing balance tests under three testing conditions, namely, shoe only, UCBL, and modified foot orthosis. Total, medial–lateral, and anterior–posterior sway were evaluated for each condition.
Results:
The results of this study revealed no statistical difference in the medial–lateral and anterior–posterior stability indices between foot orthoses and shoed conditions. The overall stability index with the UCBL foot orthosis, however, was significantly lower than that with the modified foot orthosis.
Conclusion:
The UCBL foot orthosis was able to decrease total sway and improve balance in people with flexible flatfoot.
Clinical relevance
Results of previous studies have indicated that foot orthoses were able to affect the balance of people with flatfeet. However, the possible effects of flexible orthoses on balance have not been examined. The results of this study may provide new insight into material selection for those people with balance disorders.
Keywords
Background
Flatfoot (pes planus) is defined as a partial or total collapse of the medial longitudinal arch of the foot. 1 It has been classified into two categories, namely, flexible and rigid flatfoot, based on the presence or absence of the arch in a non-weight-bearing position. It may develop unilaterally or bilaterally.
The medial longitudinal arch of the foot plays a critical role in the normal mechanics of the foot. Any increase or decrease in this osteoligamentous arch changes the normal function of the foot and triggers damage to the feet and the whole body. 2 Flatfeet change the pressure distribution pattern and alter the position sense of the foot joints, which causes an inability of the foot to accommodate to theterrain. Previous studies revealed that both static and dynamic balance in people with flatfeet largely depend on the environmental and inherent characteristics of the base of support, and any variation in these conditions could negatively affect balance. 3
Various therapeutic approaches, including exercise therapy, surgery, and orthoses, have been used to tackle the above mentioned problems. Foot orthoses are classified into three sub-categories: rigid, semi-rigid, and soft. The University of California Berkeley Laboratory (UCBL) orthosis is a static orthosis which has been extensively employed in the conservative management of flexible flatfoot. The more recently introduced modified foot orthosis (MFO) is more mobile in the midfoot region.4,5
Foot orthoses are able to reduce pain, discomfort, and fatigue by improving the foot posture distribution pattern, keeping the foot in a proper position, correcting bone spatial orientation, and altering activity patterns of the lower extremity muscles. 4 The proper combination of a shoe and an orthosis can enhance the sense of touch and proprioception, thus improving balance and reducing the probability of sprain or fall. These variations will also positively influence the normal posture of the lower extremities. 5
Foot plantar mechanoreceptors provide detailed information about contact pressure which is used for feedback mechanisms of the postural control system and balance. 6 Interventions such as a foot orthosis may optimize sensory information from plantar soles and may improve balance.7,8
An orthosis may be able to improve balance for those people with flatfeet.9,10 A study by Olmosted and Hertel 11 indicated that orthoses were effective in improving postural sway in subjects with cavus feet, yet they were ineffective for the participants with flatfoot. Corbin et al. 12 found that positioning was effective on balance outcomes. Orthoses in double limb stance position improved postural sway, but were not able to improve postural sway in single limb position.
There is not enough information concerning the effects of rigid foot orthoses on the postural stability and balance of people with flatfeet. The aims of the current investigation were (1) to provide scientific evidence of the effects of the new foot orthoses (MFO) on balance performance and (2) to compare the effects of orthosis flexibility on the postural sway of people with flatfeet.
Methods
This investigation was a quasi-experimental study, and a simple non-probability sampling method was employed. After obtaining ethical approval from the Clinical and Research Ethics Committee of the Iran University of Medical Science, 20 young patients with flatfoot (Table 1) were invited to participate in this study. They were referred to the Department of Orthotics and Prosthetics at the faculty of Rehabilitation Sciences, Iran University of Medical Science for the production of an insole due to flatfoot accompanied by pain inclusion criteria that included having an age of less than 23 years, having moderate or severe double flexible flatfoot, based on the foot posture index (FPI). 13 Participants with a score of 6–9 were considered to have moderate flatfoot, and those with a score of 10–12 were considered to have severe flatfoot. The participants had no history of fracture in the lower limbs and no systematic disease such as cerebral palsy, poliomyelitis, genu valgus, or varus that influenced the lower limbs. The flexible flatfoot condition was evaluated with the tip toe test. 14
The characteristics of the subjects studied (N = 20).

BMI: body mass index; FPI: foot posture index.
BMI = weight/height2.
Exclusion criteria were having any balance disorders, central nervous system (CNS) pathologies, or peripheral neuropathy, having used any insole in the last month, a previous history of foot surgery, any orthopedic lower limb disorder, using any drugs that influence balance, or being a professional athlete. Previous studies showed that physical activity may influence balance ability and thus must be considered in examining balance. 15
The participants were informed about the research procedures and were asked to sign both a consent form and an information sheet. Balance tests were carried out in one session with the Biodex Balance System (SD, Biodex, USA) at the Physiotherapy Research Center of the faculty of Rehabilitation Sciences, Iran University of Medical Science. The Biodex Balance System was able to provide two degrees of freedom around the anterior–posterior (A-P) and medial–lateral (M-L) axes and to measure medial–lateral stability index (MLSI) and anterior–posterior stability index (APSI). The Biodex Balance software provides an average sway score in two axes and permits to obtain the overall stability index (OSI).
A pair of sport shoes (2-cm heel and a shoelace) and two orthoses, namely, custom-made UCBL and MFO, were provided to each participant. Both orthoses were made on negative casts which were taken according to the suspension casting method introduced by Root. 16 The UCBL was modified based on the Colson and Berglund method. 17
The MFO had separate walls and a sole (Figure 1). Its M-L walls held the foot similar to the UCBL foot orthosis (Figure 2). Casts were taken in a semi-weight-bearing position in the maximum arch supination stabilization (MASS) position. 18 Orthoses were fabricated based on Saeedi’s modification method. 19
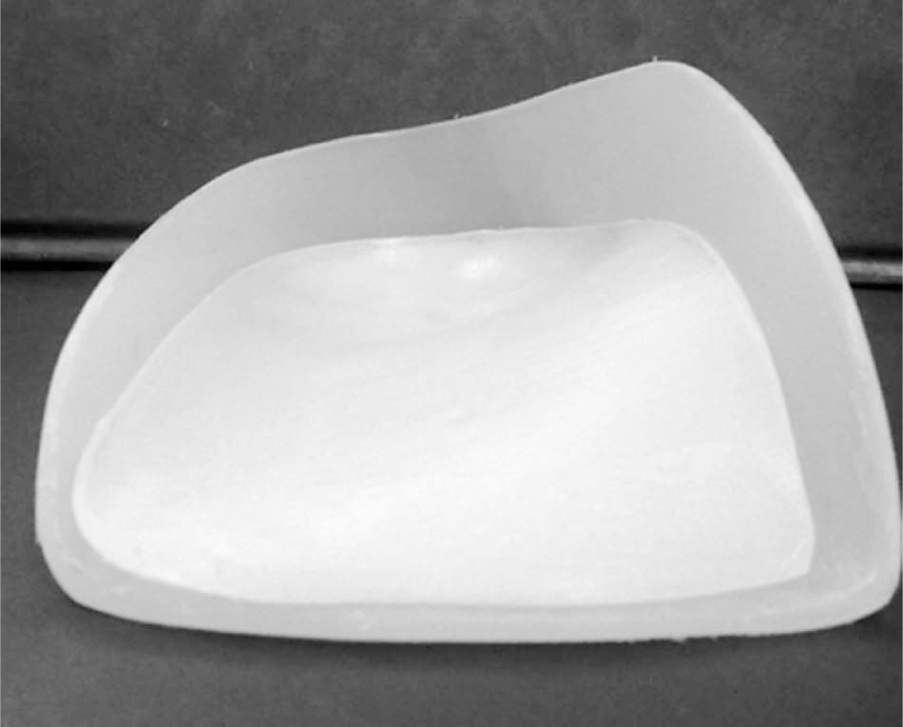
Modified foot orthosis.
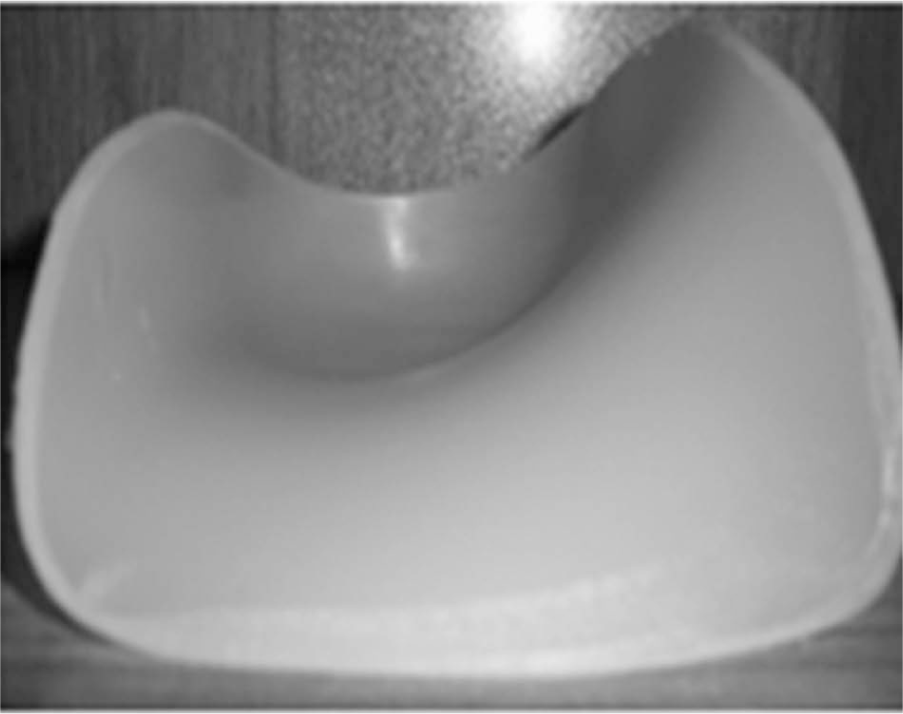
UCBL foot orthosis.
Three parameters—the total stability index, the MLSI, and the APSI—were tested in this study. Three testing conditions, namely, shoe-only, shoe plus UCBL, and shoe plus MFO, were considered for each participant. Each measurement was repeated three times and averaged.
The testing protocol consisted of a single 30-s test, which ran from the most stable level (level 12) to the least stable (level 1), with 2.5-s intervals for each testing condition 20 (Figure 3). The stability level was automatically decreased by the system. A 1-min resting time was considered between three trials of each testing condition, and a 5-min resting time was considered after each testing condition. The Biodex System was programmed to be automatically carried out for each participant.
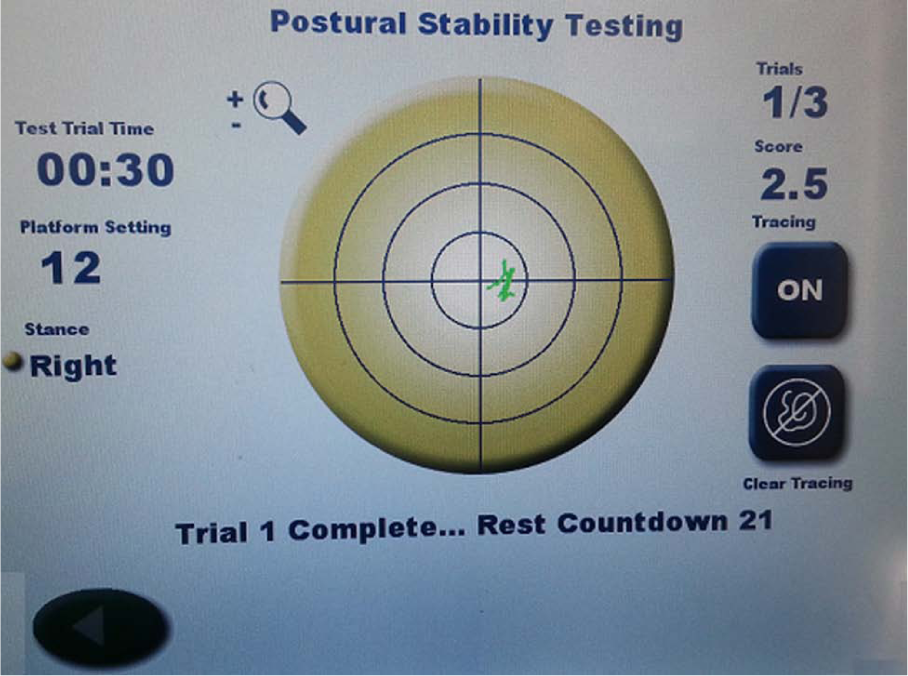
Biodex Balance System Report (SD, Biodex, USA).
The order of the testing conditions, namely, shoe, UCBL, and MFO, were randomly chosen. Randomization was carried out using opaque envelopes with concealed allocation. Participants were instructed to regulate their foot position on the plate so that while their posture was stable, the curser remained in the center of the display. This was carried out to establish each participant’s ideal foot positioning for testing. The display was then locked into the desired position. After locking, the direction of the forefoot and heel was recorded through angles drawn on the plate. This position was used for testing and was preserved for all testing conditions. Two warm-up tests were performed to familiarize participants with testing procedures before the main test was administered.
To perform the tests, participants were asked to stand on the dominant foot, while focusing to keep the cursor on the Biodex monitor in the center of the circle. They were also asked to bend the opposite leg so that the non-dominant foot did not come in contact with the ground, and their hands remained on their chests (Figure 4).

Participant test position.
Between each two tests, participants were asked to stand on his or her non-dominant foot for the 1-min resting period 21 while the dominant foot position was not changed. The recorded data were excluded whenever the non-dominant leg touched the ground or the participant used his or her hand to keep his or her balance. The participants were asked to walk 5 min before each of the three test conditions (shoe, UCBL, and MFO). All tests were carried out by the same examiner.
Statistical analysis
SPSS software ver.18.0 (SPSS Inc., PASW, USA) was used for statistical analyses. A significance level of 0.05 was considered for all testing conditions. The Kolmogorov–Smirnov (K-S) test was used to evaluate the normality of the data. Repeated-measures analysis of variance (ANOVA) was used to compare the results of the three testing conditions, and post hoc pair-wise comparisons were made using the Bonferroni adjustment for multiple comparisons.
Results
The results of the K-S test indicated that the measured data had a normal distribution (Table 2). The results of the repeated-measures ANOVA indicated that there was not a significant difference between three testing conditions (Table 3), but there was a significant difference between UCBL and MFO in total sway score. The mean of total sway score in UCBL was 13% less than MFO (p < 0.05) (Figure 5). The average sway score of participants using the MFO was increased by 10% and 12% compared to UCBL in A-P and M-L direction, respectively, but both of these differences were not significant.
Descriptive statistics for the balance measures and the K-S test.
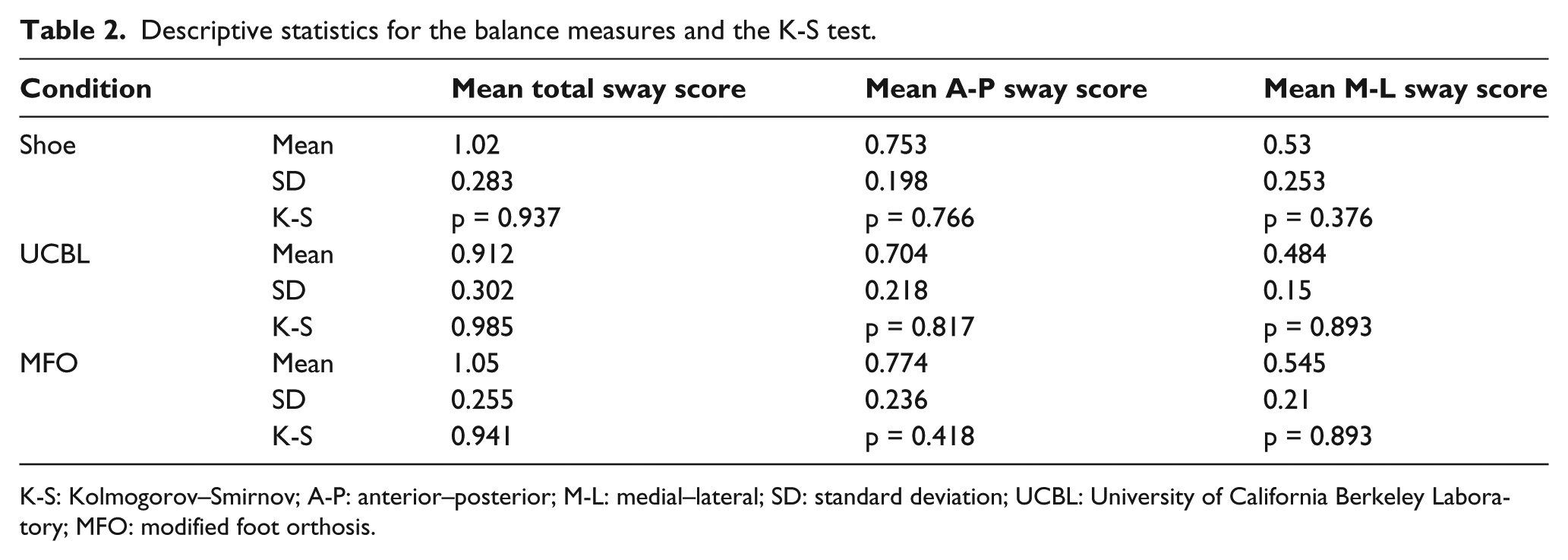
K-S: Kolmogorov–Smirnov; A-P: anterior–posterior; M-L: medial–lateral; SD: standard deviation; UCBL: University of California Berkeley Laboratory; MFO: modified foot orthosis.
Mean ± SD sway in three test positions and results of repeated-measures ANOVA test.
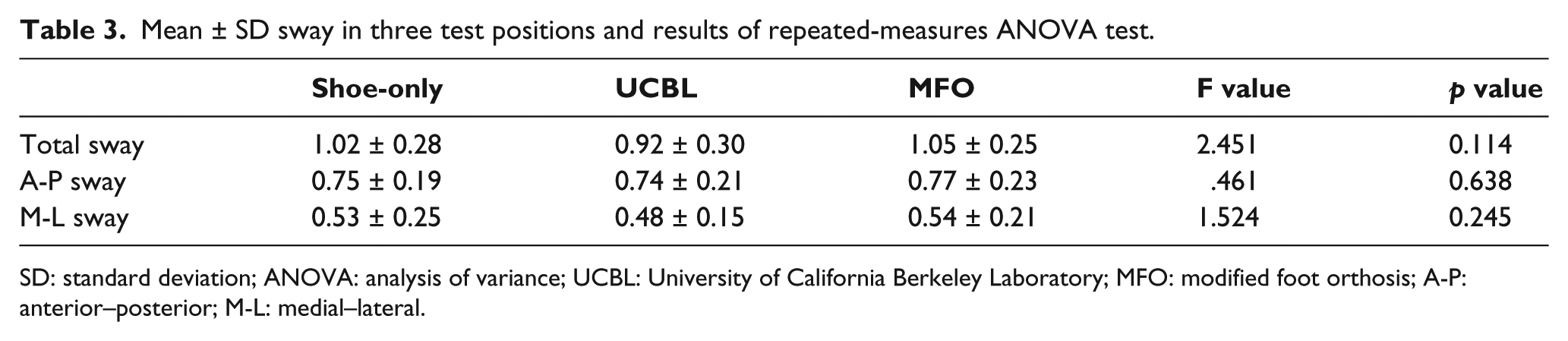
SD: standard deviation; ANOVA: analysis of variance; UCBL: University of California Berkeley Laboratory; MFO: modified foot orthosis; A-P: anterior–posterior; M-L: medial–lateral.
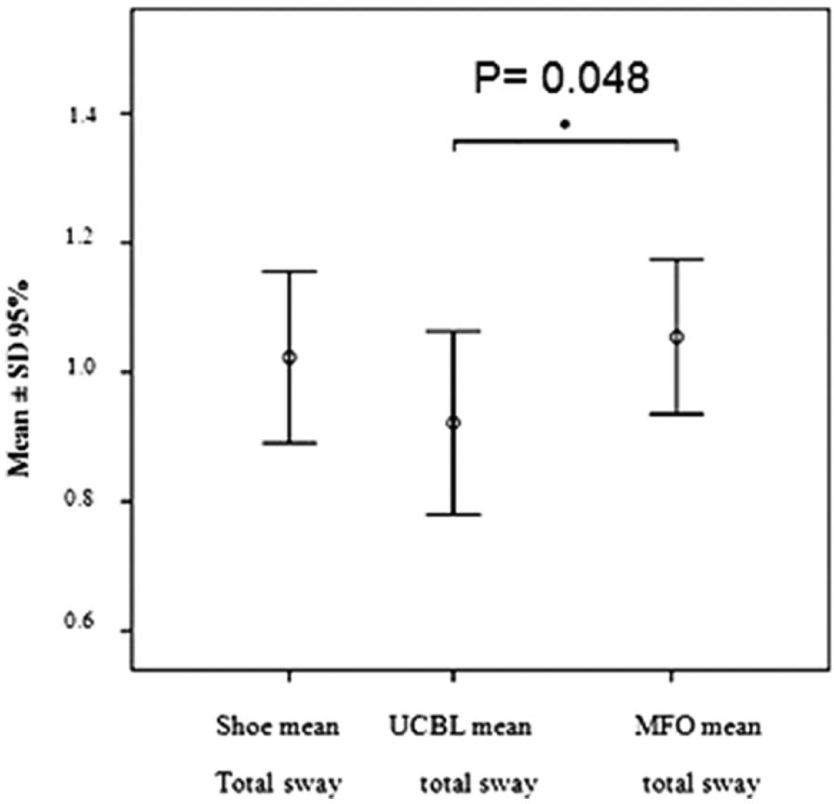
Comparison of the effect of the shoe-only, UCBL, and MFO device conditions in total sways. *p < 0.5.
Discussion
Results of the current study revealed that there was no significant difference between the mean sway in standing with shoe only and standing with combination of shoe and orthoses. This finding was consistent with the findings of Precy and Rome.5,9 They did not observe any significant difference in the postural sway for testing conditions, namely, barefoot and shoe plus orthoses.5,9 Hetrel et al. 22 and Gross et al., 23 however, observed increased postural stability and improved balance immediately after wearing the foot orthoses.
Sway in the M-L direction was generally less than the total and A-P direction. These findings were also consistent with the Cote et al. 3 study. M-L and A-P sway were the least in UCBL foot orthosis; nevertheless, they were not significantly less than MFO. The UCBL sway was, however, significantly lower than MFO in the total direction.
The center of body mass tends to internally shift in those people with flatfoot due to the fall of the medial longitudinal arch. Orthoses are prescribed to reduce pronation of the foot and to return it to its natural posture, which will shift the center of mass of the body to its normal position. This may cause alterations in the balance strategy adapted by each participant. This finding was inconsistent with the result of Landsman 24 , but was consistent with that of Orteza et al., Akbari et al., and Gross et al.,23,25,26 The decrease in the sway caused by some orthoses might be related to their structures.
A comparison of the sway in the M-L direction indicated that the UCBL orthosis had the least degree of sway in this direction. This might be due to its medial and lateral walls that firmly hold the heel and foot, thus reducing postural sway. Although the UCBL was able to reduce sway more than the MFO and shoe-only condition, this reduction was not statistically significant in A-P and M-L directions. In total direction, the sway of the UCBL foot orthosis was significantly less than that of the MFO, so participants may have tried harder to preserve their balance on the moving plate, while for the MFO, the flexibility of the MFO insole and its walls were not able to augment stability to control sway.
In this study, however, no significant difference was observed between the sway of standing with shoe only and standing with shoe plus orthosis. The orthosis was not able to reduce sway instantly compared to the shoe only. It seems, therefore, that a supportive pair of shoes (laced, sport show type etc) may reduce sway and improve balance, and an accommodation period of a few weeks may reduce the aforementioned effect of the shoes. 27
Conclusion
A comparison of sway results in the tested orthoses indicated that the UCBL orthosis significantly reduced the mean sway in the total stability index of people with flexible flatfoot, and it may improve balance in total among those with flatfeet. It seems that creating mobility in the midfoot area of the foot orthosis may cause a balance disturbance in patients with flatfoot. In this study, only the immediate effects of an orthosis on balance were investigated; the long-term effects of orthoses were not investigated. It is recommended that other balance parameters such as sway of the center of pressure and the long-term effect of orthoses also be investigated.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.