
Abstract
Background:
The effect of plantar flexion resistance of ankle–foot orthoses on the ankle and knee joints is well known, but its effect on the hip joint and upper body movement during the gait of stroke patients remains unclear.
Objectives:
To compare the effect of an ankle–foot orthosis with plantar flexion stop and an ankle–foot orthosis with plantar flexion resistance on the gait of stroke patients in the subacute phase.
Study design:
Randomized controlled trial.
Methods:
A total of 42 stroke patients (mean age = 59.9 ± 10.9 years, 36 men and 4 women) in the subacute phase were randomized to each ankle–foot orthosis group in a parallel controlled trial with no blinding. Patients received gait training from physiotherapists using the specified ankle–foot orthosis for 2 weeks. Shod gait without an ankle–foot orthosis before training and gait with an ankle–foot orthosis after training were measured by three-dimensional motion analysis.
Results:
A total of 20 patients were analyzed in each group. Significant differences were found in pelvic and thoracic tilt angles between the two groups. Compared with the gait without an ankle–foot orthosis, the pelvis showed forward tilt when patients walked with an ankle–foot orthosis with plantar flexion stop, and the thorax showed decreased forward tilt when the patients walked with an ankle–foot orthosis with plantar flexion resistance.
Conclusion:
The difference in ankle–foot orthosis function in sagittal plantar flexion resistance affected the alignment of the upper body and the pelvis during the gait of stroke patients in the subacute phase.
Clinical relevance
Maintaining upright posture is important in gait rehabilitation. The findings of this study suggest that the ankle–foot orthosis with plantar flexion resistance facilitated better alignment of the upper body and pelvis during the gait of stroke patients in subacute phase. This type of ankle–foot orthosis could be beneficial for patients with malalignment of the upper body and pelvis.
Background
Ankle–foot orthoses (AFOs) are frequently used to improve the gait of patients after stroke. The findings of many studies comparing gait with and without AFOs1–3 suggest that AFOs are beneficial to velocity, ankle and knee joint kinematics, kinetics, and the energy cost of walking. There are many kinds of AFOs—articulated and non-articulated, rigid and dynamic—but the question of how to choose the appropriate AFO for each patient remains unanswered. It is therefore important to clarify the effect of AFO design characteristics on the gait of patients.
The main purposes of AFOs are to stabilize the ankle joint in stance phase, to facilitate toe clearance in swing phase, and to promote heel strike. 4 Sagittal plane resistance to dorsiflexion and plantar flexion of the ankle joint is an important design characteristic of AFOs that helps improve these problems. Most non-articulated AFOs have dorsiflexion resistance, which has been found to assist the eccentric contraction of the plantar flexors and to stabilize the ankle and knee joints in stance. 5 However, some studies have shown that articulated AFOs lacking dorsi flexion resistance showed larger increases in velocity and dorsiflexion angle in stance compared with the non-articulated AFOs.6,7 Plantar flexion resistance facilitates toe clearance in swing phase and promotes heel strike. To prevent foot drop, most traditional AFOs restrict the movement of the ankle joint into plantar flexion. However, some studies have shown that restricted plantar flexion induces undesired knee flexion in early stance phase.7,8 The plantar flexion resistance of AFOs also plays an important role in the first rocker function.9,10 In normal gait, gradual movement into plantar flexion, supported by eccentric contraction of the dorsiflexors, controls shank rotation and achieves smooth weight shift to the leading limb in loading response. 11 Previous studies have shown the importance of adjusting an AFO’s plantar flexion resistance appropriately for each patient’s condition. 12 Kobayashi and colleagues13–16 showed systematic change of ankle and knee joint kinematics and kinetics with increased AFO plantar flexion resistance. They demonstrated decreases in both ankle plantar flexion in early stance and knee extension in late stance and increased knee flexion in early stance in relation to the increased plantar flexion resistance of the AFO. Other studies have shown that AFOs with adjusted plantar flexion resistance significantly improve the gait of stroke patients compared with the shod gait without an AFO.17,18 These results have helped clarify the effect of AFO plantar flexion resistance on the gait of stroke patients; however, the effects examined were limited to the ankle and knee joints, which are directly affected by AFO function. Moreover, the number of study subjects was limited.13–18
The recovery of stroke patients begins at stroke onset, with the recovery curve rising to a plateau at around 6 months post onset. 19 The subjects who participated in previous studies examining the effect of plantar flexion resistance were in the chronic phase, more than 181 days after onset.13–18 Sensitive outcome measures of gait recovery have been shown to differ between patients in the chronic phase compared with the subacute phase.19,20 This study was therefore performed to investigate the effect of the plantar flexion resistance of AFOs on the gait of stroke patients in the subacute phase. To accomplish this, the gait of patients with an AFO with plantar flexion stop (AFO-PS) and patients with an AFO with plantar flexion resistance were compared by a randomized controlled trial. Previous studies have suggested that plantar flexion stop induces increased dorsiflexion and knee flexion in the early stance phase of gait. This increase may induce the hip flexion. We therefore hypothesized that the kinetics and kinematics of the ankle, knee, and hip joints would be affected by AFO function.
Methods
Patients
The participants in this study were stroke patients in the subacute phase (less than 180 days after onset) who were undergoing rehabilitation at a rehabilitation center and had been prescribed the AFO and gait training using the AFO. Patients with ankle range of motion greater than 0° in dorsiflexion and spasticity grade less than 2 on the Modified Ashworth Scale 21 were included. The inclusion criteria were so defined because patients with severe contracture or spasticity had difficulty walking without an AFO. Exclusion criteria were non-concurrent pathologies affecting the central nervous system or neuromuscular system, communication problems, and proprioceptive sensory impairment. Before participating in the study, patients received gait rehabilitation from physiotherapists, but did not use any kind of AFO. In all, 42 patients met the above criteria and participated in this study. Because the first measurement was done as patients began walking 10 m with supervision, patients were assigned to two groups in order of participation with no blinding: one group wore an AFO-PS and the other wore an AFO with plantar flexion resistance. All procedures were approved by the local ethics committee of the International University of Health and Welfare and Nakaizu rehabilitation center. Informed consent was obtained from all patients prior to their participation in the study.
Equipment and protocol
The two types of AFOs shown in Figure 1 were used in this study. An AFO with metal uprights and a Klenzak joint was used as the AFO-PS. The ankle of the AFO-PS does not move into plantar flexion. An AFO with metal uprights and a mechanical ankle joint with an oil damper (AFO-OD; Gait Solution; Kawamura Gishi) were used as the AFO with plantar flexion resistance. 22 The ankle joint of the AFO-OD moves into plantar flexion with resistance that is generated by the oil damper. The magnitude of the resistance can be changed from 1 to 4 by rotating a screw located at the top of the oil damper; however, resistance was set at 3 in this study because this magnitude was used the most frequently for patients in the subacute phase. The ankle joints of both AFOs move freely into dorsiflexion. We chose AFOs with metal uprights because that type of AFO was used in previous studies that investigated the effect of plantar flexion resistance of AFOs on the gait of stroke patients.13,15,16
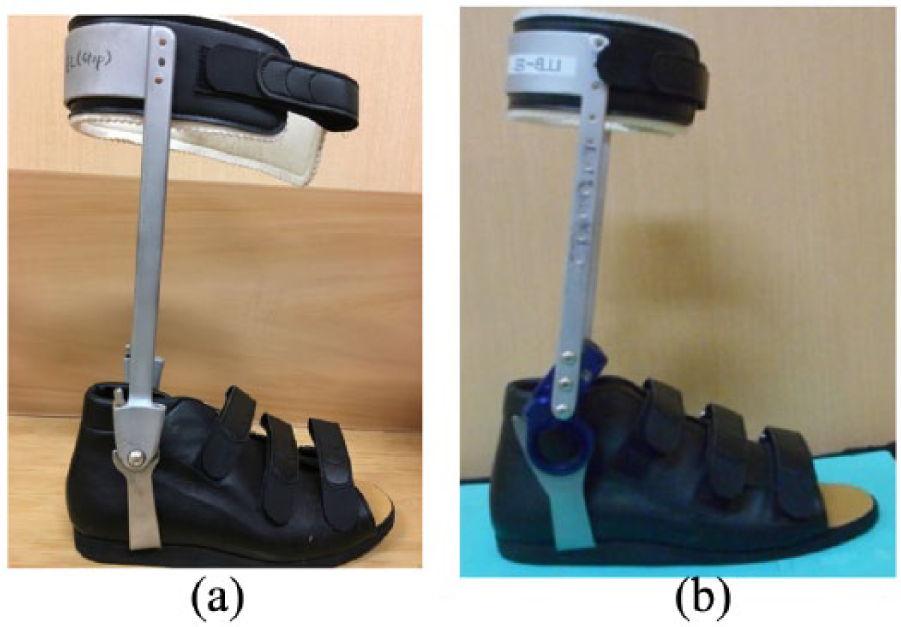
Ankle–foot orthoses (AFOs) used in this study: (a) AFO with plantar flexion stop (AFO-PS) and (b) AFO with plantar flexion resistance (oil damper; AFO-OD).
Gait was measured using a three-dimensional motion analysis system (10 VICON MX cameras and 6 AMTI force plates). A total of 34 reflective markers were attached to patients at various landmarks. Markers were placed on the thorax (spinous processes of the 7th cervical and 10th thoracic vertebrae, the xiphoid process of the sternum, and the jugular notch where the clavicles meet the sternum) and on the pelvis (both anterior superior iliac spines and the posterior superior iliac spines). Markers were also placed on the upper limbs (both shoulders, elbows, and wrists) and lower limbs (both hips, thighs, knees, shanks, ankles, heels, and metatarsophalangeal (MP) joints). Additional markers were placed on the medial aspect of the knee, ankle, and MP joints to allow accurate calculation of the joint center. Marker trajectories and force plate data were sampled at a frequency of 100 Hz. Patients wore shoes that were prepared for the experiment (V-step; Pacific Supply), which were used in usual gait training for stroke patients. The shoes were used in gait without an AFO as well as for the nonparetic foot in gait with an AFO. The use of canes was allowed if necessary and was consistent in the two conditions for each patient.
Shod gait at the patients’ selected speed without an AFO was measured. As mentioned above, the first measurement was done as patients began walking 10 m with supervision. Measurements were repeated until four paretic limb steps on the force plates had been obtained. Patients were then divided into two groups: AFO-PS and AFO-OD. Each patient participated in 1 h of physiotherapist-led gait training every day for 2 weeks, using the specified type of AFO. Gait training was performed identically between the groups. After the completion of training, gait with the specified type of AFO was measured using the same procedure described above.
Data processing
Marker trajectories and force plate data were low-pass filtered by a second-order Butterworth filter with cutoffs of 6 and 18 Hz, respectively. The link segment model consisted of 12 segments: thorax and pelvis and both upper arms, forearms, thighs, shanks, and feet. The center of gravity (COG) for each segment of the link segment model were calculated using anthropometric data. Progressive COG velocity was calculated by differentiating the displacement of the combined COG. Joint kinematics and kinetics were calculated using an inverse dynamic model. Step length was normalized by body height, and ground reaction force and joint moment were normalized by body weight. Joint angles, joint moments, and ankle power were calculated for the paretic limb. The peak values in each gait phase and the change in each phase were calculated. Because most patients did not exhibit heel rise of the paretic limb in single-stance phase, the stance phase was subdivided into loading response, single stance, and pre-swing. These phases were divided using the vertical component of the ground reaction force. In total, the 37 gait parameters shown in Tables 2 to 4 were calculated. The lateral obliquity and rotation of the pelvis and thorax were also calculated. All calculations were performed using Visual 3D software version 5 (C-Motion Inc.).
Statistical analysis
Gait parameters were measured and averaged for at least three gait cycles in each condition (without an AFO before training and with an AFO after training). Normality of the data was assessed by the Shapiro–Wilk test. A two-way analysis of variance (ANOVA) was performed for normally distributed data, with paired factors (condition, with and without) and an unpaired factor (type of AFO). If no interaction was found, the main effects of the two factors were considered. In cases of interaction, comparison was made between conditions in each AFO group using one-way ANOVA. Data without normal distribution were subjected to the Wilcoxon t-test to compare the different conditions and Man–Whitney U-test for the type of AFO. Statistical significance was set at p values of less than 0.05. SPSS version 24 for Windows was used for all statistical analysis.
Results
A total of 20 patients were analyzed in each group (Figure 2). There were no significant differences between the groups in age, body height, body weight, days after onset, or gait velocity without an AFO, as shown in Table 1.
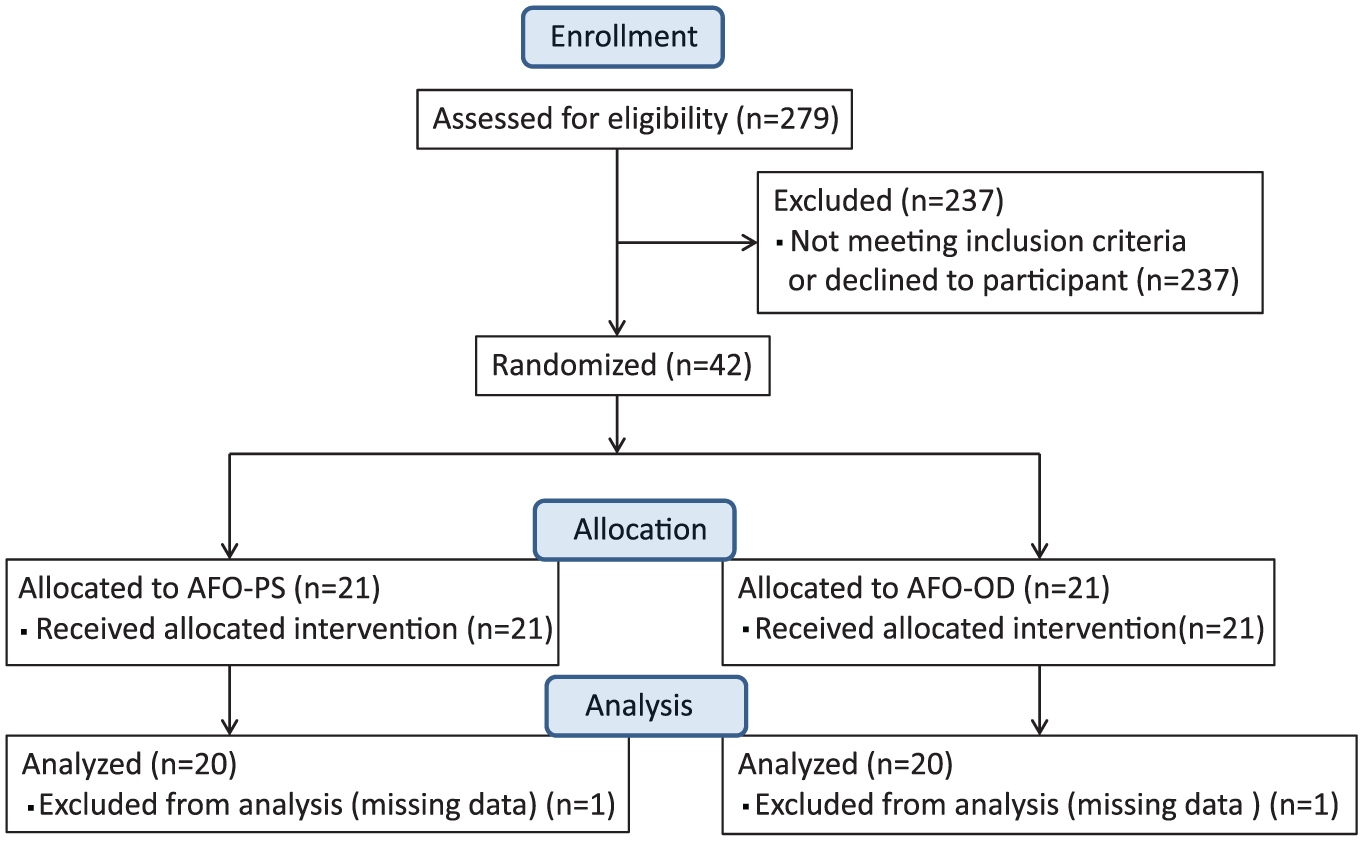
Consolidated Standard of Reporting Trials (CONSORT) flow chart.
Patient profiles.
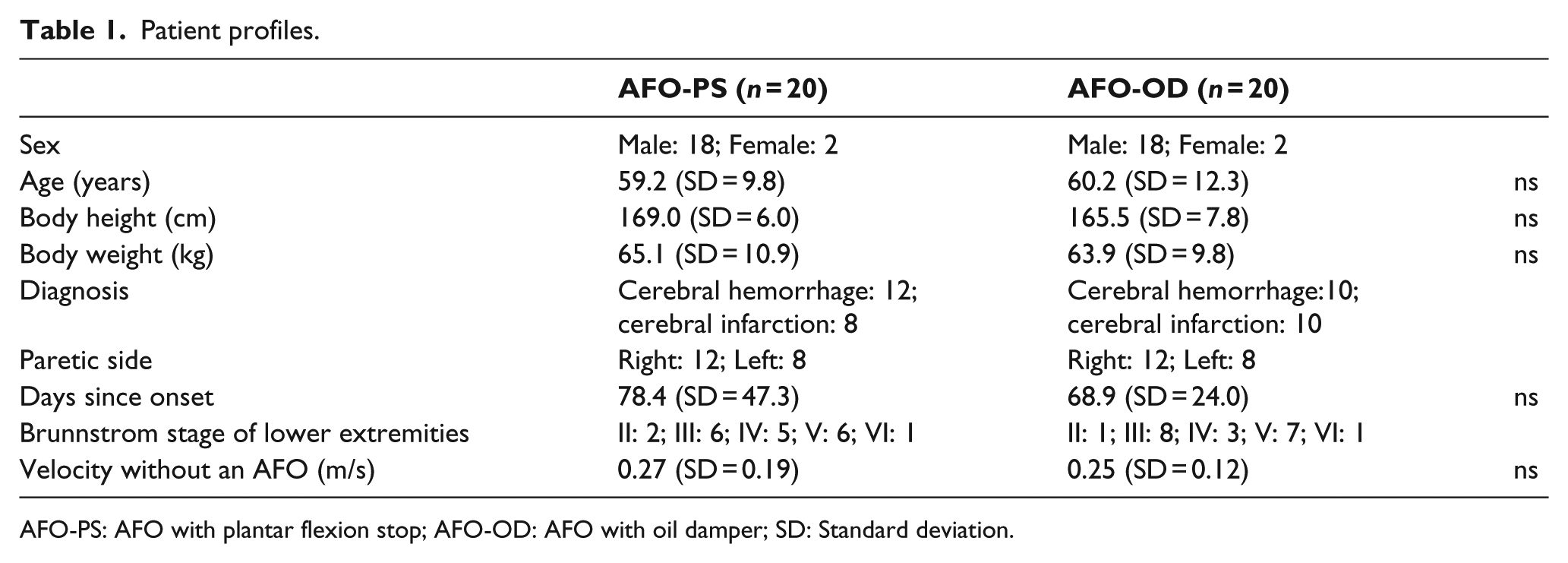
AFO-PS: AFO with plantar flexion stop; AFO-OD: AFO with oil damper; SD: Standard deviation.
The normality of all parameters, except the loading response time and center of pressure (COP) progression in single stance, was confirmed. Temporal and spatial factors, ground reaction forces, and COP progression results are shown in Table 2. Joint kinematics and kinetics are shown in Table 3, and pelvic and thoracic tilt angles are shown in Table 4. Data for lateral obliquity and rotation of the pelvis and thorax are not shown because there were neither interactions nor differences between conditions and groups.
Temporal and spatial factors and ground reaction forces.
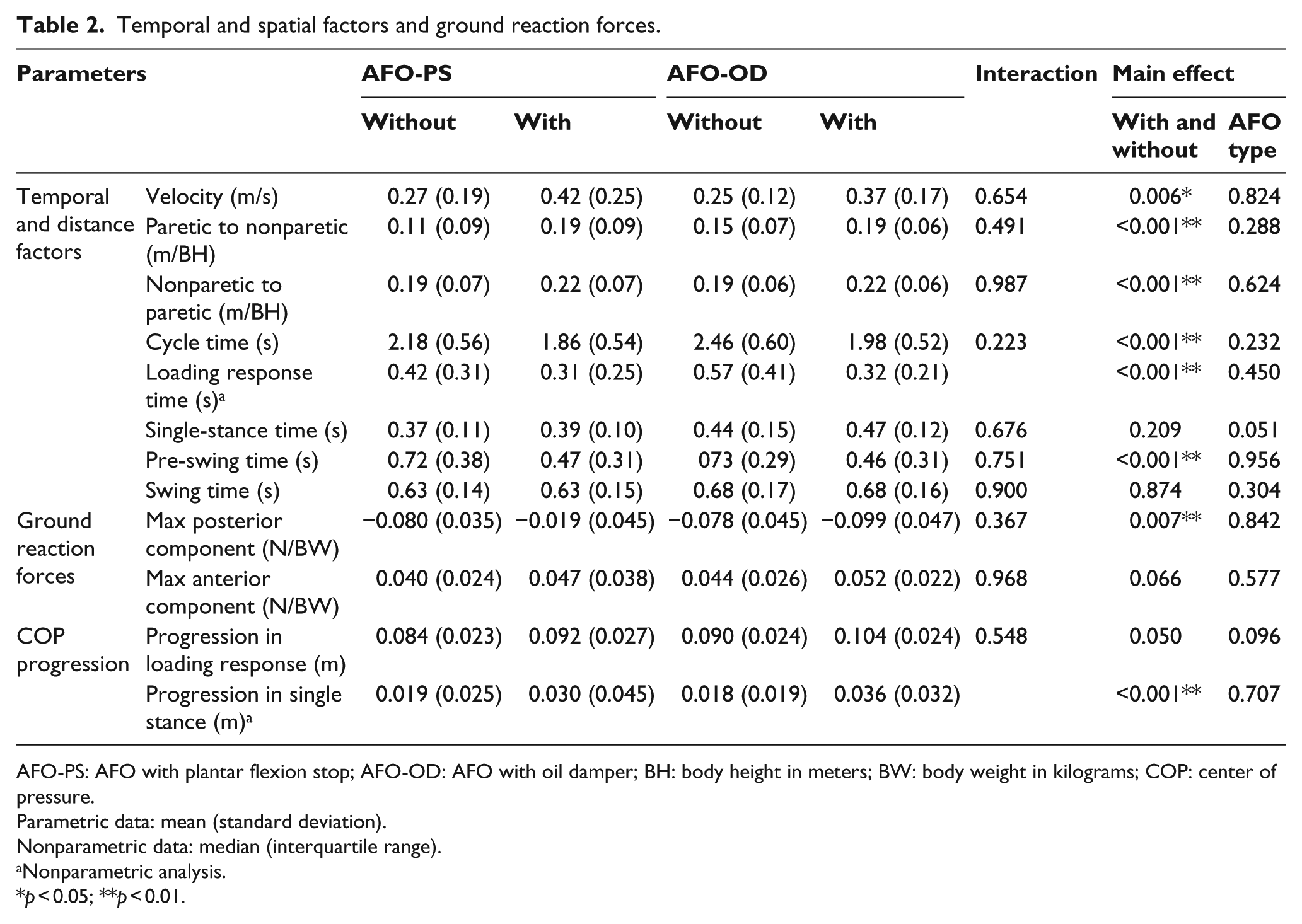
AFO-PS: AFO with plantar flexion stop; AFO-OD: AFO with oil damper; BH: body height in meters; BW: body weight in kilograms; COP: center of pressure.
Parametric data: mean (standard deviation).
Nonparametric data: median (interquartile range).
Nonparametric analysis.
p < 0.05; **p < 0.01.
Joint kinematics and kinetics.
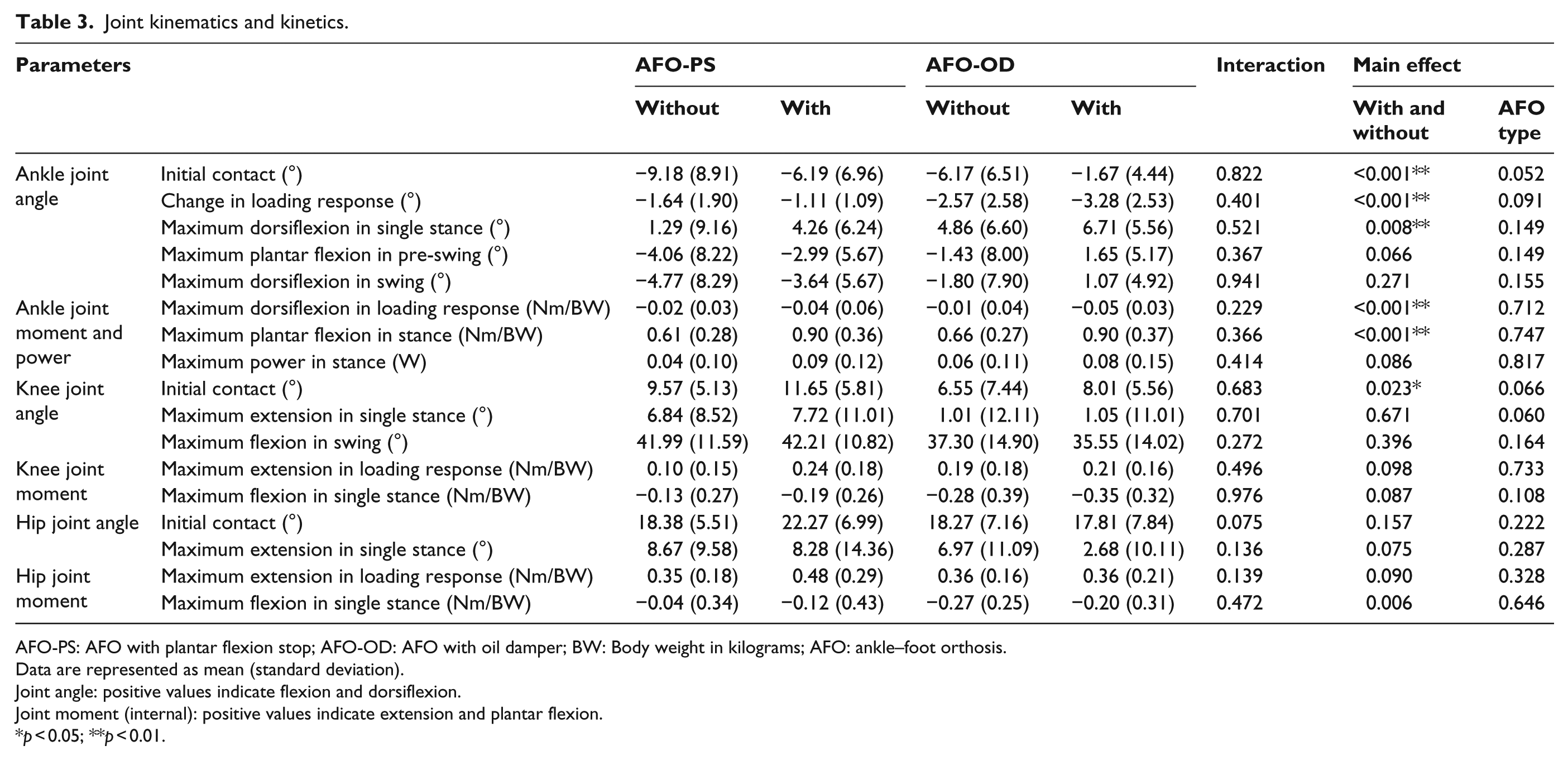
AFO-PS: AFO with plantar flexion stop; AFO-OD: AFO with oil damper; BW: Body weight in kilograms; AFO: ankle–foot orthosis.
Data are represented as mean (standard deviation).
Joint angle: positive values indicate flexion and dorsiflexion.
Joint moment (internal): positive values indicate extension and plantar flexion.
p < 0.05; **p < 0.01.
Pelvic and thoracic tilt angles.
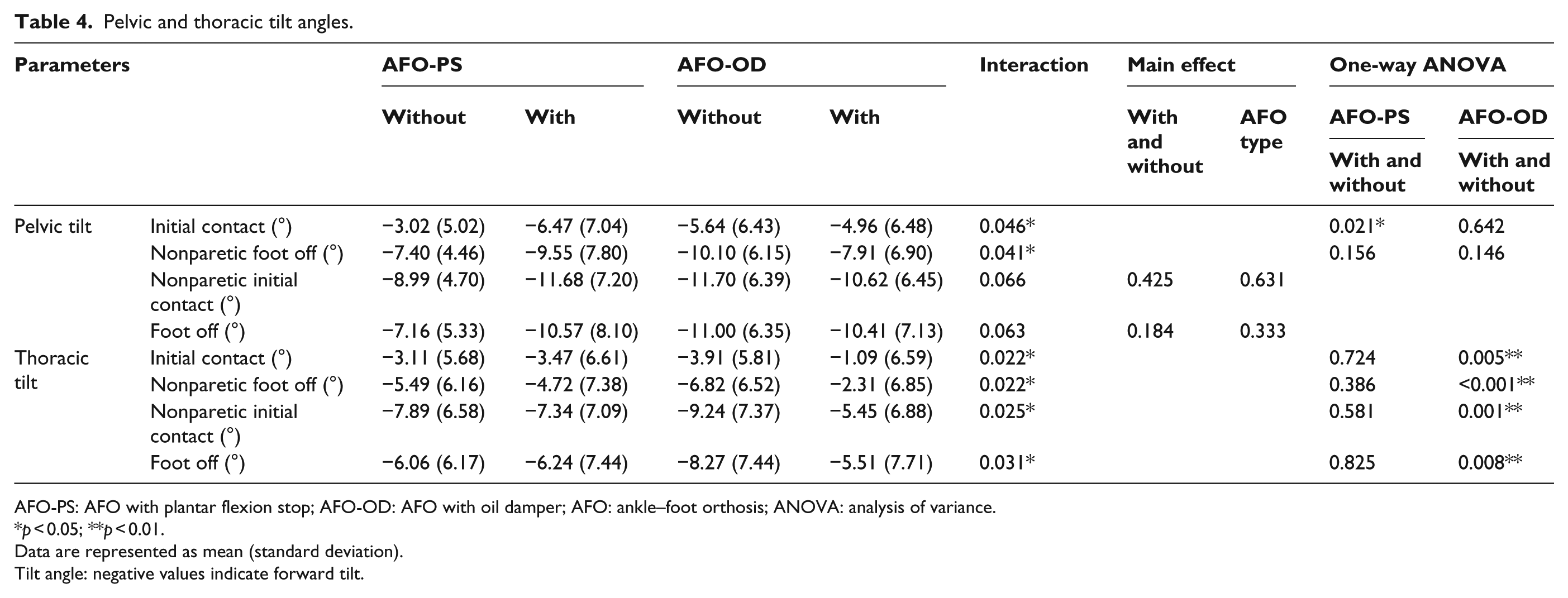
AFO-PS: AFO with plantar flexion stop; AFO-OD: AFO with oil damper; AFO: ankle–foot orthosis; ANOVA: analysis of variance.
p < 0.05; **p < 0.01.
Data are represented as mean (standard deviation).
Tilt angle: negative values indicate forward tilt.
As shown in Tables 2 and 3, no interaction was found in temporal and spatial factors, ground reaction forces, and joint kinematics and kinetics. A main effect that showed the difference between conditions, with and without an AFO, was found for many parameters. Regarding the temporal and spatial factors, the velocity, step lengths, posterior component of the ground reaction forces, and COP progression in single stance were increased in the gait with an AFO. Cycle time, loading response time, and pre-swing time were decreased in the gait with an AFO. In terms of ankle joint kinematics and kinetics, the dorsiflexion angle at initial contact, plantar flexion change in loading response, maximum dorsiflexion in single stance, maximum dorsiflexion moment in loading response, and maximum plantar flexion moment in stance were increased in the gait with an AFO. Knee joint flexion at initial contact was larger in the gait with an AFO. There was no significant difference between the AFO-PS and AFO-OD groups regarding these parameters.
Interactions were found in pelvic and thoracic tilt angles (Table 4). One-way ANOVA was performed for parameters, which showed the interaction to compare the conditions in each AFO group. In AFO-PS group, the forward inclination of the pelvis at initial contact was increased when the patients walked with the AFO compared with the shod gait without an AFO; no difference was found in the AFO-OD group. Concerning the thoracic tilt angle, the forward inclinations at initial contact, nonparetic foot off, nonparetic initial contact, and foot off were decreased when the patients walked with the AFO-OD compared with the shod gait without an AFO; no difference was found in the AFO-PS group.
Figure 3 shows the average and standard deviation of tilt angle of the pelvis for each group. The horizontal axis shows the percent gait cycle starting at initial contact of the paretic limb, and the vertical axis shows the tilt angle with forward tilt as negative. The waveforms are similar in shape, but forward tilt was increased when patients walked with the AFO-PS (Figure 3(a)). In the AFO-OD group, no difference was found between conditions (Figure 3(b)). Figure 4 shows the average thoracic tilt angle in the same way. Forward tilt was reduced throughout the gait cycle when patients walked with the AFO-OD (Figure 4(b)), but no difference was found between conditions in the AFO-PS group (Figure 4(a)).
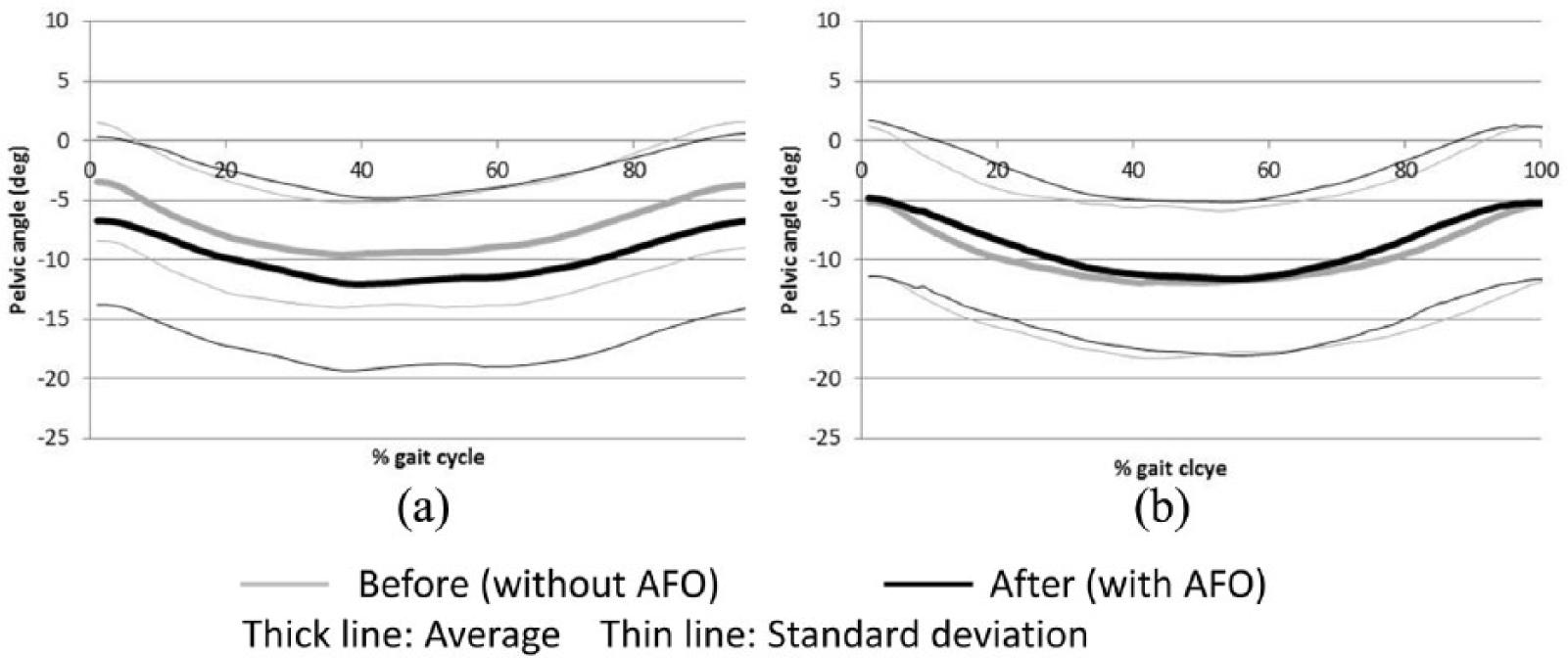
Average and standard deviation of pelvic tilt angles in one gait cycle Negative values indicate forward tilt: (a) AFO-PS and (b) AFO-OD.
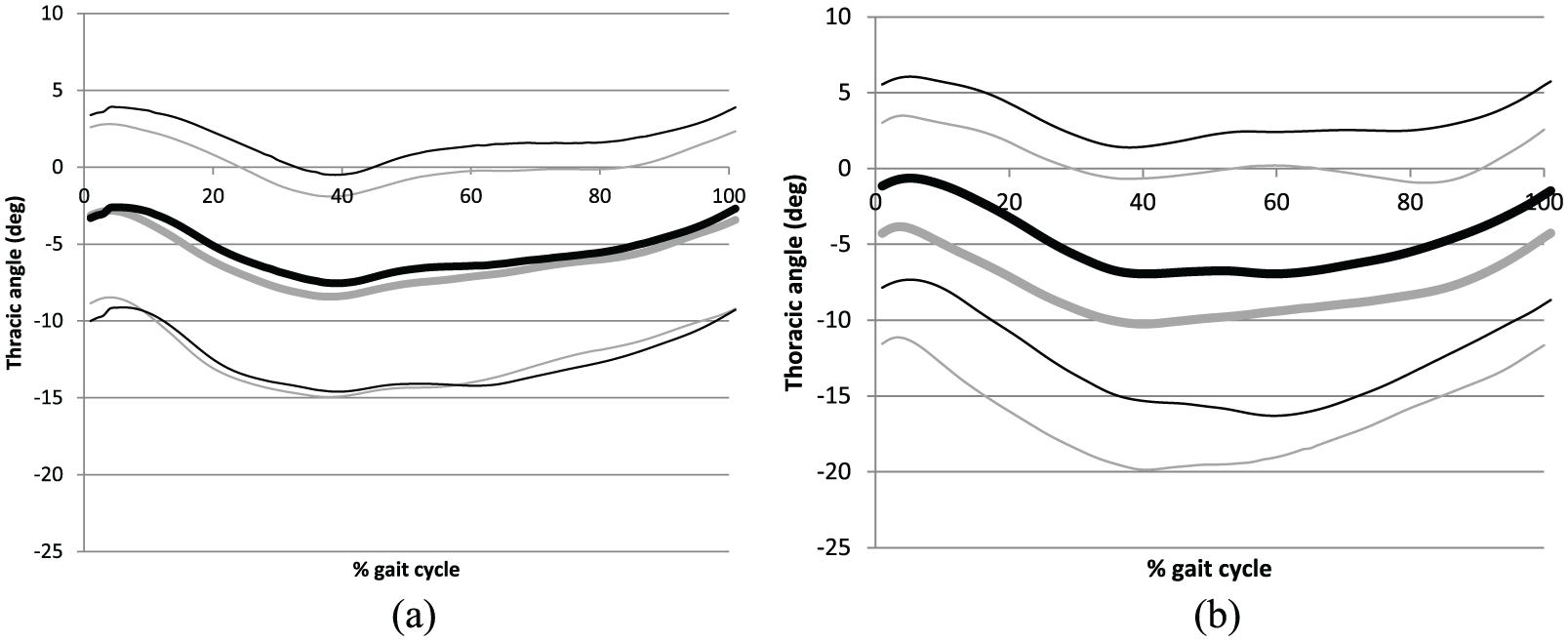
Average and standard deviation of thoracic tilt angles in one gait cycle Negative values indicate forward tilt: (a) AFO-PS and (b) AFO-OD.
In terms of the participants’ perception, many patients felt it was easier to walk with an AFO than without an AFO in both groups. Some patients in the AFO-PS group complained about hindrance to the ankle joint movement during gait; however, no patients in the AFO-OD group had such complaints.
Discussion
Many differences between gait with and without an AFO were observed within the two AFO groups (AFO-PS and AFO-OD). Because the subjects in this study were stroke patients in the subacute phase, these changes were caused by the patients’ recovery process, the effect of training, and the effect of the AFO. The increases in velocity, step length, COP progression, and ankle and knee joint angles and moments observed in this study were similar to those observed in previous studies comparing gait with and without an AFO.1–3
The focus of this study was to investigate the effect of AFO function on the ankle, knee, and hip joints during the gait of stroke patients in subacute phase. Our results showed no interaction between the two AFO groups in joint kinematics and kinetics. Although not significant (p = 0.075), hip flexion angle at initial contact was increased from 18.4° ± 5.5° without an AFO to 22.3° ± 7.0° with an AFO in the AFO-PS group, but it decreased from 18.3° ± 7.2° to 17.8° ± 7.8° in the AFO-OD group.
A previous study that compared the ankle joint angle between AFO-PS and AFO-OD groups showed that the ankle joint started dorsiflexion immediately after initial contact in the AFO-PS group. 23 However, the ankle joint gradually moved to plantar flexion in the AFO-OD group. Generally, increased dorsiflexion induces flexion of the knee and hip joints due to a kinematic chain. However, there were no significant differences between groups in parameters regarding the ankle, knee, and hip joints in this study. This could be attributed to the variety of patients’ gait patterns. In previous studies, the gait of patients in the subacute phase was categorized into certain patterns, such as extension thrust, buckling knee, and stiff knee.24,25 In these studies, the key parameter for categorization was knee joint movement. Another study on the effect of plantar flexion resistance of the AFO demonstrated that the subjects were limited to the stroke patients who showed genu recurvatum. 16 Conversely, gait pattern was not considered as inclusion criteria in our study, and so, significant differences were not easily detected in the ankle, knee, and hip joints.
Differences between the two AFO groups were found in the movement of the pelvis and thorax. Interactions were found in the tilt angles of these segments. In the AFO-PS group, the pelvis was inclined forward to a greater degree at initial contact compared with the shod gait without an AFO. In contrast, in the AFO-OD group, the thoracic tilt angle was reduced throughout the stance phase compared with the shod gait without an AFO. Although there were no significant differences in the lower extremities between the two AFO groups, the observed differences in the tilt angles of the pelvis and thorax may have been caused by different alignment during initial contact and loading response of the paretic limb. The AFO-PS induces flexed alignment of the lower limb as well as forward tilt of the pelvis. In contrast, the AFO with plantar flexion resistance promotes gradual movement to plantar flexion in loading response, assisted by the oil damper. This induces relatively extended alignment of the lower limb without causing forward tilt of the pelvis, resulting in an upright thoracic posture. The inclined posture of the pelvis and the thorax is a known feature of the gait of stroke patients. 26 Previous studies comparing gait with and without AFOs focused on ankle and knee joint kinematics and kinetics, 2 and few studies have investigated the effect of different kinds of AFOs on the pelvis. 27 The results of this study show that AFOs may have an indirect effect on alignment of the pelvis and thorax during the gait of stroke patients in the subacute phase. These findings suggest that the AFO with plantar flexion resistance facilitates better alignment of the upper body and pelvis. This type of AFO could be beneficial for patients who have malalignment of the upper body and pelvis during gait.
There are some limitations to this study. First, the duration of AFO use was 2 weeks in this study. Although this was necessary for ethical reasons, it did not provide sufficient time to show the full effects of AFO function. Second, as the data obtained in this study were measured at a rehabilitation center, the universality of the results has not been demonstrated. The patients in this study showed a variety of gait patterns. Finally, the participants were stroke patients in the subacute phase. Future studies should clarify whether similar results are obtained for stroke patients in the chronic phase.
Conclusion
The gait of 40 stroke patients in the subacute phase was measured before and after 2 weeks of gait training using either an AFO with plantar flexion stop or an AFO with plantar flexion resistance. Significant differences between the two AFO groups were found in tilt angles of the pelvis and thorax; compared with the shod gait without an AFO, the pelvis showed forward tilt when patients walked with an AFO with plantar flexion stop and the thorax showed reduced forward tilt when patients walked with an AFO with plantar flexion resistance. The plantar flexion resistance function of the AFO affected the alignment of the upper body and the pelvis during the gait of stroke patients in the subacute phase.
Footnotes
Acknowledgements
The authors thank the patients who participated in this study. The authors also thank the physiotherapists who performed the gait training and assisted with the gait measurement.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI Grant Number 26350630.