
Abstract
Background:
Despite the common use of braces to prevent curve progression in idiopathic scoliosis, their functional effects on respiratory mechanics have not been widely studied.
Objective:
The objective was to determine the effects of bracing on pulmonary function in idiopathic scoliosis.
Methods:
A total of 27 adolescents with a mean age of 14.5 ± 1.5 years and idiopathic scoliosis were included in the study. Pulmonary function evaluation included vital capacity, forced expiratory volume, forced vital capacity, maximum ventilator volume, peak expiratory flow, and respiratory muscle strengths, measured with a spirometer, and patient-reported degree of dyspnea. The tests were performed once prior to bracing and at 1 month after bracing (while the patients wore the brace).
Results:
Compared with the unbraced condition, vital capacity, forced expiratory volume, forced vital capacity, maximum ventilator volume, and peak expiratory flow values decreased and dyspnea increased in the braced condition. Respiratory muscle strength was under the norm in both unbraced and braced conditions, while no significant difference was found for these parameters between the two conditions.
Conclusion:
The spinal brace for idiopathic scoliosis tended to reduce pulmonary functions and increase dyspnea symptoms (when wearing a brace) in this study. Special attention should be paid in-brace effects on pulmonary functions in idiopathic scoliosis.
Clinical relevance
Bracing seems to mimic restrictive pulmonary disease, although there is no actual disease when the brace is removed. This study suggests that bracing may result in a deterioration of pulmonary function when adolescents with idiopathic scoliosis are wearing a brace.
Background
Bracing is the gold standard of conservative treatment for moderate or severe idiopathic scoliosis (IS) and is used to prevent curve progression during the skeletal growth period. 1 Thoracolumbosacral orthosis (TLSO) are commonly used, and they have a rigid construction and tend to reduce the mobility of the trunk. 2 Despite the existence of several brace designs, the brace mechanism includes three-dimensional external corrective forces acting against the curve. 3 Therefore, the effects of bracing on thorax mechanics, chest mobility, and pulmonary functions are considered inevitable. 4
Bracing has important positive effects on scoliosis treatment in the long term, such as reducing curve magnitude and rib hump, and improving cosmetic appearance and trunk symmetry.5,6 However, wearing a brace for many years can be a traumatic experience for adolescents. A brace may cause pressure scars, pain, emotional and social problems, and a disturbed self-image and body image, thereby affecting the quality of life of an individual with IS. 7
Earlier long-term studies had reported a brace-related increased risk of cardiorespiratory failure. 8 Other studies have shown that the effects of a TLSO brace caused a reduction in volume and pulmonary compliance in patients with IS.9,10 But recent studies have found either no bracing effect on adolescent pulmonary function over a 2-year period 11 or a positive effect of curve correction regarding increase in thoracic volume and pulmonary capacity in patients with IS with severe restrictive pulmonary function. 12
The assessment of pulmonary function is an important complement for establishing the diagnosis of various pulmonary problems as a marker of morbidity, mortality, and general health. 13 In scoliosis, reductions in vital capacity (VC), pulmonary restrictions, and altered chest wall mechanics related to the angle of spinal curvature may occur. 14 Spirometric measurement is a simple, rapid, and non-invasive method that provides quantitative knowledge of respiratory functions. 15 It is also helpful in detecting mechanical dysfunctions of the respiratory system, defining the nature of the dysfunction as obstructive or restrictive, and evaluating the effect of therapeutic intervention, such as bracing on the respiratory system in adolescents and adults. 15 Moreover, the knowledge of how pulmonary functions are affected by the brace may provide the chance to create novel clinical solutions when designing a corrective brace for scoliosis.
Although many studies show that bracing is effective in preventing curve progression, its effects on pulmonary function remain controversial. In view of these contradictory studies, the aim of this research was to determine the effects of bracing on pulmonary function in adolescents with IS (while wearing a brace).
Methods
Participants
A total of 27 female adolescent patients with IS undergoing brace treatment were included in the study. The inclusion criteria were having a primary thoracic curve, moderate scoliosis (a Cobb angle of 20°–45°for the primary curve), and a bracing indication. Exclusion criteria involved having undergone spine surgery, being a smoker, being a professional athlete, and having a respiratory disease. All patients used a custom-made TLSO brace for their scoliotic curve (Figure 1). 16
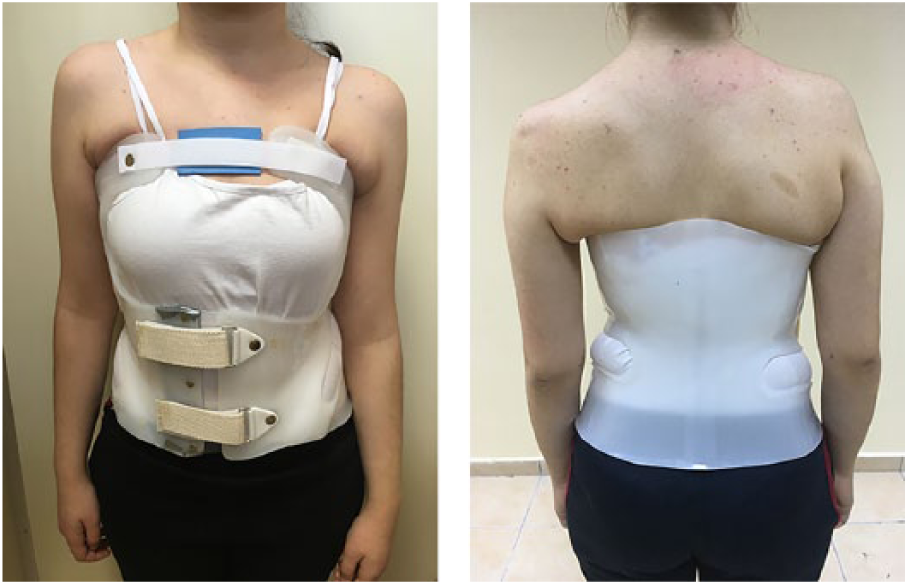
The thoracolumbosacral orthosis (TLSO).
Outcome measures
The following demographic characteristics were recorded for each patient: age, gender, height, weight, body mass index, and brace-wearing time per day. A total of 20 patients had a right thoracic left lumbar curve pattern, whereas seven patients had a high right thoracolumbar curve pattern. The curve magnitude was assessed by antero-posterior spine radiography with the Cobb angle. 17 Trunk deformity was measured by the angle of trunk rotation (ATR) of the hump on the main curve with Bunnell’s scoliometer in the forward bending test. 18
A 0–10 Modified Borg Scale was used to evaluate the degree of dyspnea. 19 The scale consisted of a vertical scale labeled 0–10, with corresponding verbal expressions of progressively increasing perceived sensations of breathlessness (Figure 2).
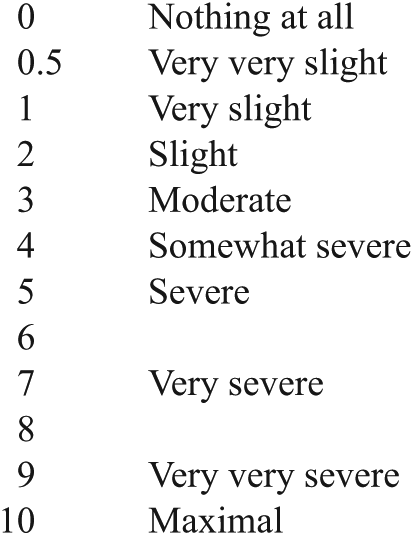
Modified Borg scale.
Pulmonary function
Slow VC (the maximum volume of air that can be exhaled after a maximum inspiration), forced expiratory volume (FEV1) in 1 s (the amount of air expired in 1 s during a rapid and maximal expiration from full inspiration), forced vital capacity (FVC) (the maximum volume of air expelled as rapidly and completely as possible by a maximum effort after a maximum inspiration), maximum ventilator volume (MVV) per minute, and peak expiratory flow (PEF) were measured with a desktop spirometer (a pulmonary function test instrument; Cosmed Pony FX). 20 The ratio of FEV1/FVC and forced expiratory flow between 25% and 75% of VC (FEF25–75) expired and were used to evaluate airway obstruction.
Respiratory muscle strength was assessed as maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) with the same device. MIP was measured at residual volume after a complete exhalation, and MEP was measured at total pulmonary capacity after a maximal inspiration. The patient was instructed to hold the manovacuometer, tighten the mouthpiece firmly against the lips, preventing air leakage, and make a maximum inspiration from the residual volume to measure MIP and a maximum expiration from total pulmonary capacity to determine MEP. 21
All pulmonary function tests were performed according to specifications of the American Thoracic Society for pulmonary function testing by the first author (G.Y.). 21 Sufficient time was allowed for patients to rest between pulmonary function tests as well as between individual maneuvers to minimize fatigue. All the equipment was calibrated according to standard recommendations. Patients were assessed in the sitting position. The subjects were given an opportunity to perform a few practice efforts at baseline. Later, each subject was required to perform a minimum of three efforts reproducible for each measurement under the supervision and direction of a physiotherapist, with resting intervals of 30–60 s between measurements. The highest value considered was used in the analysis for each test.
Outcome measures were collected before treatment (unbraced) and 1 month after bracing for the in-brace condition (braced). The order of testing (unbraced or in-brace condition) was randomized. The brace was worn at least 1 h before in-brace evaluation. Total rest period between unbraced and in-brace conditions was 4–6 h. Hacettepe University Research Ethics Board approved the study. All patients and their parents were educated about the study and signed informed consent paperwork.
Brace design
A custom-made, rigid TLSO brace was fabricated and fitted according to patient’s individual requirements by an experienced orthotic technician (Figure 1). The manufacturing process included plaster cast measurement, positive model forming, and fabricating the polyethylene molded final version of the brace. The proper biomechanical principles for orthotic correction was applied regarding corrective forces against spinal column lateral deviation and axial rotation, while protecting the physiological lumbar lordosis and allowing thoracic expansion and free movement ability to the trunk and four extremities. While maintaining original body shape, the brace also provided symmetrical posture by achieving this a three-dimensional action of correction.
Analysis
Statistical analysis was performed using the Statistical Software Package (SPSS), version 15.0 (SPSS Inc., Chicago, IL, USA). Normality of distribution of the data was assessed using the Kolmogorov-Smirnov test. Differences between mean values of the unbraced and braced conditions were tested for significance using the Wilcoxon signed-rank test. Data were expressed as means ± standard deviations. The alpha level for determining statistical significance was set at 0.05.
Results
The cohort comprised 27 females with IS. The mean age was 14.5 ± 1.5 years (range, 12–16 years). The mean Cobb angles were 28.6° ± 7.0° and 24.3° ± 6.5° for the thoracic and lumbar regions, respectively. The mean ATR was 7.5° ± 3.1° and 5.2° ± 1.4° for the thoracic and lumbar regions, respectively. Table 1 shows patient characteristics.
Patient characteristics.
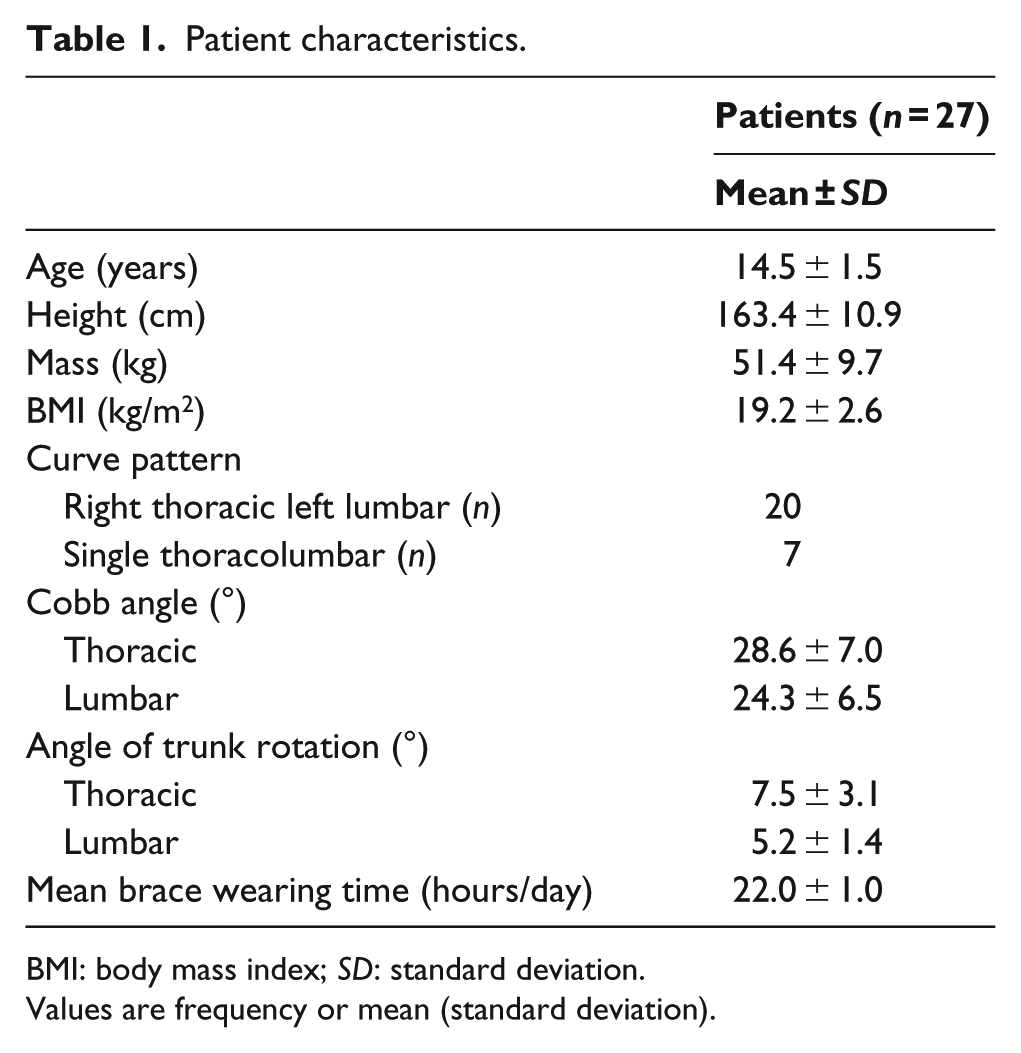
BMI: body mass index; SD: standard deviation.
Values are frequency or mean (standard deviation).
Table 2 shows a comparison of dyspnea and pulmonary functions of patients in unbraced versus braced conditions. Spirometric results showed a difference in pulmonary function between braced and unbraced conditions. Significant reductions were observed for the braced condition for VC, FEV1, FVC, MVV, and PEF actual and % predicted values when compared with the unbraced condition. There was no difference in the ratio of FEV1/FVC between unbraced and braced conditions. The FEF25–75 value was decreased for the braced condition. In addition, patients reported greater dyspnea symptoms in daily life for the braced condition. There was no difference in the values of MIP and MEP between braced and unbraced conditions.
Comparison of pulmonary functions of patients with brace versus without brace conditions.
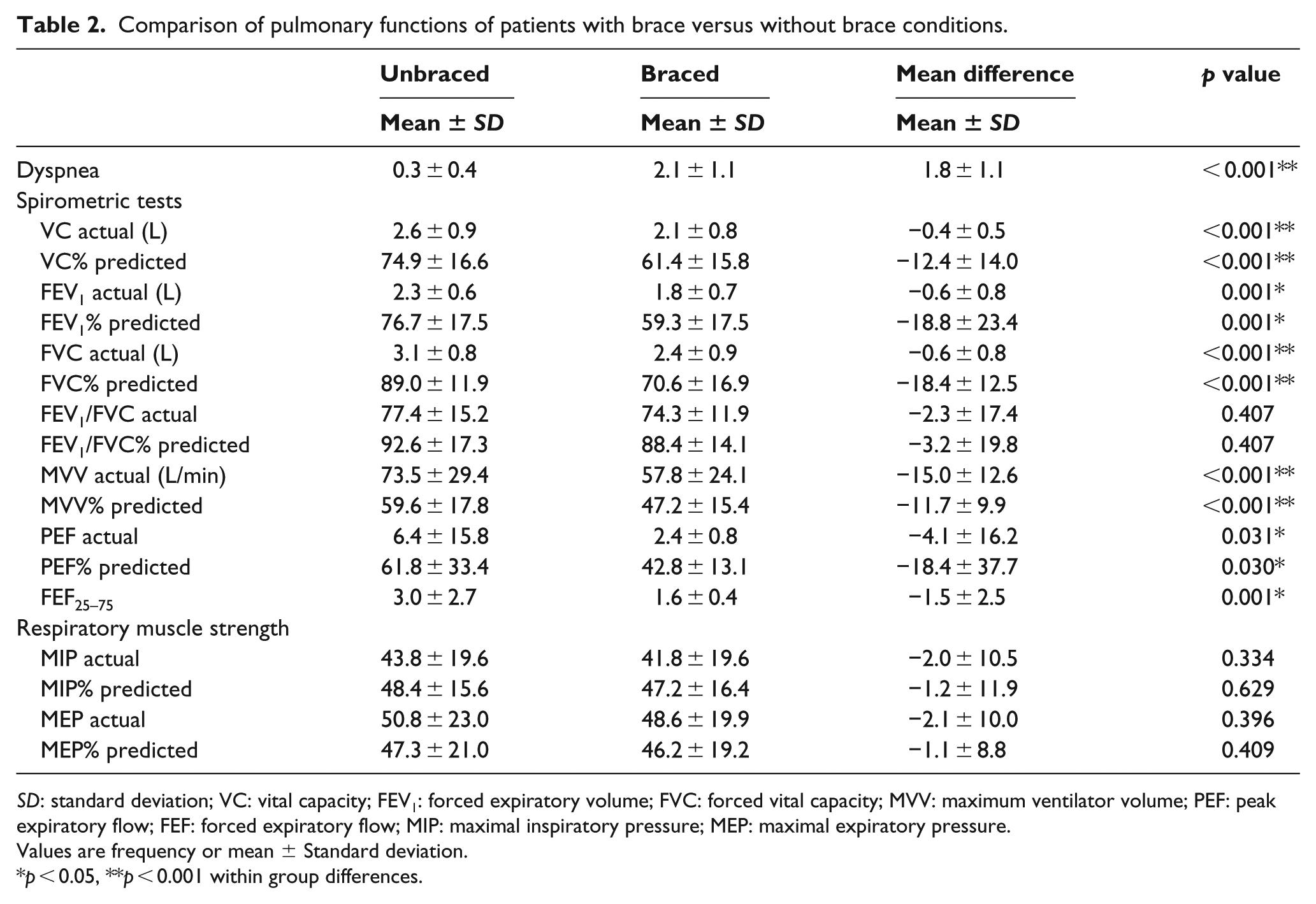
SD: standard deviation; VC: vital capacity; FEV1: forced expiratory volume; FVC: forced vital capacity; MVV: maximum ventilator volume; PEF: peak expiratory flow; FEF: forced expiratory flow; MIP: maximal inspiratory pressure; MEP: maximal expiratory pressure.
Values are frequency or mean ± Standard deviation.
p < 0.05, **p < 0.001 within group differences.
Discussion
In this study, the in-brace condition was found to alter pulmonary functions and tended to decrease FEV1, VC, FVC, MVV, and PEF values, while increasing patient-reported dyspnea in daily activities. The results also show that respiratory muscle strength of the patients was under the norm in both the unbraced and braced conditions, while bracing did not affect the pressure-generating capacity of the inspiratory and expiratory muscles. Patients with IS seem to have pulmonary function limitations from the brace (while wearing the brace).
Pulmonary function in patients with mild to moderate scoliosis has generally been reported as normal. As the curve magnitudes increase, pulmonary volume reduces and in severe cases, airway obstruction occurs. 22 But the effects of bracing on respiratory mechanics may vary according to curve magnitude, brace design, restrictive effects on rib cage and trunk mobility, applied corrective forces, how long the brace is worn, and so on.4,8 In this study, the unbraced and braced condition comparisons have shown that there was a mild decrease (defined by the American Thoracic Society) 23 in FEV1 (with mean change 18.8%), VC (with mean change 12.4%), FVC (with mean change 18.4%), MVV (with mean change 11.7%), and PEF (with mean change 18.4%) values of spirometric measurements while wearing a brace when compared with the unbraced condition. These alterations may be due to the correcting forces exerted by the brace and its possible limiting effect on the expansion of the rib cage during inspiration. Kennedy et al. 8 reported a significant reduction in VC (14%), functional residual capacity (22%), and total pulmonary capacity (12%) with the application of Boston or Milwaukee braces in 13 patients with IS. They associated these alterations with decreased lower rib cage and abdominal movement and the increased effect on diaphragmatic workload. Similarly, Korovessis et al. 11 and Katsaris et al. 9 found a decrease in pulmonary function, including VC, FVC, and functional residual capacity as an immediate effect of the Boston brace. But Korovessis et al. 11 also reported that 2 years of bracing for mild IS does not alter pulmonary function. Yu et al. 10 also revealed that wearing a brace may aggravate pulmonary function by increasing the stiffness of the thoracic cage. However, Pehrsson et al. 24 indicated improvement in pulmonary function regarding increased VC (12.3% improvement) and FEV1 (7.1% improvement) in brace-treated patients at the 25-year follow-up.
In terms of airflow variables, in this study the ratio of FEV1/FVC did not change with bracing, whereas FEF25–75 decreased in the braced condition. The FEV1/FVC ratio is considered to define medium airway patency and values above 75% are generally accepted as normal. 25 Therefore, we can say that the mean FEV1/FVC ratios of our patients are relatively within the normal range for both the unbraced and braced conditions. But reduced FEV1 and FVC, together with a normal FEV1/FVC ratio in the braced condition, shows that bracing seems to cause extrinsic restrictive pulmonary disorders (although there is no actual disease). The midflow rate, FEF25–75, measured during spirometric testing, is believed to represent reduced airway airflow. 26 We could say that bracing causes minor airway flow disturbances or air trapping in the small airway (while wearing the brace). We also know that our patients reported greater dyspnea in daily activities while they wore a brace. Our brace design has a space and elastic strap on the chest in front of the brace that aim to provide proper thorax expansion during respiration. But these results may show that the ability of the thorax to expand may be limited in some cases with the brace compression effect, despite the elastic strap on the chest. This may make breathing significantly harder, increasing the workload of the respiratory muscles and causing dyspnea.
Because of the convex and concave shapes of the scoliotic spine, antero-posterior and transverse diameters in each hemithorax differ significantly, and therefore, asymmetrical inflation of the lungs may occur. 27 Even when the lungs themselves are completely healthy in IS, the work involved in breathing has been reported to increase. 22 Respiratory muscles, the diaphragm, internal and external intercostal muscles, and several muscles of the abdominal wall have a functional role in respiration. 22 Bracing may limit their functions by changing the optimal length-tension relationship of the muscles and causing overstretching or the inability to stretch due to changes created by the brace in the intercostal spaces. 8 In healthy adolescents, the mean MIP was reported as 74.6 and 103.5 cm H2O, and the mean MEP was reported as 86.2 and 120.1 cm H2O for girls and boys, respectively. 28 Previously, inspiratory and respiratory muscle strengths were shown to be under the norm in IS, with averages of 76.6 and 79.5 for MIP and MEP, respectively. 14 In this study, MIP and MEP scores of patients with IS (with averages of 43.8 and 50.8 cm H2O) were both under the norm and less than those found in other studies on IS. And there was no difference between the two conditions. This may show respiratory muscle weakness in our patients, who have moderate scoliosis.
There are some limitations of this research. Our study was designed to assess only the immediate effects of bracing on pulmonary function. Further studies are needed with long-term intervention of bracing in larger groups of patients with IS. Our patients had a primary thoracic curve pattern; therefore, the brace covered the thoracic lumbar and sacral regions for the primary correction effect in the thoracic region. Moreover, this study included patients with moderate scoliosis. The results may vary if the curve magnitude is more severe. Our results cannot be generalized for other types of spinal braces used for scoliosis treatment.
Conclusion
Spinal bracing is likely to limit pulmonary functions, including reduced FEV1, VC, FVC, MVV, and PEF values and to increase dyspnea in daily activities (while patients wear the brace). Bracing seems to mimic restrictive pulmonary disease, although there is no actual disease when the brace is removed. The results also show that respiratory muscle strength of patients with moderate IS was under the norm. In conclusion, this study suggests that bracing may result in a deterioration of pulmonary function when adolescents with IS are wearing a brace.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This article has been supported by the Scientific Research Coordination Unit of the Hacettepe University [grant number. THD-2015-6090].