
Abstract
Background:
Scoliosis is common in children with neuromuscular deficits. It is often associated with an asymmetric sitting position and with poor balance. Many children with neuromuscular scoliosis spend most of their day sitting.
Objectives:
To describe how sitting function is affected by treatment with a modified custom-moulded Boston brace in children with neuromuscular scoliosis.
Study design:
Retrospective review of medical records.
Methods:
A review of medical records from children fitted with scoliosis braces, including analysis of sitting, using a pressure-mapping system.
Results:
A total of 106 children with a median age of 11.3 (1.7–17.7) years were included. The most frequent diagnoses were cerebral palsy (n = 33) and myelomeningocele (n = 17). Around 56 children could sit without support and 24 children were independent walkers. The Cobb angle was between 19° and 126°. Sitting function as noted in medical records improved in 73/105 children and deteriorated in five. The pressure mapping showed that symmetry was improved in 44/86 children, while three deteriorated. Stability improved in 20/40 children and seven decreased.
Conclusion:
Bracing had a positive effect on sitting function in children with neuromuscular scoliosis.
Clinical relevance
Bracing can reduce the need for support in sitting. Children with severe scoliosis can get a better sitting function with a brace. Sitting analysis with pressure mapping can identify sitting problems needing correction of the brace and adaptations of the chair.
Background
Scoliosis is common in children with cerebral palsy (CP), myelomeningocele (MMC) and neuromuscular disorders (NMDs).1 –7 There are several factors that can contribute, such as lack of postural control, increased or decreased muscle tone, muscle weakness, muscle contractures and congenital vertebral malformations.3 –5,8 –11 Scoliosis is many times associated with an asymmetric sitting position and an increased risk of pressure ulcers. 12
In children with CP, MMC and NMD, there is a relationship between motor function and the presence of scoliosis, with a higher incidence in children who do not have the ability to walk.2,3,5,7,10,11,13 This means that many children with scoliosis spend most of their time sitting. Having a stable sitting position is a prerequisite for active participation in various activities, and a lack of postural control can compromise vital functions such as the ability to communicate. A more upright posture facilitates head control, which is often essential for children using alternative communication. A stable position can also free arms/hands from acting as support and can then instead be used for activity and participation. Sitting function can be expressed in terms of symmetry, stability, postural alignment (representing International Classification of Functioning, Disability and Health (ICF) body functions) and motor ability (ICF activity). 14
Treatment options for scoliosis are conservative or surgery. A meta-analysis has shown that treatment with a scoliosis brace for more than 23 h a day has good results in children with idiopathic scoliosis. 15 Success in brace treatment is dependent on how flexible the scoliosis is at the start of treatment.16,17 Rigo et al. 18 have shown that conservative treatment diminishes the need for surgery.
For children with neuromuscular scoliosis, both bracing and surgery are used.5,10,11,19 –21 There is a discussion regarding the effect by bracing on the scoliosis in these groups.12,20 Studies have shown that if the Cobb angle is less than 45° at the start of treatment, it can have a positive effect in patients with MMC and CP.20,22 Two studies describe better sitting function with a brace in children with neuromuscular scoliosis.19,20 Surgery is not possible in some patients for medical reasons, thus making a brace necessary. In addition to reducing scoliosis, one aim of bracing can be to improve sitting function.
The purpose was to describe how sitting function is affected by a spinal brace in children with neuromuscular scoliosis and to identify whether there are differences in the effects of bracing between children with different functional levels.
Methods
In the western part of Sweden all children with neuromuscular scoliosis is referred to Sahlgrenska University Hospital for treatment, with cooperation between the Departments of Orthopaedics, Prosthetics and Orthotics and the Regional Rehabilitation Centre. The children stay at the Regional Rehabilitation Centre for 1–2 weeks when they get their first brace. The aim of this period is that the brace should be well fitted to the child and to adjust the chairs to the new condition. The child should be accustomed and comfortable to use the brace in different situations and the families well informed and able to handle the brace.
A retrospective review was made from medical records of all children with neuromuscular scoliosis fitted with scoliosis braces during 2003–2010. All braces were of a Boston type, 23 mostly made after a mould.
The children were classified according to sitting ability, walking ability and severity of scoliosis:
Sitting ability was classified according to the Level of Sitting Scale (LSS), 24 where sit with support includes grades 1–4 and sit without support grades 5–8.
Walking ability was graded as independent walkers or non-walkers, using different systems depending on diagnosis: for children with CP, the Gross Motor Function Classification System (GMFCS) 25 was used, where grades I–III are classified as independent walkers, children with MMC and paraplegia/tetraplegia were classified according to Hoffer et al., 26 where grades 1–2 are classified as walkers, and children with NMD were classified according to Vignos et al., 27 where grades 1–6 are classified as walkers. For other diagnoses, the GMFCS was used.
Scoliosis was measured with the Cobb method. The severity of the scoliosis was classified in two groups according to whether the primary curve was ≥ 46º.
Sitting analysis with and without the brace was made sitting on a bench and with registration with a pressure-mapping system (force-sensitive applications (FSAs), Seat & Back System 4th edition, Verg Inc, Canada, and TekScan, CA Mätsystem AB, Stockholm). The children sat without a backrest, with the feet on the floor, for 90 s. Children who could not sit independently were supported for balance at the shoulders by a physiotherapist. The pressure-mapping measurement and a normative material are described by Olsson et al. 28 and have good reliability.
Differences in seat-load symmetry and stability between sitting with and without the brace were graded in a three level ordinal scale: positive, no change or negative. Seat-load symmetry is the proportion of the mean values of pressure distribution on the right and left sides of the anatomical midline, presented as percent, as measured with the pressure-mapping system. Seat-load symmetry was compared with the normative material, where a variation between sides up to 40%/60% is normal in typically developing children. Changes in seat-load symmetry were graded as positive if it changed from asymmetric to symmetric according to the normative material or with at least 20%-units improvement and vice versa if a negative change was present. Stability was assessed by the sway seen in the pressure-mapping measurement, calculated from the standard deviation of the mediolateral excursion of the centre of pressure (COP), which was compared with the normative material. 28 Stability was also noted as changes in the children’s ability to sit, graded with the LSS.
Information on effects sitting in their regular chair, which could be attributed to the brace, was retrieved from physiotherapy and occupational therapy records. Data were categorised, first independently by a physiotherapist (A.B.) and an occupational therapist (K.O.) and then in a discussion to reach consensus.
The study was approved by the ethics committee in Gothenburg Ö583-01, 2002-01-24.
Statistical methods/data analysis
As the group was considered heterogeneous, nonparametric statistics was used. The Pearson Chi square test was used for comparison between subgroups, and the sign test for analysis of changes with the brace. Statistical analyses were made with software SPSS, version 20 and at statistics website http://www.infovoice.se/fou/.
Results
A total of 127 patients were found: six were excluded due to brace only for sitting purposes and seven with only kyphosis and no scoliosis, leaving 114 who met the inclusion criteria. The braces were in most cases made after a plaster mould. The brace treatment was not fulfilled in two children due to a poor medical condition, and there were no data on sitting function in six other children. Finally, 106 children were included in the study, see Figure 1.
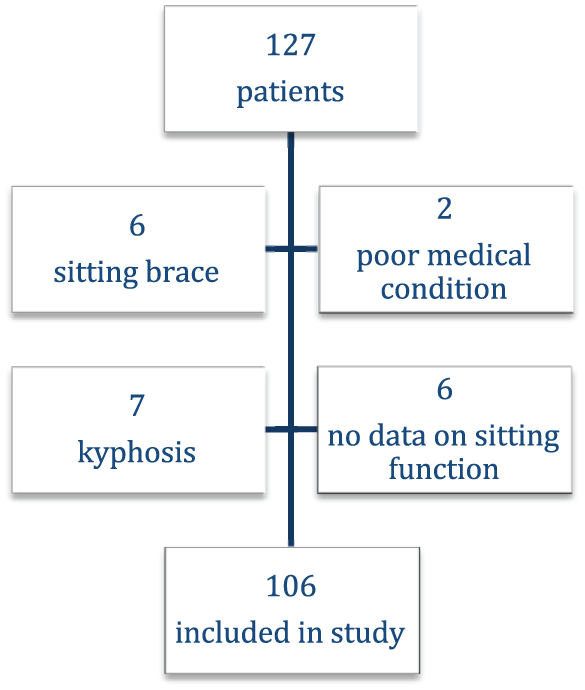
Flow chart of participants included in the study.
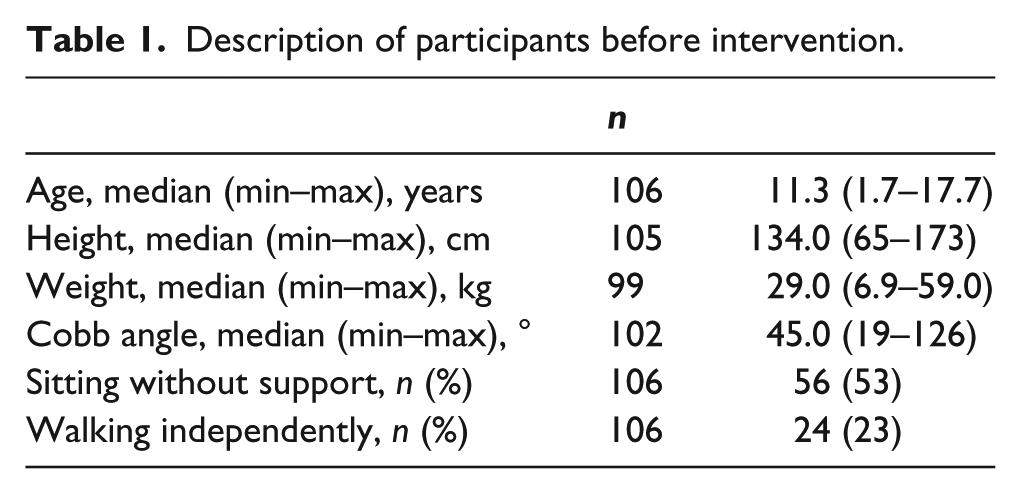
A description of the participants is given in Table 1. There were 58 girls and 48 boys with a median age of 11.3 years at the start of treatment. Around 56 children could sit without support and 24 were independent walkers. X-rays in sitting without a brace were available in 102 children, of whom 59 had a Cobb angle between 19° and 45°, and 43 had more severe scoliosis with a Cobb angle between 46° and 126°.
Description of participants before intervention.
The most common diagnoses were CP (33 children) and MMC (17 children). Other diagnoses with less than 10 children in each group were: spinal muscular atrophy, arthrogryposis multiplex congenita, Duchenne muscular dystrophy, encephalopathy, Prader–Willi syndrome, MB Down and other syndromes.
Sitting analysis with pressure mapping was available in 86 children. Comparing children needing support to those sitting without support showed more seat-load asymmetry in children needing support, with an asymmetric distribution in 31/38 (81.6%), compared to 19/48 (39.6%) in children sitting without support (χ2 = 15.369, df = 1, p < 0.001). Both seat-load symmetry measurements and X-rays were available in 84 children, showing that asymmetry in sitting was more frequent in those with a more severe scoliosis, with an asymmetric distribution in 26/36 (72.2%), compared to 22/48 (45.8%) in those with a smaller curve (χ2 = 7.360, df =2, p = 0.025).
Changes with the brace
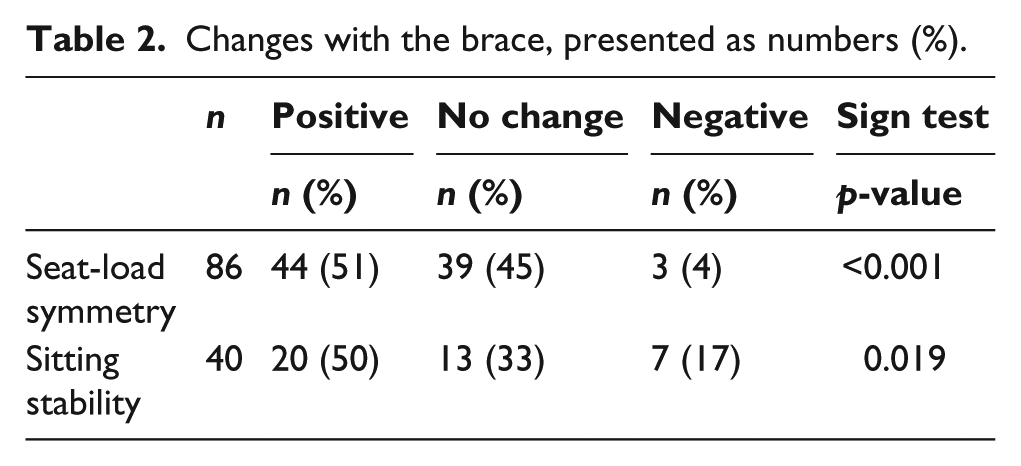
Changes in sitting variables are presented in Table 2 and Figures 2 and 3. There was a statistically significant improvement for both seat-load symmetry and stability with the brace. This was present both in children with small and severe scoliosis.
Changes with the brace, presented as numbers (%).
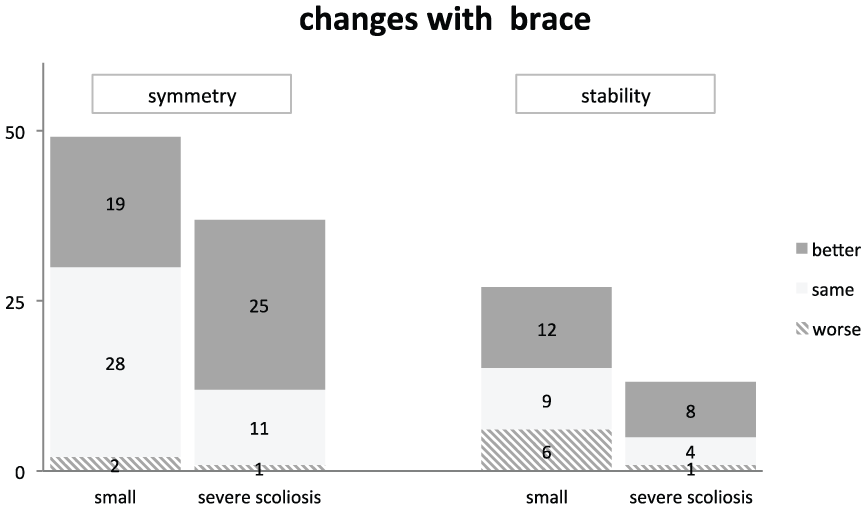
Changes with scoliosis brace divided according to severity of scoliosis. Figures indicate the number of children.
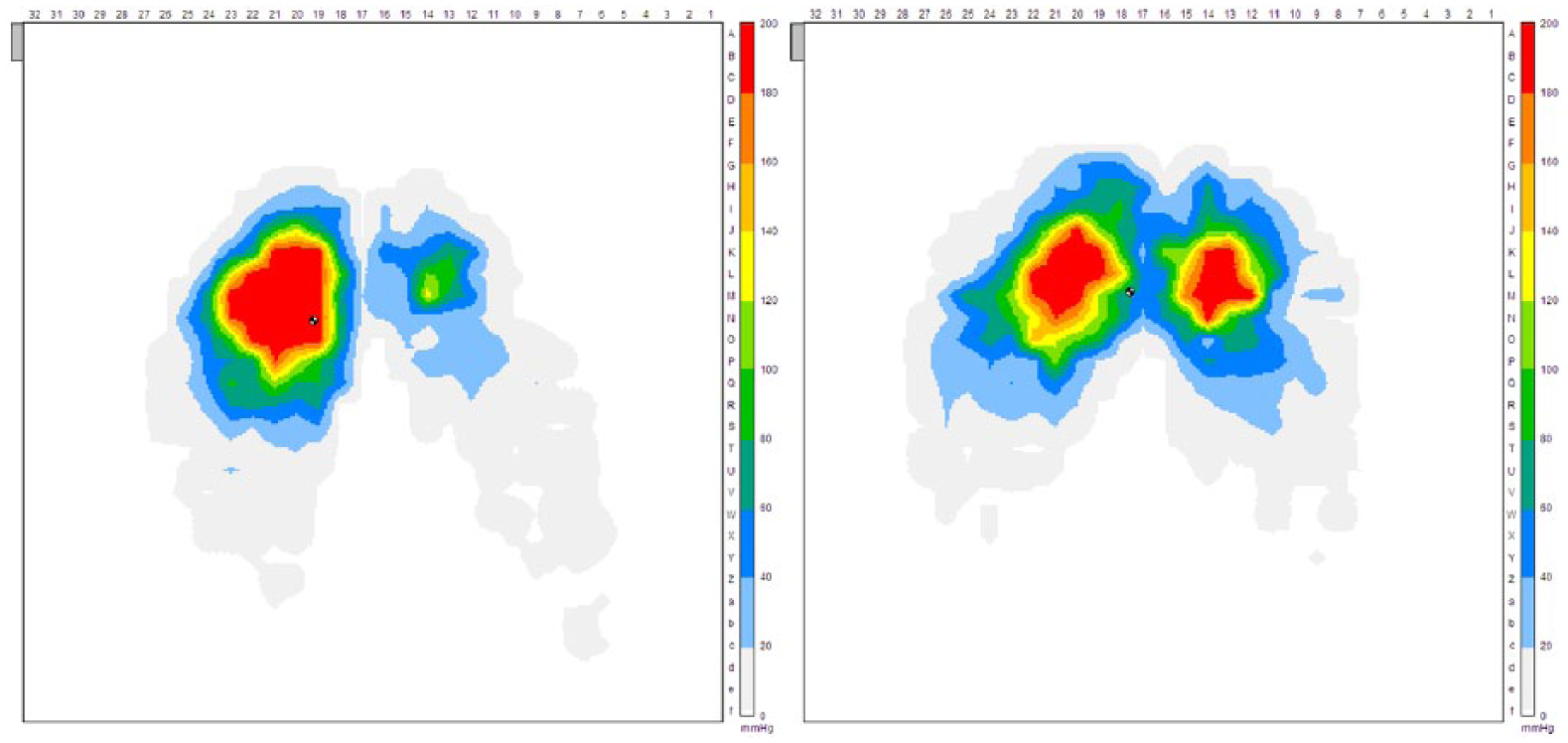
Example of pressure mapping, without and with brace.
The calculation of seat-load symmetry in sitting was compared to the normative material, where 36 of the children were within normal variation without the brace, which increased to 57 with the brace (see example in Figure 3). Seat-load symmetry improved without reaching normal values in another 23 children. Symmetry deteriorated in three.
Stability was analysed in 40 children, with 20 improving and seven deteriorating.
It was possible to calculate stability in terms of the standard deviation of COP in 35 children sitting without support. Improvement was seen in 16 children and deterioration in 6 according to the COP measurement. Stability also improved in four children as graded with the LSS, being able to sit without support with the brace. One child deteriorated and could not sit without support with the brace.
In 20 children, problems were identified in the sitting analysis even if not all of them deteriorated with the brace. This was expressed as need of support, increased sway or decreased seat-load symmetry, needing correction in their regular chairs or adjustment of the brace. In two children, and after control with X-ray, this led to a decision to make a new brace. In four children with deteriorated stability, the braces were adjusted to allow more flexion of the hips. These changes were controlled by a clinical reassessment but with no further pressure mapping. In nine children with asymmetric seat load, the seat of the chair was adjusted with extra material on one side, to improve seat-load symmetry. Pressure mapping was used to try out the height of the extra material needed. For one child, who had a distance in the chair before the brace, this could be removed, as the position became symmetric with the brace. Three children had mixed changes of their chairs and one child needed more time to get accustomed to the brace before finding balance in sitting.
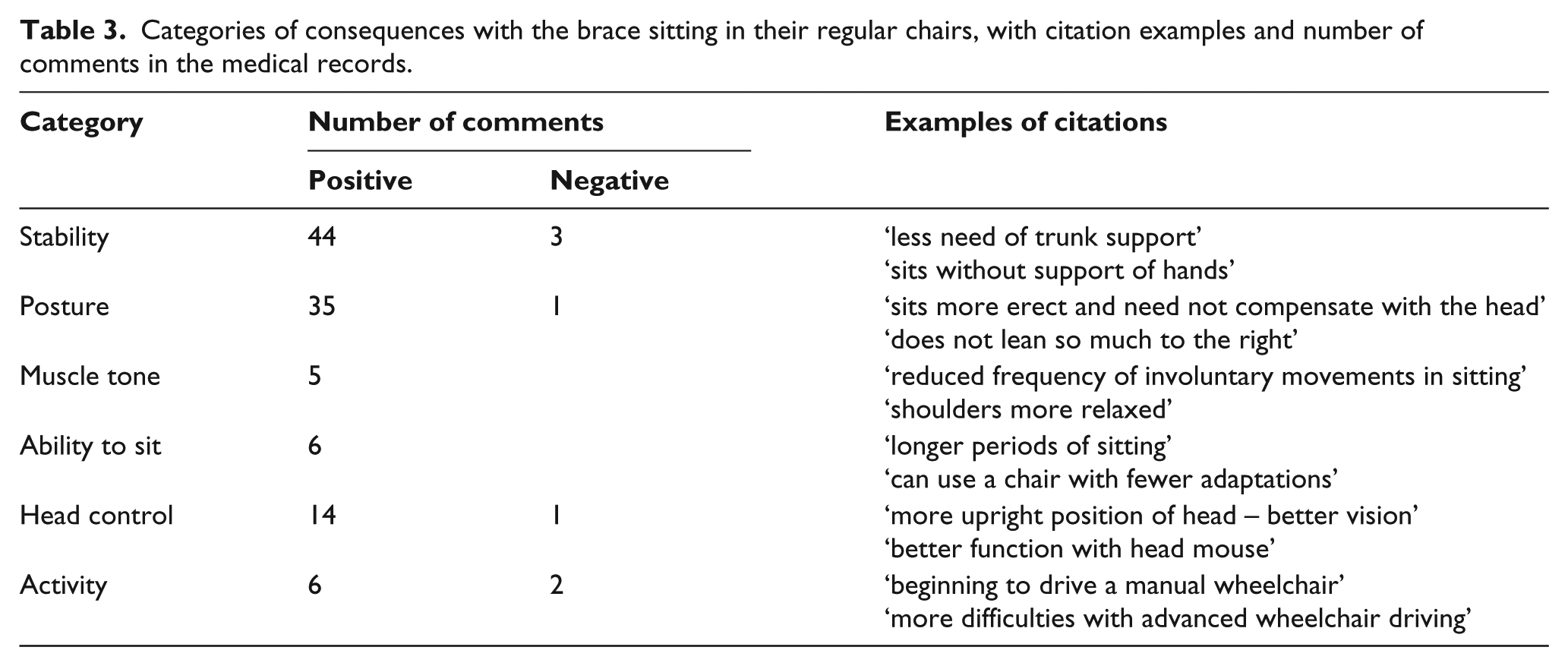
Notes on sitting in their regular chairs were described in the medical records of 105 children, with positive changes in 73 and negative changes in five of the children. Five children had both positive and negative consequences. The changes were categorised into six groups: stability, posture, muscle tone, ability to sit, head control, and activity. The most frequent comments were in stability and posture, for examples of citations see Table 3. Around 14 children needed less external support in their chairs, and three could not sit at all without the brace. The proportion of children with improvement was greater in the group who needed support with 43/49 (87.8%) improving, compared to 30/56 (53.6%) of children being able to sit without support.
Categories of consequences with the brace sitting in their regular chairs, with citation examples and number of comments in the medical records.
Complications
Negative consequences, not directly concerning sitting, were reported in 19 children. These included comments on gross motor function (eight children) and activities in daily life (ADL) (two children). In three children, the parents reported that the children were less active or satisfied and needed longer time to getting used to the brace. Six children had more difficulties in feeding, and one child could not continue the brace treatment because of problems with both feeding and respiration. No children had problems with pressure ulcers.
Discussion
The study shows that bracing had a positive influence on sitting function in children with neuromuscular scoliosis. The greatest improvements were seen in children who needed support in sitting, but children able to sit without support also improved with the brace. The need of external support and the number of special adaptations of the chair decreased for many children when using the brace. The findings in our study comply with a study by Terjesen et al., 12 who found a positive effect on sitting function in 57 children with CP treated with a Boston brace, where 72% of the patients continued to use the brace at 22 years of age. Together, this indicates that a brace is a good treatment option for sitting problems in children with neuromuscular diagnoses.
The use of braces varies a great deal around the world. For patients with scoliosis >45°, surgery is often the recommended treatment,20,29 and children with scoliosis >45° do not always get a brace. In our study, we could see that bracing had a positive effect on sitting function in this group. When choosing between different treatment options, you can consider the positive effect on sitting function in children with severe problems, where bracing can have a double function, such as sitting support and preventing further deterioration of the scoliosis.
Sitting analysis on a bench with pressure mapping is a way to identify and understand the child’s need of support. It can assess the sitting function and guide in whether and what adjustments are needed for a functional sitting position. The standardised position on the bench makes it possible to repeat and compare at different times, which is not the case in the child’s regular chair, where there may be a different chair next time and with other adjustments. The more objective way of describing sitting has been a way to communicate in the team of physiotherapists, occupational therapists and orthotists and to understand the special needs in these groups. We have noted that the need for adjustments to allow more hip flexion in the braces were more frequent in the first years of the study. The importance of sufficient hip flexion in the brace in children spending most of their time sitting differs from braces in children with idiopathic scoliosis. Visualising the pressure distribution with the pressure mapping also helps children, parents and caregivers to understand sitting problems, and when you can see the improvement, it can act as a strong motivation to use the brace. However, the sitting analysis with pressure mapping does not reflect the children’s everyday sitting in different chairs, so the measurements were supplemented by inspection of the children sitting in their regular chairs as reported in the medical records. With the brace there were negative effects on gross motor function and ADL in some children. Our experience is that this is often temporary and could mostly be addressed by allowing more time to get accustomed to the brace and for retraining skills. Problems with feeding usually also decrease over time but sometimes you have to make special adaptations on the brace or reduce the time wearing the brace.
Limitations
There are some limitations that need to be acknowledged in this study, affecting the generalizability. The group of children is heterogeneous; the background of the sitting problems varied and the age span was wide, with children from 1 to 17 years of age.
It was not possible to make a sitting analysis with pressure mapping in all patients owing to severe spasticity, lack of postural control and contractures, making it impossible to place them on the bench. For children needing support in sitting, a physiotherapist was holding the child at the shoulder level in a balanced position, which is difficult to standardise. Pressure-mapping measurements with and without the brace were however made on the same occasion, allowing the physiotherapist to support in the same way.
Data on effects that could be attributed to the brace are collected from several therapists, which can compromise reliability of the findings. But the therapists at the unit have a long experience in the field and are familiar with common functional problems in the included patient groups. No standardised instruments for measurement of motor function were used. This is explained partly by the fact that this is a retrospective study and with children at different functional levels and various diagnoses and no common formal evaluation of motor function is made. However, impact on function in everyday life is important, and this information in the clinical records helps us to identify important aspects with respect to the brace.
This study only describes the effect on sitting function during the 10-day hospital period for weaning in the brace. However, changes in sitting function can be seen and described momentarily. Terjesen et al. 12 described the same positive effects on sitting function. In a previous follow-up of children with CP who had been fitted with a scoliosis brace, 12/20 children still used the brace at least 23 h a day after a mean of 2.9 years, and positive effects were reported on sitting, standing and quality of life (personal communication).
To evaluate the effect on the scoliosis you need a long-time follow-up with X-ray. In our study, however, the purpose was to focus on sitting function and not on scoliosis treatment. As we believe that the thorough sitting analysis makes it easier for the child to use the brace fulltime and helps the parents to understand the positive effects with bracing it would be of great interest to make a follow-up on the long-term effects on both sitting function and scoliosis in these groups.
Conclusion
A scoliosis brace has a positive effect on sitting function in children with neuromuscular scoliosis.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Financial support was provided by the Petter Silfverskiöld foundation and the Research and Development Foundation of Göteborg and Bohuslän.