
Abstract
Background:
Infrapatellar strapping is a treatment technique used in various knee pathologies; however, its effect on pain and functional performance among young athletes has not been studied.
Objectives:
To evaluate the effect of infrapatellar strap on pain and jumping performance among young athletes diagnosed with patellar tendinopathy.
Study design:
Pre-/post-test (within-subject research design).
Methods:
A total of 16 young male basketball and volleyball athletes (age range, 12–18 years) diagnosed with patellar tendinopathy were included in the study. Infrapatellar strap was applied beneath the patella, over the patellar tendon. The athletes performed four jumping tests: squat jump, drop jump, single-leg jump, and jumps 30 s test, with and without the strap. Pain severity in the symptomatic knee during jumping was assessed using a visual analog scale and jumping performance parameters were assessed using an Optojump Next optical measurement system.
Results:
Pain severity reported by the participants decreased in drop test, single-leg jump test, and jumps 30 s test while using the infrapatellar strap compared with no strap condition (p < 0.05). No significant difference in jumping performance was found between jumping with and without the strap.
Conclusion:
The infrapatellar strap was effective in reducing local pain among young male athletes without altered jumping performance.
Clinical relevance
The infrapatellar strap can be recommended to use during physical activity as part of the physical therapy treatments for patellar tendinopathy. Given the low cost, ease to use, and being a non-invasive method without adverse effects, it is an appropriate intervention for young athletes.
Background
Patellar tendinopathy (“Jumper’s Knee”) is a common sports injury characterized by localized tenderness of the patellar tendon at its origin on the inferior pole of the patella.1,2 This overuse injury occurs when stress on a given tissue becomes greater than the ability to withstand the stress. Rapid repetitive action such as acceleration, deceleration, jumping, and landing, places tremendous stress on the extensor mechanism and the patellar tendon.3–6 Therefore, patellar tendinopathy frequently occurs in sports involving the mentioned activities with high demands on speed and power for the leg extensors like playing basketball and volleyball.2,7 Athletes with patellar tendinopathy usually present with anteriorly located knee pain, exacerbated by activity or occasionally by prolonged knee flexion. Patients can often associate the onset of pain to a period of increased sport activity. 5 Subsequently, patellar tendinopathy may result in time lost from practice, activity limitations, and performance decline.7,8
The prevalence of patellar tendinopathy was found to be high among elite athletes with a significant difference between sports with different performance characteristics (range, 0%–45%). Prevalence in professional and recreational basketball players was found to be 32% and 12%, respectively, while in professional and amateur volleyball players, the prevalence was 45% and 14%, respectively. 9
Various protocols describing the treatment for Jumper’s knee have included preventive strategies such as reducing training sessions on hard surfaces known to increase bone–tendon tension or increasing recovery times, 10 employing conservative treatments such as physiotherapy including exercises5,11–13 treatment with non-steroidal anti-inflammatory (NSAID) drugs 3 and bracing. 4 Infrapatellar bracing, strapping, or taping are frequently being used as a conservative treatment for patellar tendinopathy among athletes, yet, the exact mechanism for pain reduction or whether reducing tendon strain would contribute to the resolution of symptoms or alter the pathology of a patient suffering from patellar tendinopathy is still unclear. 4 It was previously hypothesized that the strap might disperse the force sustained by the tendon over a wider area and decrease the forces applied on the tibial tubercle;4,14 the strap might increase knee joint proprioception or change the sensory input.15,16
Several studies have supported the idea of pain reduction achieved by patellar bracing/strapping for patella–femoral pain17–19 and for patellar tendinopathy among adult. 20 However, its effect on pain and functional performance in patellar tendinopathy among young athletes has not been studied. The aim of this study was to evaluate the effect of the infrapatellar strap on pain and jumping performance among young athletes diagnosed with patellar tendinopathy. We hypothesized that the infrapatellar strap will reduce the athlete knee pain during jumping tests and improve jumping height due to the reduction in pain.
Methods
Subjects
A total of 16 male basketball and volleyball athletes from the national sports academy (Wingate Institute, Israel) participated in this study (mean age: 15.84 years). Inclusion criteria were age 12–18 and anterior knee pain due to patellar tendinopathy. Patella tendinopathy diagnosis was made via the academy’s sport physician according to a description of anterior knee pain or pain beneath the patella area, the presence of pain over a 6-week period, and a physical examination. This examination included palpation tenderness at the tendon insertion to the inferior pole of the patella, resisted knee extension pain, and single-leg squat pain (eccentric movement).5,21 Exclusion criteria were past knee surgery, patellar tendon abnormality in previous available imaging, a history of knee injury (i.e. meniscus or ligaments), and complaints of knee instability. Athletes who were diagnosed with differential diagnosis as Hoffa’s impingement syndrome or patella-femoral pain were also excluded from the study. In addition, athletes with pain at the insertion of the patellar tendon to the tibial tuberosity were excluded from this study as Osgood–Schlatter’s diseases might be a differential diagnosis at this area in this age group.22,23
The study was performed with institutional ethic committee (#0076-11HYMC) and Ministry of Health Juvenile ethic committee Approval (#HT6278) and all athletes and their parents signed an informed consent form.
Procedure
Prior to testing, weight and height of each participant were measured. The athletes performed four jumping tests: squat jump test, drop test, single-leg jump test and jumps 30 s test, with and without a standard infrapatellar strap (Uriel Meditex Ltd) The strap was applied by an expert physiotherapist beneath the patella, over the patellar tendon and adjusted for a snug fit that did not restrict circulation (Figure 1). The test order and use of the strap was randomly changed for each subject. This implies that each subject performed the same tests order with and without the strap but each subject had different order (start with strap or not and the tests order itself). The 30 s jump test, was always examined last, since it measures performance under muscle fatigue. The participant performed a warm-up of 5 min of gentle jogging prior to jumping examination. A rest interval of 90 s was interspersed between jump repetitions, while 5 min rest was performed between jump trials.
The infrapatellar strap adjusted over the patellar tendon
Jumping tests
(1) Squat jump test—a single jump from a squatting position (90° knee flexion) with hands on hips, without counter movement. Subjects were instructed to jump as high as possible; 24 (2) Drop jump test—a single jump starting from a preset height of 30 cm off the ground, landing with both feet at a distance of approximately 50% of the participant height and jumping immediately back into the air as high as they were able; 25 (3) Single-leg jump test—a single jump starting from an upright position and with a counter movement on only one leg. The subject was instructed to sink to a self-selected depth as quickly as possible and then jump as high as possible with hands held in place on the hips; 26 (4) Jumps 30 s test—performing 30 s of double-leg continuous jumps. 27
These four jumping tests were included, as each test provides different load on the knees, for example, single-leg compared with double-leg support, jumping from height and fatigue test.
For the first three tests, three jump repetitions were performed, and the average of all outcome measurement was calculated for final analysis; for the last test of 30 s jumps, a single measurement was taken.
Outcome measures
Outcome measures were pain severity and jumping performance. Pain severity was assessed via the visual analog scale (VAS) which ranges between 0 (no pain) and 10 cm (most severe pain). The participants were asked to indicate the pain in the symptomatic knee during each test.
Jumping performance parameters were measured using the Optojump Next optical measurement system (Microgate, Italy). The Optojump is an optical measurement system consisting of a transmitting and receiving bar. Each of these contains 96 light emitting diodes (LEDs) (1.0416 cm resolution). The LEDs on the transmitting bar communicate continuously with those on the receiving bar. The system detects any interruptions in communication between the bars and calculates their duration. This system can measure flight and contact times during the performance of a series of jumps with an accuracy of 1/1000 of a second. Combined with its dedicated software, a series of parameters connected to the athlete’s performance with the maximum accuracy and in real time can be calculated. 28 The jump performance parameters received via the Optojump were: (1) flight time (converted to jump height in centimeters using Bosco et al.’s 29 1983 formula); (2) gravity acceleration (flight time and contact time converted to power in Watt/kg); and (3) coefficient of variation for the 30 s jumps. The use of Optojump photoelectric cells was found to be valid and reliable and recommended for field-based assessments of vertical jump height.28,30
Statistical analysis
Data analysis was performed using the Excel (Microsoft Corporation) and SAS (version 9.4; SAS Institute Inc, Cary, NC, USA) statistical programs. The data were initially analyzed to evaluate normality distribution using Kolmogorov–Smirnov test. For the normally distributed variables, standard statistical methods were used in calculating means and standard deviation, and a paired t-test was used to evaluate the changes between with and without the infrapatellar strap conditions. For the not normally distributed variables, the median and range were calculated, and Wilcoxon signed-rank sum test was conducted for the comparison between conditions.
Pearson’s correlation test was used to analyze the correlation between the demographic characteristics (age, height, and weight), and the difference in the outcome measures taken with and without the infrapatellar strap. It was also used to analyze the correlation between the difference in jumping outcome measures and difference in pain severity. An alpha level of 0.05 was considered significant.
Sample size was calculated prior to study. In order to achieve 80% power with significance of α = 0.05, 15 subjects were required for the study.
Results
Study population
The mean age of the subjects participating in this study was 15.84 (±1.82) years; mean height 182.06 (±12.91) cm, mean body mass 71.12 (±13.93) kg, and mean body mass index (BMI) 21.27 (±2.40) kg/m2.
The effect of the infrapatellar strap on pain severity
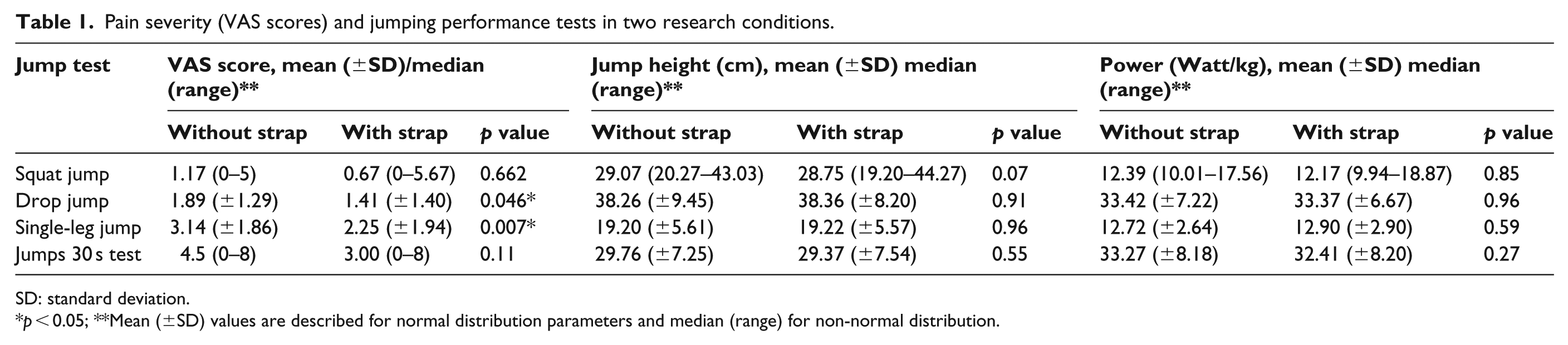
A significant difference was found in VAS results in the drop jump test (p = 0.046) and the single-leg jump test (p = 0.007) between research conditions (with and without the strap). The VAS results were lower when performing the jump tests with the strap (Table 1). No significant difference in VAS results was found between research conditions in the squat jump test (p = 0.662) and jumps 30 s test (p = 0.11), although a tendency can be observed, and the VAS was lower while exhibiting the jumps with the strap.
Pain severity (VAS scores) and jumping performance tests in two research conditions.
SD: standard deviation.
p < 0.05; **Mean (±SD) values are described for normal distribution parameters and median (range) for non-normal distribution.
The effect of the infrapatellar strap on jumping performance
No significant difference in jumping performance results was found between jumping with and without an infrapatellar strap nor was a significant difference in the coefficient of variation results with and without the infrapatellar strap (p > 0.05; Table 1).
Correlation between demographics, change in VAS score, and jumping performance
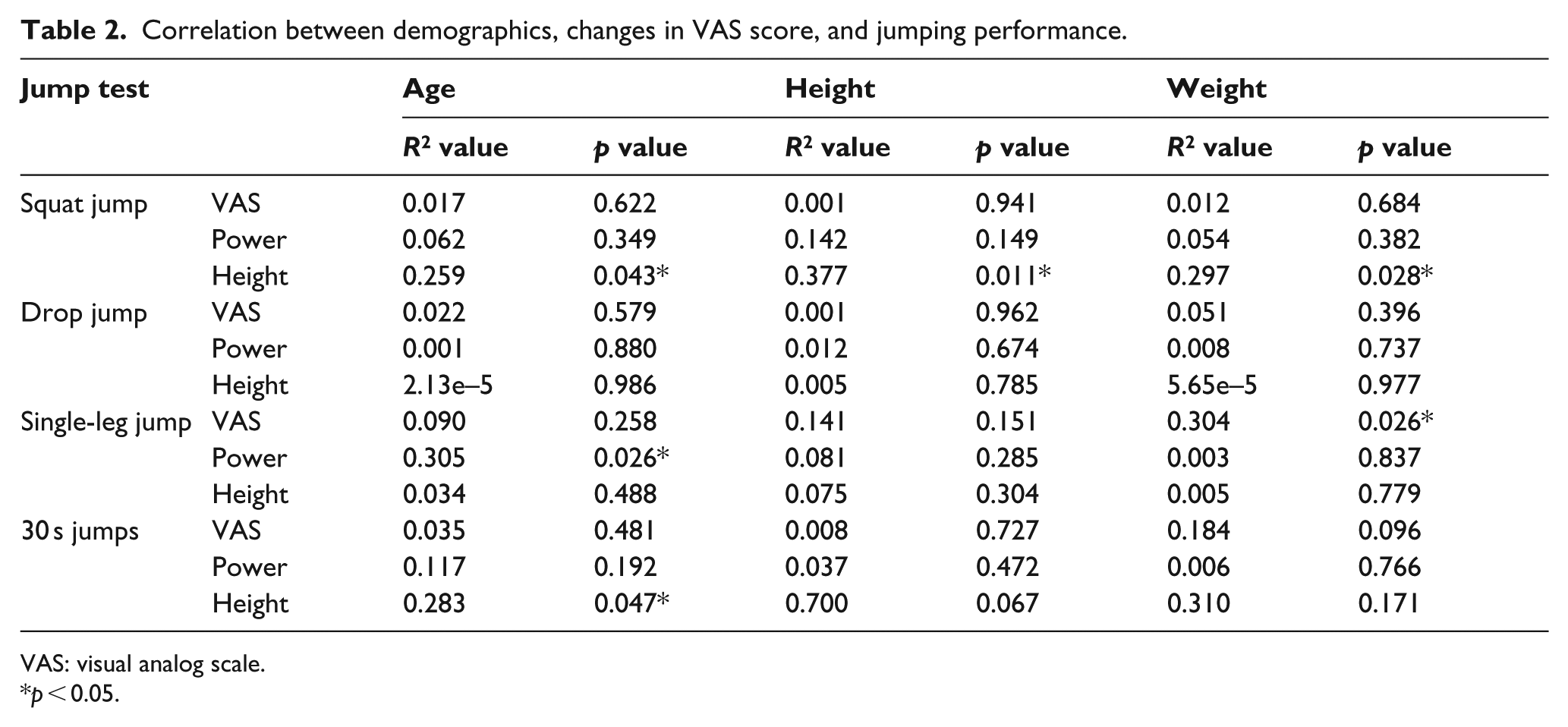
A significant correlation between changes in the VAS score and the subject’s weight was found in the single-leg jump (p = 0.026). No correlation between changes in the VAS score and other demographic characteristics was found (p > 0.05; Table 2). A correlation between the heights of the squat jump test (p = 0.043), Jumps 30 s test (p = 0.047) and the age of the subject was found, and between the power generated during single-leg jump (p = 0.026) and the age of the subject. A significant correlation was also found between the height (p = 0.011) and weight (p = 0.028) of the subjects and the height of their squat jump. No other correlations were found (Table 2).
Correlation between demographics, changes in VAS score, and jumping performance.
VAS: visual analog scale.
p < 0.05.
Discussion
Patellar bracing/strapping is commonly used for pain reduction in patients suffering from patello-femoral pain. This concept has been supported by several studies.17–19 Athletes with patellar tendinopathy also use patellar strapping; however, its effect on pain and functional improvement in patellar tendinopathy has not been studied extensively, and a lack of evidence exists as to its effectiveness.
This study examined the effect of the infrapatellar strap on pain and jumping performance among young athletes diagnosed with patellar tendinopathy. We found that the use of infrapatellar strap decreased pain severity reported by the participants in two out of four jumping tests (drop jump and single-leg jump). The most pain-provocative test was the single-leg jump test, 31 exhibiting the highest significant change in pain severity.
These findings are consistent with de Vries et al. 20 who studied the short-term effect of infrapatellar strap and tape on pain in individuals with patellar tendinopathy during the single-leg decline squat, vertical jump test, and triple hop test. The result of this study showed significant decrease in pain score while using the strap. In addition, this study compared the strap to other tapes, finding no differences between conditions claiming that any orthosis during sport can reduce pain in patellar tendinopathy. Rosen et al.32,33 examined the effect of infrapatellar strap on quadriceps’ muscle activity, lower extremities kinetics, and pain during jumping performance. Their result showed decreased pain severity while using the strap, reduced knee adductor moment, and lower activation of vastus lateralis prior to landing. Rosen’s studies compared individuals with patellar tendinopathy to healthy control using electromyography and motion analysis lab.
Other studies demonstrated similar results of effectiveness of infrapatellar strap in reducing pain; yet, the studies included patients with patello-femoral pain and not patellar tendinopathy.18,19
A possible explanation for the significant pain reduction can be found in the radiologic study of Lavagnino et al. 4 who examined 22 men with and without an infrapatellar strap. The men were laterally X-rayed in a 60° knee flexion position with and without weight-bearing (this angle represents the highest tendon tension point landing from a jump and therefore was selected). The examiners measured the angle between the patellar bone and the patellar tendon (PPTA: patellar tendon-patella angle) and the patellar tendon length (PTL). Their study showed that infrapatellar strap reduced the predicted average and maximum localized tendon strain at the site of the jumper’s knee. A strong and significant correlation between the ability of the infrapatellar strap to increase the PPTA and decrease the PTL (which indirectly decreased patellar tendon strain) and their ability to lessen the predicted average and maximum localized patellar tendon strain was found, thus decreasing the localized tendon strain can result in pain reduction as was shown in this study. Thus, we propose that a conservative symptomatic treatment will enable a continuation of sports participation in athletes with patellar tendinopathy.
Villar 34 studied 37 soldiers with patello-femoral pain treated with a standard infrapatellar strap while performing any physical activity during the day. Only 22% reported pain reduction. All soldiers claimed the strap was generally uncomfortable. None of the athletes in this study complained about strap comfortability.
The minimum clinically significant difference in VAS pain score for children aged 8–15 years (on a 100 mm VAS scale) is 10 mm. 35 Although the results in this study show a smaller difference between conditions, the tendency for pain reduction using the infrapatellar strap exists. This might suggest that another study with larger sample size should be conducted.
Studies have found that among individuals with patellar tendinopathy, there is a reduction in quadriceps strength and flexibility, altered quadriceps activation, altered jumping kinetics, and reduced sport performance.2,8,32,33,36,37 This is probably due to the pain that causes inhibition to muscle contraction. Using an infrapatellar strap was found to reduce quadriceps activation which might reduce the tensile stress in the tendon. 33 It was also found to improve knee joint proprioception which is important for jumping and performance.15,16
Despite pain reduction while wearing the infrapatellar strap, no significant difference in jumping performance results (height and power) was found between wearing the infrapatellar strap and not wearing the strap. We can assume that decreasing the localized tendon strain is insufficient to create a significant change in jumping performance results.
On the other hand, the use of an infrapatellar strap did not detract from the athletes’ jumping performance results. This specific finding is very important, demonstrating that the athletes’ jumping performance will not be altered by the use of an infrapatellar strap and therefore can be used in treatment without distress.
In a study on the immediate effect of orthotic management on grip strength of patients with lateral epicondylosis, Jafarian et al., 38 found that the use of two types of elbow orthoses resulted in an immediate increase in pain-free grip strength. Lateral epicondylosis (also known as tennis elbow) is similar to patellar tendinopathy by the nature of the pathology (overuse injury involving the tendon). As in our study, we did not find any effect of the strap on strength or performance, our possible explanation for this difference is that external orthoses might affect small muscles with smaller/shorter leverages but are not strong enough for large muscles and tendon as the quadriceps muscle.
The correlation analysis in our study revealed that subjects with a higher body mass showed greater pain improvement during the single-leg jump and improvement in their squat jump height when using the strap. Older subjects exhibited a significant improvement in jump height during two jump tests while using the infrapatellar strap, and taller subjects demonstrated a significant improvement in their squat jump height when using the strap. This result may suggest that the individual who is more mature and well developed in their body structure will have greater benefit from the strap.
The immediate applicability of the results is that using the strap as an immediate treatment for patellar tendinopathy is recommended since it is a local, conservative, self-applicable, and low cost treatment. No side effects were noted in this study. The recommendation for using the strap should be additionally added to the conservative treatment applied. Active exercised and eccentric training in particular have strong evidence for being effective for patellar tendinopathy. Most studies use the decline board squat, as the load on the patellar tendon in this position is believed to be maximized, and the knee extensor muscles activity is being greater.5,39–43
This is the first study examining the effectiveness of infrapatellar strap among adolescent population. Young athletes are still during their skeleton and muscle development. As such, some physical therapy treatments are not suitable (i.e ultrasound and shock-wave therapy) especially in the areas of open epiphyseal plates. The infrapatellar strap is a safe and appropriate treatment for young population, in addition to the recommended physical therapy. Our study lends support to the use of the strap among adolescent with patellar tendinitis for reducing pain during jumping activities. Furthermore, this study used the Optojump Next optical measurement system which calculates in maximum accuracy and in real time the jump performance and is an objective tool to assess jumping height.
Limitations
The study only examined the immediate effect of bracing on young, male athletes. The study examined strap condition to control (without strap) and did not compare the strap condition to placebo, other taping technique, or healthy group. Future research should also consider long-term effects in a larger sample size. This study examined males only, as it was previously established that patellar tendinopathy prevalence is higher in males than in females included in the adolescent population, 44 yet future research should examine how the strap effects the young female athletic population.
Conclusion
The use of the infrapatellar strap was effective in reducing local pain among young male athletes without altering jumping parameters. Although no immediate effects were observed on jumping parameters, it can be assumed that the reduction in pain will cause better performance of the athlete during practice or match.
Given its low cost, ease of use, and the fact that it is an appropriate intervention for young athletes, the infrapatellar strap can be recommended to use during physical activity in addition to other physical therapy modalities (e.g. appropriate exercise and manual therapy) for patellar tendinopathy.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.