
Abstract
Background:
Sufficient cardiorespiratory fitness has been regarded a prerequisite for prosthetic walking. In order to improve cardiorespiratory fitness, adequate strain ought to be placed on the system during training.
Objectives:
To determine cardiorespiratory fitness at the start and end of inpatient rehabilitation after lower limb amputation and determine the physical strain experienced during conventional prosthetic rehabilitation.
Study design:
Multicenter prospective cohort study.
Methods:
Cardiorespiratory fitness was assessed using a peak one-legged cycle exercise test. Physical strain was assessed during a minimum of three full rehabilitation days using heart rate recordings. Physical strain was expressed in the time per day that heart rate exceeded 40% of heart rate reserve.
Results:
At the start of rehabilitation, peak aerobic capacity was on average 16.9 (SD, 6.5) mL/kg/min (n = 33). Overall, peak aerobic capacity did not improve over the course of rehabilitation (n = 23, p = 0.464). Fifty percent of the patients experienced a physical strain level that satisfies minimum criteria for maintaining cardiorespiratory fitness (>40% heart rate reserve for 30 min/day).
Conclusion:
Cardiorespiratory fitness was low and did not increase during conventional prosthetic rehabilitation. On average, the physical strain during rehabilitation was insufficient to elicit potential improvements in aerobic capacity. Results stress the need for dedicated physical training modules at the individual level.
Clinical relevance
This study shows that clinicians ought to be aware of the relatively low cardiorespiratory fitness of people who have undergone lower limb amputation and that improvements during rehabilitation are not always obtained. Results stress the need for physical training modules in which intensity is imposed at the individual level.
Background
Undergoing a lower limb amputation is a major life event that drastically affects daily activity and functioning and hence restricts active participation in the community. Not surprisingly, lower limb amputation has been associated with a decrease in quality of life. 1 Prosthetic rehabilitation following lower limb amputation is aimed at improving quality of life by enabling patients to regain and improve their functional ability using a prosthesis. Optimizing cardiorespiratory fitness is one of the underlying goals pursued when improving functional ability during prosthetic rehabilitation. 2
A vast majority (87%–94%) of the amputations performed in developed countries are a result of vascular deficiency.
3
These patients often have comorbidities that negatively affect cardiorespiratory fitness and lead an inactive lifestyle both prior to and after surgery. Moreover, the advanced age at which lower limb amputation is primarily performed (75% > 60 years)
4
and the age-related natural decline in aerobic capacity support the notion that aerobic capacity is low in this patient population. However, few scientific studies have quantified this expected reduction in aerobic capacity2,5 and prospective observational studies are lacking. A cross-sectional cohort study by Chin et al.
6
showed that at the time of prosthetic rehabilitation, elderly people have a reduced aerobic capacity when expressed as a proportion of the age-predicted aerobic capacity
Adequate cardiorespiratory fitness may have great implication for those who have undergone amputation since aerobic load of walking is markedly increased. In previous studies, a relationship was observed between a reduced aerobic capacity and the ability to walk with a prosthesis.6,10,11
To improve cardiorespiratory fitness, sufficient strain on the cardiorespiratory system through physical activities is required. The amount of physical strain experienced by a patient is determined by intensity, duration, and frequency of the physical activities performed. To improve or maintain cardiorespiratory fitness, the American College of Sports Medicine recommends a minimum of 30 min of moderate-intensity (>40% heart rate reserve) exercise for 5 days per week. 12 Koopman et al. 13 showed that on average the physical strain of a heterogeneous group of patients (including nine patients with an amputation) reached the minimal required activity volume during rehabilitation, albeit the variation in strain level was very large among patients. It remains questionable, however, whether this resulted in improvements in cardiorespiratory fitness over the course of prosthetic rehabilitation.
The current multicenter prospective cohort study aims to determine cardiorespiratory fitness in people after lower limb amputation at both the start and end of rehabilitation and to determine the physical strain experienced during conventional rehabilitation. Information about the physical strain experienced during rehabilitation might contribute to our understanding of potential changes in aerobic capacity, or lack thereof, at the end of the program, which could have important implications for future development of effective rehabilitation programs.
Methods
Study design and patient inclusion
This study was designed as a prospective cohort study, with assessments at the start (T0) and end (T1) of the regular rehabilitation program. All patients entering one of the two participating rehabilitation centers (Heliomare, Rehabilitation, Wijk aan Zee, the Netherlands or UMCG, Center of Rehabilitation, Beatrixoord, Haren, the Netherlands) for prosthetic inpatient rehabilitation over a time course of 11 and 8 months, respectively, were eligible for participation. Exclusion criteria for participation in the study were an absolute contraindication for exercise testing, 14 severe comorbidities (e.g. non-healing large wounds, movement limitation in the contralateral limb, and severe respiratory limitations), a body mass index (BMI) above 40, and/or a bi-lateral amputation of the lower limb. This study was approved by the Medical Ethical Review Board of the VU University Medical Center in Amsterdam (NL43218.029.13) and all participants provided written informed consent preceding inclusion in the study.
Data collection
Graded exercise test
All patients underwent graded exercise testing using the previously validated graded discontinuous one-legged cycle exercise test at the start of rehabilitation to determine the peak aerobic capacity. A more elaborate description of this test protocol, and its validity, can be found in a previous publication.
15
Prior to the exercise test, resting electrocardiogram (ECG), blood pressure (by manual auscultation), and BMI (body weight/height
2
, note: body weight was determined without prosthesis and not controlling for the amputated leg) were recorded. Throughout the exercise test, oxygen consumption
Physical strain during rehabilitation
In general, patients were engaged in the inpatient rehabilitation program for 5 days a week from about 8 am to 5 pm, during 2–5 months. The rehabilitation program followed general Dutch guidelines for rehabilitation after lower limb amputation. The program contained different activities spread over the entire day involving activities of daily living (ADL), specific therapeutic sessions, general training activities, and resting periods. The exact type, order, and timing of these activities varied between patients depending on their possibilities and individual rehabilitation goals.
Information about the physical strain during rehabilitation was gathered using heart rate recordings (Polar Electro Oy or Polar team pack, Kempele, Finland). During the week following the graded exercise test, patients were instructed to wear a heart rate monitor for 3–5 days between 8 am and 5 pm, while undergoing regular rehabilitation (weekends were excluded). Patients repeated this assessment at the end of rehabilitation, that is, within 2 weeks of the proposed discharge date. During the days of heart rate monitoring, patients received care as usual.
Data analysis
Data processing
Graded exercise test. Oxygen consumption was attenuated using a 5-breath moving averaged filter. The peak aerobic capacity (
Physical strain during rehabilitation. The resting heart rate was determined as the lowest value recorded on any day during the experiments after applying a moving average filter of 60 s. Peak heart rate was obtained from the graded exercise test. However, for six patients, the heart rate recorded during rehabilitation was higher than that obtained during the exercise test (differences ranging between 5 and 32 beats/min). For these patients, the higher heart rate during the monitor week was used as the HRpeak. Activity intensity during rehabilitation was expressed in percentage heart rate reserve (%HRR) using the formula reported by Karvonen et al. 19 HRR was calculated as the difference between maximum heart rate and the heart rate at rest.
Physical strain was expressed as the amount of time a patient spent above 40%HRR during the time of heart rate recording. First, heart rate data as a function of time was smoothed with a 10-min moving average. This prevented counting of very small episodes of increased heart rate and complies with the recommendations that effective exercise episodes should last at least 10 min. 12 Subsequently, the total time during the measurement session spent over 40% HRR was summed. As the time of measurement varied between patients, because the heart rate monitor was not worn or transmitting the entire day for all patients, we expressed data as the percentage of wearing time. Multiplying this percentage by the nominal 9 h of the rehabilitation day, we estimated the total minutes of time spent above 40% HRR on each day. As secondary outcomes, we also calculated the amount of time per day spent at an intensity level above 70% HRR; moreover, physical strain is presented as a frequency distribution per 10% of HRR.
Statistical analysis
Data were tested for normality using the Kolmogorov–Smirnov test. All parameters were normally distributed. Statistical significance of differences between measurements performed at the start and end of rehabilitation was determined using paired sample t-tests. Correlations between the percentage increase in aerobic capacity
Results
Patients
During the time course of this study, 67 patients were admitted for prosthetic rehabilitation. In total, 34 patients were considered eligible to participate in the study. As can be seen in Figure 1, the major reason for being ineligible for participation was severe comorbidity. Of the 34 patients who were eligible for participation, one was unable to successfully perform the exercise test due to cognitive limitations. Of the remaining 33 patients (average age 57.9 (SD, 14.2) years and BMI 26.7 (SD, 5.3)) that performed the exercise test at the start of rehabilitation (T0), 29 had undergone amputation due to vascular deficiency, 2 due to trauma, and 2 due to cancer. Twenty-one patients underwent amputation at the transtibial level, 8 at transfemoral level, and 4 at other levels (1 knee disarticulation, 1 hip disarticulation, and 2 rotationplasty). At the time of the first exercise test, time since amputation was on average 89 days but varied widely (range, 13–774). The large variation in days between amputation and initial test could be explained by four patients who were re-admitted for prosthetic rehabilitation (n = 1, vascular), had a long hospitalization period (n = 1, cancer), or were admitted to a nursing home prior to prosthetic rehabilitation (n = 2, vascular). Average time spent in rehabilitation was 118 days (SD, 51). Of the 33 patients who participated, 12 were using Beta-blocking medication. For several reasons, data were only partially collected in a number of patients (Figure 1). No differences in patient characteristics were found between the group that performed all measurements and those that participated in only part of the study. Characteristics of the patients included in the different analyses are reported in Tables 1 and 2.
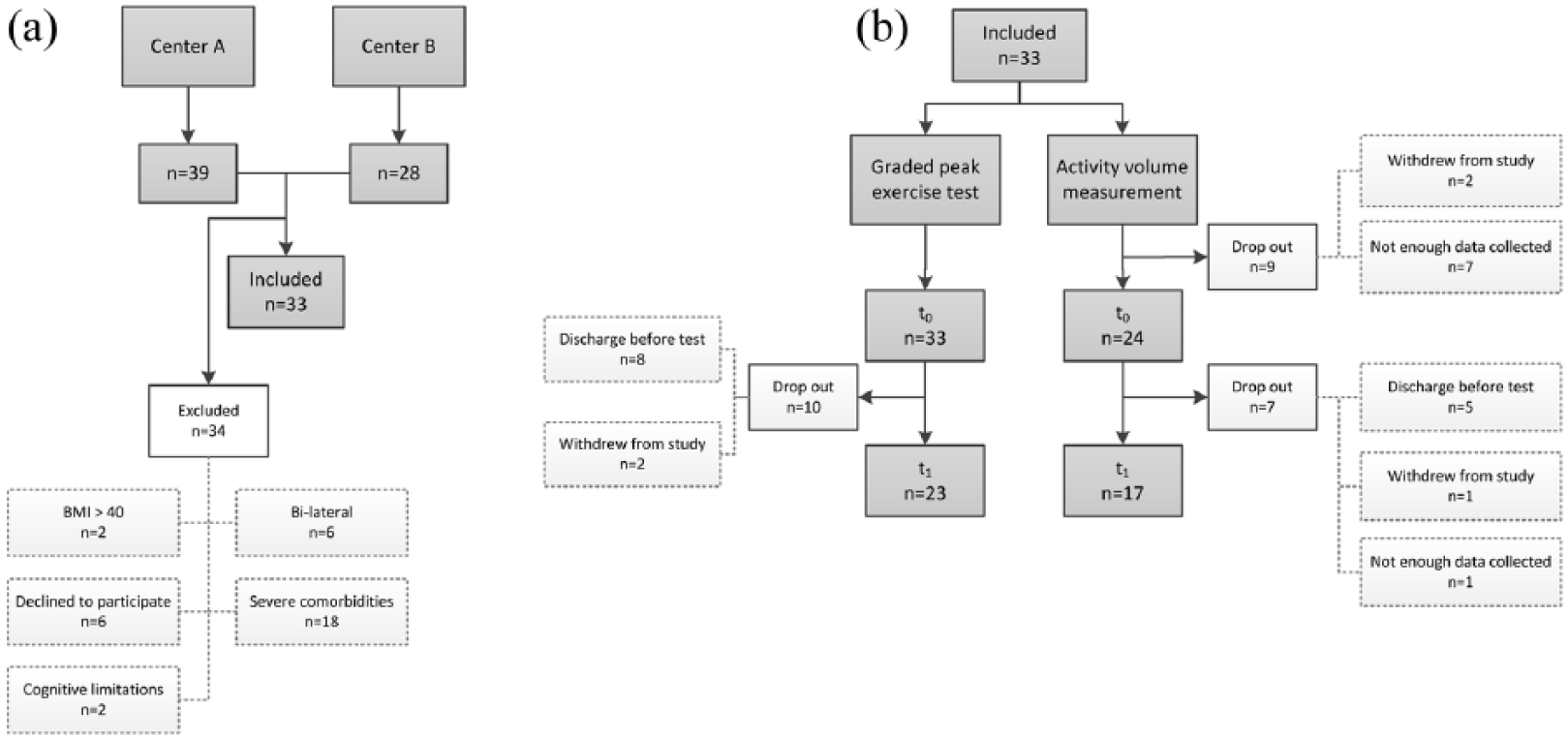
Flow diagram of patient inclusion. (a) The total number of patients admitted for prosthetic rehabilitation in both rehabilitation centers. Inclusion period was 11 months in Center A and 8 months in Center B. The number of patients excluded from this study and the associated reasons are presented. If patients decided not to participate, they were not obliged to give a reason this is indicated withdrew from study. (b) The number of patients who took part in the different measurements within this study.
Graded exercise test; mean subject characteristics (SD or range).
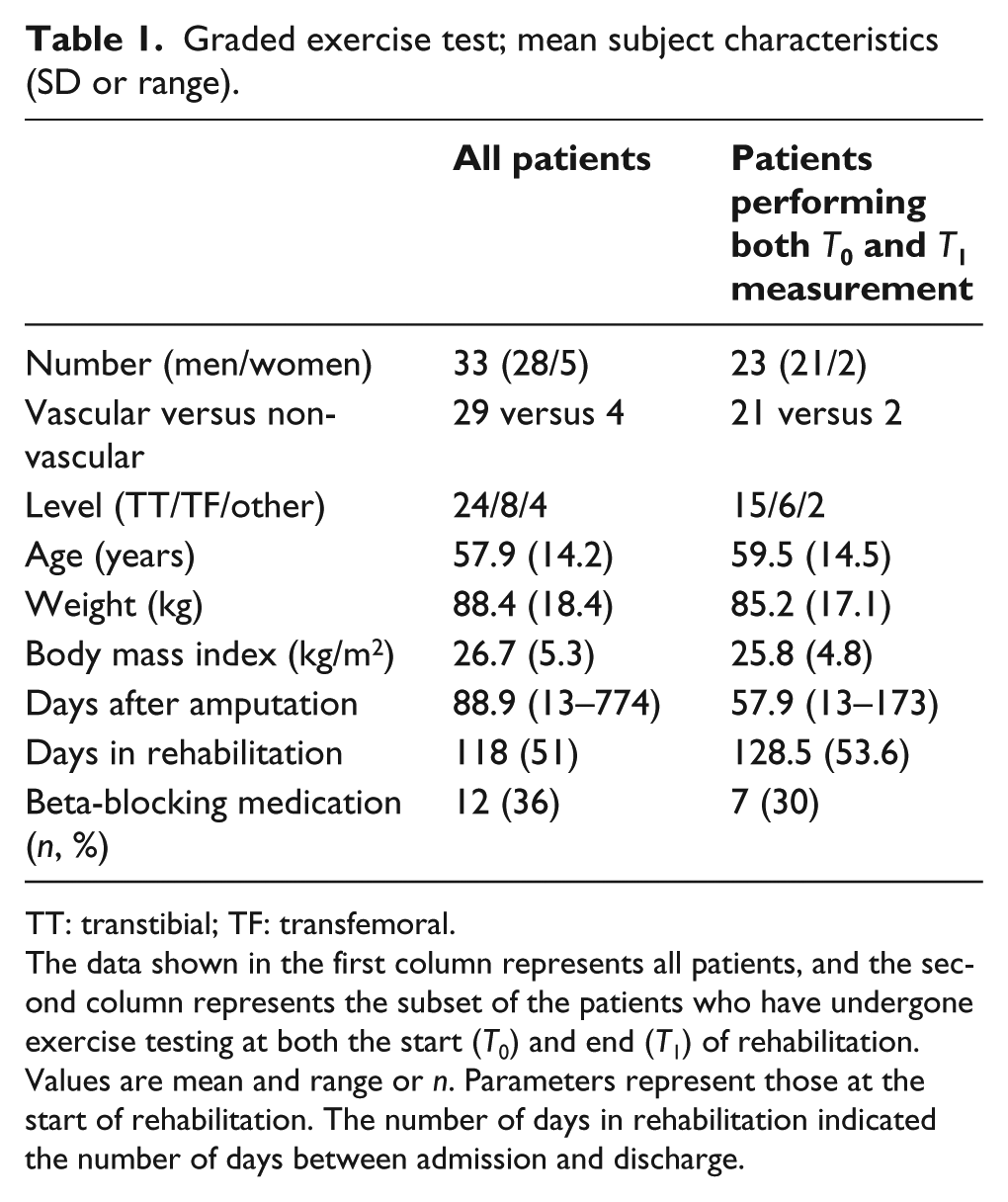
TT: transtibial; TF: transfemoral.
The data shown in the first column represents all patients, and the second column represents the subset of the patients who have undergone exercise testing at both the start (T0) and end (T1) of rehabilitation.
Values are mean and range or n. Parameters represent those at the start of rehabilitation. The number of days in rehabilitation indicated the number of days between admission and discharge.
Activity volume; mean subject characteristics (SD or range).
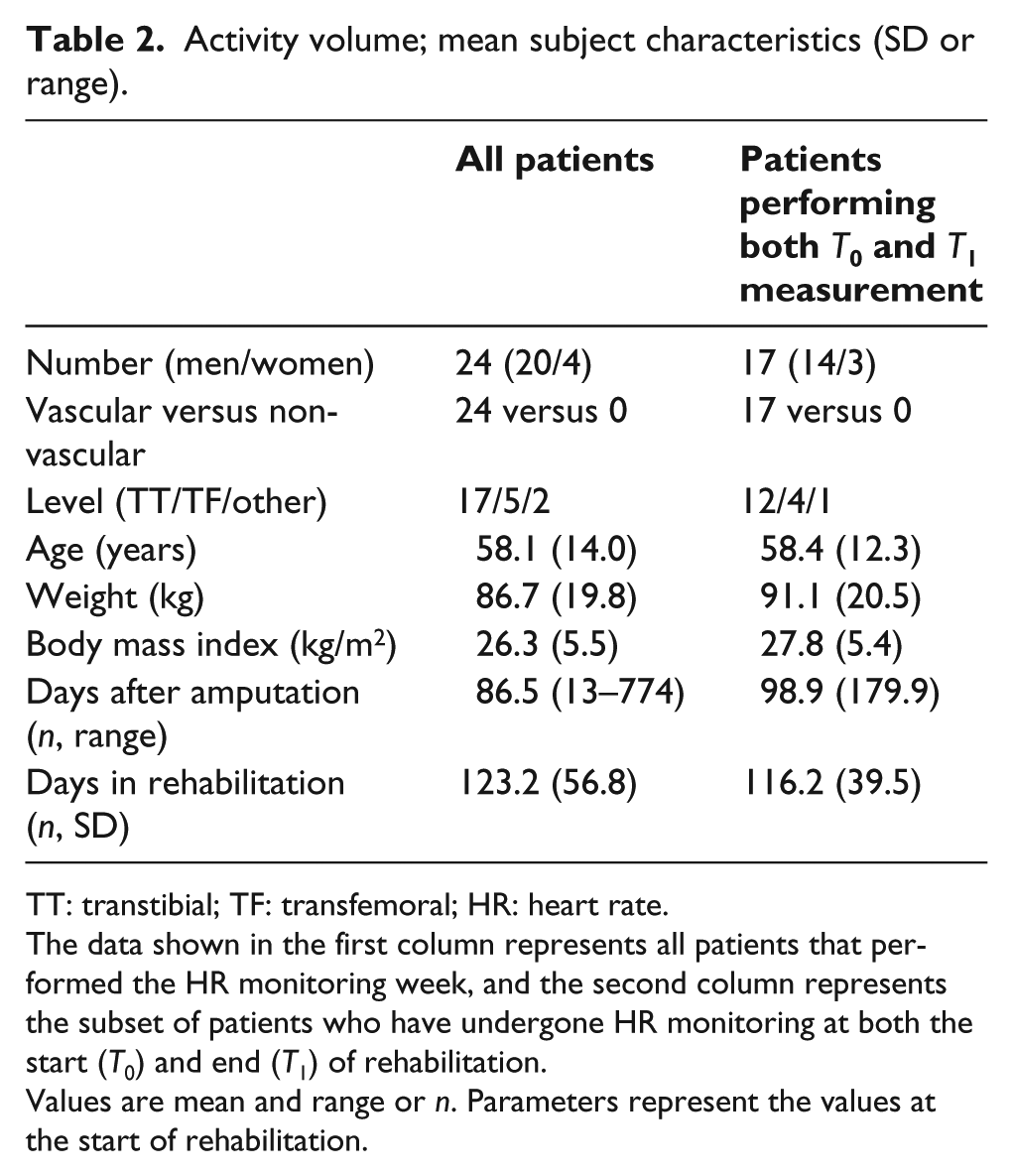
TT: transtibial; TF: transfemoral; HR: heart rate.
The data shown in the first column represents all patients that performed the HR monitoring week, and the second column represents the subset of patients who have undergone HR monitoring at both the start (T0) and end (T1) of rehabilitation.
Values are mean and range or n. Parameters represent the values at the start of rehabilitation.
Peak aerobic capacity
At the start of rehabilitation (T0), the average peak aerobic capacity obtained using one-legged exercise test was 16.9 (SD, 6.5) mL/kg/min (n = 33, Table 3). Women had an aerobic capacity of 12.8 (n = 5, SD = 3.4) and men 17.6 (n = 28, SD = 6.7) mL/kg/min. A total of 23 patients performed the second graded exercise test at the end of rehabilitation (T1). Over the course of rehabilitation, peak aerobic capacity
Graded exercise test; results.
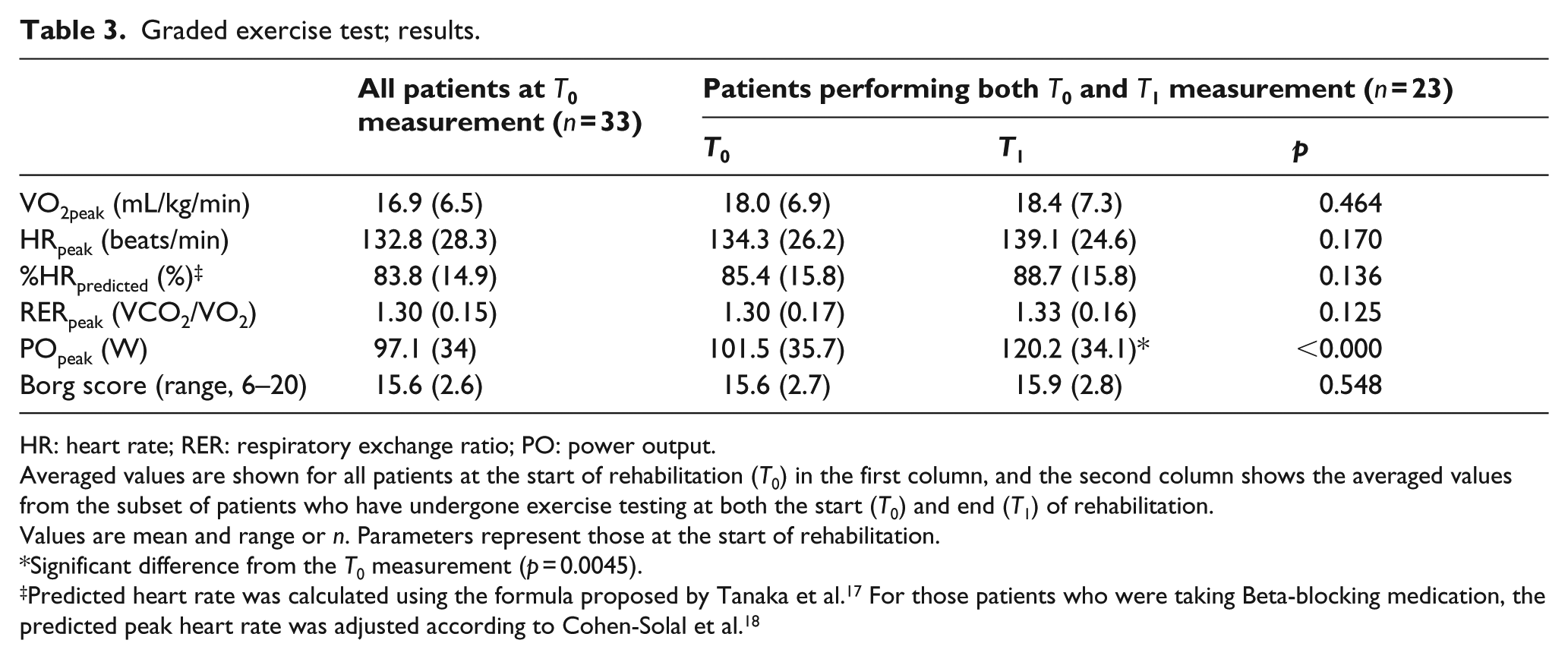
HR: heart rate; RER: respiratory exchange ratio; PO: power output.
Averaged values are shown for all patients at the start of rehabilitation (T0) in the first column, and the second column shows the averaged values from the subset of patients who have undergone exercise testing at both the start (T0) and end (T1) of rehabilitation.
Values are mean and range or n. Parameters represent those at the start of rehabilitation.
Significant difference from the T0 measurement (p = 0.0045).
Physical strain during rehabilitation
On average, 2245 (SD = 496) min of heart rate data per patient (n = 24) were recorded during a week in rehabilitation, equivalent to 4.2 9-h days (Table 4). In 17 of these patients, heart rate data were again recorded at the end of the rehabilitation period (T1). The average number of minutes recorded at both T0 and T1 and patient characteristics are shown in Table 4. Figure 2 shows the percentage of time patients spent in the different HRR zones for patients (n = 24) at the start of rehabilitation (Figure 2(a)) and for those (n = 17) who performed both T0 and T1 measurements (Figure 2(b)).
Activity volume; results.
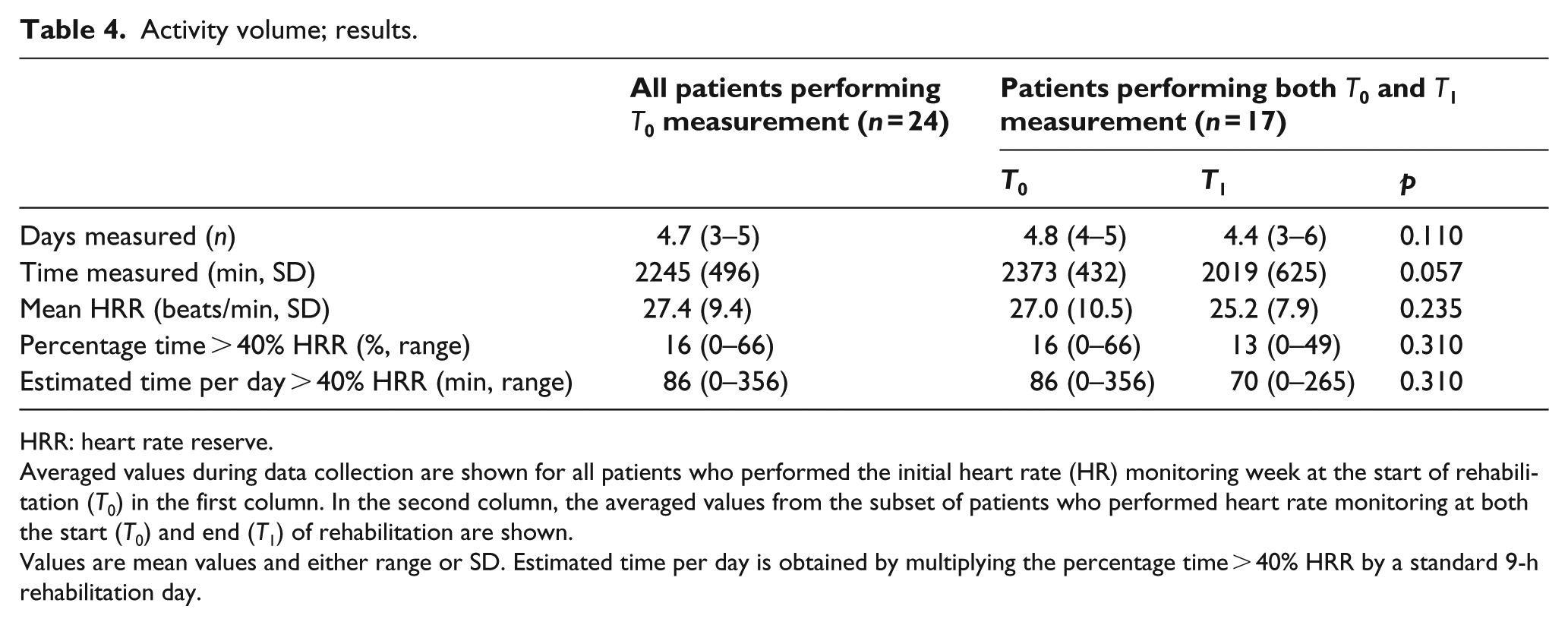
HRR: heart rate reserve.
Averaged values during data collection are shown for all patients who performed the initial heart rate (HR) monitoring week at the start of rehabilitation (T0) in the first column. In the second column, the averaged values from the subset of patients who performed heart rate monitoring at both the start (T0) and end (T1) of rehabilitation are shown.
Values are mean values and either range or SD. Estimated time per day is obtained by multiplying the percentage time > 40% HRR by a standard 9-h rehabilitation day.
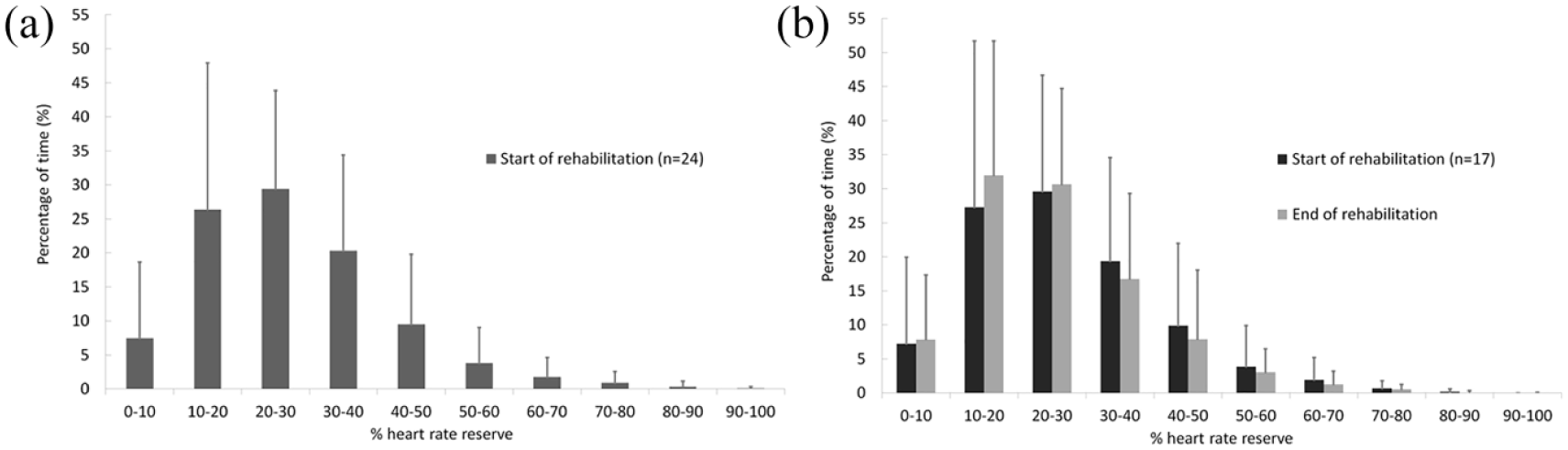
Percentage of time spent at heart rate reserve zones. (a) The averaged percentage of time spent at the different zones of heart rate reserve at the start of rehabilitation for all patients (n = 24). (b) The averaged time patients spent at the different heart rate reserves zones are shown for those patients (n = 17) for whom heart rate was monitored during both the start and end of rehabilitation. Standard deviations are shown as error bars.
At the start of rehabilitation, patients (n = 24) spent on average 16% of the total time above 40% HRR during a rehabilitation week; this would equal 86 min of moderate exercise on a full day in rehabilitation. However, large inter-individual differences were seen ranging from not spending any time above 40% HRR up to spending 66% (356 min) of the time at a heart rate above 40% HRR. In total, 12 (50%) of the 24 patients reached the criteria of spending 30 min per day above 40% HRR.
At the end of the rehabilitation program, 8 out of 17 patients (47%) reached the criteria of spending an accumulated 30 min per day above 40% HRR in at least 10-min bouts. No statistically significant differences in activity volume were found between T0 and T1. No correlation was found between the percentage increase in
Discussion
In this study, we assessed aerobic capacity and its development over the course of prosthetic rehabilitation. In addition, we monitored the activity volume during rehabilitation to account for potential changes in aerobic capacity (or lack thereof).
Peak aerobic capacity in this study was on average substantially lower (16.9 mL/kg/min) than a group of able-bodied subjects of similar age (30.8 mL/kg/min) and non-vascular amputees (28.1 mL/kg/min) who were tested using the same type of exercise test.
7
Our data are in agreement with those of Chin et al.,
6
who found an aerobic capacity of 45%–65% of the age-predicted
No significant change was observed in
Examination of the physical strain experienced by the patients during prosthetic rehabilitation shows that, while on average the amount of time spent above an exercise intensity of 40% HRR is much higher than the required minimum of 30 min per day, only half of patients reached the predefined criteria at the start and end of rehabilitation. 12 In this study, patients received care as usual, which consisted of a multidisciplinary program in accordance with the Dutch guidelines for rehabilitation after lower limb amputation 20 including physiotherapy and occupational therapy sessions, different forms of sports activities (e.g. cycling, hand-bike training, or general fitness training in the gym), and counseling. As the aim of the study was to gain insight into the physical strain created by current rehabilitation programs, no attempt was made to specifically prescribe or adjust the nature of the therapies. Improving cardiorespiratory fitness is mentioned as one of the specific goals of the current rehabilitation program. However, in the current programs, this goal is not addressed specifically in a dedicated therapy session. Most often, this goal is assumed to be reached in conjunction with other goals within the context of functional training and coaching. Our data reveal that this approach seems insufficient to elicit potential improvements in cardiorespiratory fitness as it insufficiently stresses the cardiorespiratory system in a large number of patients.
Over the course of rehabilitation, patients acquire a prosthesis and increase their level of mobility using this prosthesis. Based on this expected increase in mobility, one would expect the activity level and concomitant physical strain at the end of rehabilitation to be higher than at the start of rehabilitation. This was not the case in the cohort investigated. This is surprising and in contrast to the principle of progressive intensity that is advocated in general exercise programs.
The lack of improvement in aerobic capacity in our cohort over the course of rehabilitation might be explained by the insufficient physical strain that was experienced by a large number of patients. Interestingly, however, those who spent more time above the 40% HRR were not more likely to have an improved aerobic capacity at the end of rehabilitation, as evidenced by the non-significant correlation. This seems counterintuitive as higher aerobic strain during rehabilitation would be expected to result in more likely improvements in aerobic capacity especially in a deconditioned population as the patients in this study. Although the non-significant correlation might be affected by the small number of patients included in the analysis, there might be other explanations. The efficacy of an exercise program relies not only on intensity and duration of exercise but also on type and frequency of exercise and a progressive increase in these parameters, generally referred to as the FITT principle. The collective observations of this study suggest that cardiorespiratory fitness training requires a more dedicated approach within the rehabilitation program. Specific training sessions aimed at improving physical capacity need to be implemented in the program and exercise intensity, duration, and frequency systematically imposed and closely monitored for individual patients.
Several methodological considerations need to be discussed in relation to this study’s validity and generalizability. Assessment of peak aerobic capacity in this patient population is not straight forward because of the challenge of finding a suitable type of exercise that can be performed with one leg and because of the (cardiovascular) comorbidities of this relatively frail patient population. We adopted a one-leg cycle ergometer test that we previously developed and validated 15 and that resembles a protocol previously used by Chin et al. 6 The validity of this peak aerobic capacity assessment is to a large extent related to the ability, willingness, and/or motivation of the patient to perform maximal exercise. One often used criterion for maximum effort is reaching an RER of >1.1. Only two out of 33 patients failed to reach this criterion (both reached an RERpeak of 1.01). Another criterion is the percentage of age-predicted maximal heart rate reached. 17 Five patients in our cohort failed to reach the required 70% of their predicted maximal heart rate (none used Beta-blockers and all reached an RER > 1.1). Hence, while the majority of the patients complied with criteria for maximal aerobic exercise, it cannot be certain that all patients achieved maximal performance. This could have underestimated the peak aerobic capacity and overestimated the activity volume during prosthetic rehabilitation.
Another consideration is our method of assessing and presenting physical strain. We aimed to record heart rate for all participants during 5 consecutive full days in rehabilitation (8 am–5 pm). However, this was not realized as some patients had to skip rehabilitation during part of this time due to other obligations (e.g. hospital visits) or days of illness. Therefore, we analyzed the data for the available days (minimally 3) and for the available time periods on those days and expressed time in the relevant HRR zones as a percentage of the measurement time. These percentages were converted back to an estimated time spent in the relevant HRR zone for a full 9-h day in rehabilitation. This conversion should be kept in mind when interpreting activity time in this study. We assume that patients did not exhibit different levels of physical strain during the times where data were not obtained. However, this might not be true in all cases. For instance, during a day of illness, patients are likely less active. Not taking these into account will overestimate the average physical strain. In addition, it should be acknowledged that we did not monitor activities in the evening. Although we might assume that patients are relatively sedentary during these hours, we cannot rule out that activities in the evening period also contribute to the total physical strain experienced by the patients.
Finally, this study was subject to a selection bias as only patients admitted to prosthetic rehabilitation and who had no contraindications for graded exercise testing were included in the study. Considering all the selection criteria, conclusions of this study are limited to relatively older but active patients who have the desire and are expected to regain walking ability with their prosthesis. An additional note about generalization should be made regarding the participating centers in this study. Although both centers are well recognized and provide rehabilitation programs according to the current guidelines, they were not randomly selected and as such are not necessarily representative of the clinical rehabilitation centers in the Netherlands or the rest of the world. Finally, a major challenge in performing longitudinal research in a clinical setting is to minimize the number of drop-outs over the course of the study. As can be seen in Figure 1, a relatively large number of patients did not complete all measurement sessions resulting in a selection bias. Therefore, we present patient characteristics explicitly in Figure 1 and Tables 1 and 2. Despite these limitations, results could provide a valuable benchmark for prosthetic rehabilitation in general.
Conclusion
Cardiorespiratory fitness seems low in older predominantly vascular patients admitted for prosthetic rehabilitation, and this does not seem to increase over the course of general rehabilitation. In general, physical strain during rehabilitation seems too low to elicit improvements in cardiorespiratory fitness. Considering that large variability in physical strain between patients exists, results stress the need for dedicated physical training modules in which intensity is monitored and imposed for individual patients.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: No competing interests are reported. No author has received additional compensation for participation in the execution or writing of the article outside their regular salary. Preliminary results of this study have been presented at the World Congress of the International Society of Prosthetics and Orthotics (June 2015, Lyon, France) as part of a broader presentation on the relevance of aerobic capacity in people after lower limb amputation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from Scientific College Physical Therapy (WCF) of the Royal Dutch Society for Physical Therapy (KNGF).