
Abstract
Background:
Studies suggest that the energy expenditure of healthy persons (control) during walking with the preferred walking speed in steady-state conditions is dominated by fat oxidation. Conversely, carbohydrate and fat oxidation during walking is little investigated in transfemoral amputees.
Objectives:
To investigate carbohydrate and fat oxidation, energy cost of walking, and percent utilization of maximal aerobic capacity
Study design:
Eight transfemoral amputees and controls walked with their preferred walking speed and speeds 12.5% and 25% slower and faster than their preferred walking speed.
Methods:
Energy expenditure and fuel utilization were measured using a portable metabolic analyzer. Metabolic values are means ± standard deviation.
Results:
For transfemoral amputees (37.0 ± 10.9 years) and controls (39.0 ± 12.3 years), fat utilization at the preferred walking speed was 44.8% ± 7.2% and 45.0% ± 7.2% of the total energy expenditure, respectively. The preferred walking speed of the transfemoral amputees and controls was close to a metabolic cross-over speed, which is the speed where carbohydrate utilization increases steeply and fat utilization decreases. When walking fast, at 90 m min−1 (preferred walking speed plus 25%), transfemoral amputees utilized 70.7% ± 5.6% of their
Conclusion:
At the preferred walking speed, carbohydrate, not fat, dominates energy expenditure of both transfemoral amputees and controls. For the transfemoral amputees, consequences of fast walking are very high
Clinical relevance
Research on the relationships between physical effort and fuel partitioning during ambulation could provide important insights for exercise-rehabilitation programs for lower limb amputees (LLA). Regular endurance exercise will improve maximal aerobic capacity and enable LLA to walk faster and at the same time expend less energy and improve fat utilization.
Background
Walking is the most common form of exercises and may for many people be the only break in an otherwise sedentary life.
1
Following a lower limb amputation and the resulting walking disability, persons often adopt a very sedentary lifestyle
2
which may, over time, further reduce aerobic power, physical fitness, and walking speed. During level walking, the rate of oxygen uptake relates to the walking speed
3
; hence, measurements of the rate of oxygen uptake
Moreover, there are very few studies on the relation between walking speed and fuel partitioning during prosthetic ambulation, but previous studies on healthy persons have demonstrated that fat is the preferred energy substrate when walking with the PWS. 12 The quantity of energy from carbohydrate (CHO) stores of the body is only 1% of that available in fat, 13 and the rate of CHO oxidation increases with increasing physical effort.14,15 Consequently, it is suggested that conservation of CHO energy reserves, rather than walking economy per se, governs the selection of a PWS, and that central nervous system (CNS) selects a PWS that is supported mainly by fat oxidation. 12 Except for one previous study, looking at fuel utilization at the PWS during treadmill walking, 16 data on CHO and fat oxidation during prosthetic walking are virtually absent from the literature.
Thus, there is a need to investigate how overground walking with different speeds affect CHO and fat oxidation rates and walking economy of persons with a unilateral transfemoral amputation (TFA) and healthy, age-, and sex-matched individuals.
The main hypotheses are that persons with a TFA have a higher rate of CHO oxidation at similar relative speeds compared to healthy persons. In addition, we hypothesize that differences in walking speeds will have little effect on the walking economy, but that the physical effort, quantified as percent utilization of the maximal oxygen uptake
Methods
Participants
Two groups of participants were recruited to this study. The participants of the TFA group were eight, non-smoking adults (50 % females) with unilateral TFA for other reasons than vascular diseases and no comorbidities. Causes of amputations were as follows: trauma (n = 1), cancer (n = 5), congenital (n = 1), and infection (n = 1). The TFA participants had in average (±standard deviation (SD)) used their prosthesis for 15.9 ± 13.9 (range: 3–39) years. Five persons had a microcontroller-assisted knee joint, while three persons used hydraulic-controlled knee joints, and all TFA participants used their prosthesis on a daily basis. The average weight of the prostheses was 3.80 ± 0.5 kg.
The participants in the control (CON) group were eight healthy, non-smoking adults (50% females) with no orthopedic problems and with similar weight, height, and age as the TFA. Exclusion criteria for both groups were use of medication that could affect heart rate or energy expenditure (i.e. beta-blockers and thyroid hormone replacements). Daily walking distance of both the TFA and CON was assessed by a self-report form, and inclusion criteria was that the participants were able to walk continuously for at least 500 m. Written informed consent was obtained from all subjects and the study was approved by the Regional Committees for Medical and Health Research Ethics in Norway.
Study design
The participants were instructed to avoid exercise and alcohol 24 h prior to testing and to abstain from coffee and tea on the day of testing. The TFA and CON reported to the laboratory in the morning, 2 h after eating a low-fat breakfast (bread, jam, sliced ham, juice, low-fat milk) and were subsequently instrumented for collection of expired air. During all walk trials, the
Gas exchange and energy expenditure measurements
The oxygen analyzer was calibrated for barometric pressure, and gas was calibrated with a reference gas mixture of 16% O2 and 4% CO2. The calibration was then verified with measurements of ambient air, according to the manufacturer’s instructions. In addition, a volume calibration was performed using a standardized 3-L syringe (Hans Rudolph, Shawnee, KS, USA).
VO2, VCO2, lung ventilation, heart rate, and RER values were continuously monitored during testing by telemetry in real time to verify steady-state conditions during walking trials. The RER is the ratio between the carbon dioxide production and the oxygen consumption, and all walking sessions were completed with RER values <1.0. CHO and fat oxidation was calculated by indirect calorimetry using standard methods.
20
Protein oxidation was assumed to be insignificant during these walking trials.
21
The energy cost of walking (ECW), that is, the oxygen consumption per unit distance (mL kg−1 m−1), was calculated by dividing the participants
Statistics
Independent t tests were used to compare the TFA and CON for physical characteristics. A two-way mixed analysis of variance (ANOVA) was used to test if oxygen uptake (
Results
Physical characteristics of the participants
The mean ± SD age, height, weight, and body mass index of the TFA and CON were 37.0 ± 10.9 and 39.0 ± 12.3 years, 175.5 ± 4.6 and 170.0 ± 7.4 cm, 73.6 ± 10.4 and 72.7 ± 14.2 kg, 23.8 ± 2.7 and 25.2 ± 3.3 kg/m2, respectively. The weight of the TFA is including their prosthesis. There were no statistical differences in physical characteristics between the two groups. The maximal aerobic capacities
Walking speed
All participants walked with their PWS and speeds 12.5% and 25% slower and faster than their respective PWS, thus all relative walking speeds were similar for the TFA and CON. In terms of actual walking speed in m min−1, mean PWS of the TFA and CON were 73.2 ± 11.1 and 91.3 ± 8.8 m min−1 (TFA vs CON; p < 0.001). The range of walking speeds from the slowest to the fastest walking speeds (PWS minus 25% to PWS plus 25%) was 54.8 ± 9.7 − 90.4 ± 13.2 and 69.0 ± 6.3 − 114.4 ± 10.9 m min−1 for the TFA and CON, respectively (TFA vs CON; all comparisons, p < 0.001). Actual walking speeds were monitored by the OptoGait system (described in the “Methods” section), and there was a close correlation between OptoGait measurements and the pre-determined (calculated) walking speeds. For the TFA group, correlation coefficients for the measured and calculated walking speeds of PWS minus 25% and 12.5%, the PWS, and the PWS plus 12.5% and 25% were as follows: 0.997 (p < 0.001), 0.992 (p < 0.001), 0.994 (p < 0.001), 0.997 (p < 0.001), and 0.998 (p < 0.001), respectively. For the CON group, the correlation coefficients for the same speeds were as follows: 0.984 (p < 0.001), 0.989 (p < 0.001), 0.985 (p < 0.001), 0.993 (p < 0.001), and 0.997 (p < 0.001), respectively.
Oxygen uptake
The oxygen uptake (mL min−1 kg−1) following walking with different speeds is shown in Table 1. There was no significant interaction between group*time F(4, 56) = 0.572, p = 0.684,
Oxygen uptake and percent utilization of
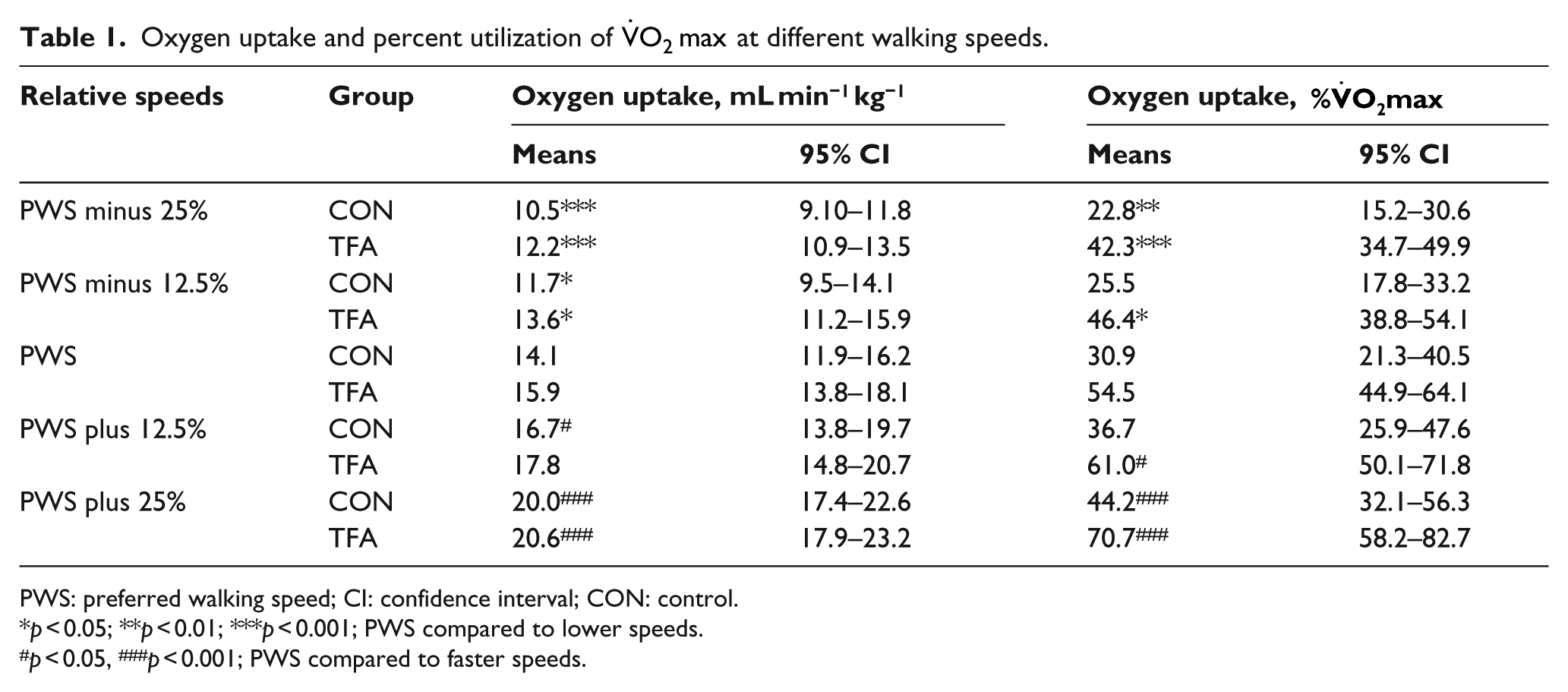
PWS: preferred walking speed; CI: confidence interval; CON: control.
p < 0.05; **p < 0.01; ***p < 0.001; PWS compared to lower speeds.
p < 0.05, ###p < 0.001; PWS compared to faster speeds.
Pairwise post hoc comparisons (for time) with Bonferroni corrections showed that for the TFA, the oxygen uptake at the PWS was significantly higher compared to PWS minus 25% (p < 0.001) and PWS minus 12.5% (p < 0.05) and lower compared to PWS plus 25% (p < 0.001). For the CON, the oxygen uptake at the PWS was significantly higher compared to PWS minus 25% (p < 0.001) and PWS minus 12.5% (p < 0.05) and lower compared to PWS plus 12.5% (p < 0.05) and PWS plus 25% (p < 0.001).
utilization
There was no significant interaction between group*time F(4, 56) = 1.406, p = 0.244,
Pairwise post hoc comparisons (for time) with Bonferroni corrections showed that for the TFA, the
ECW
There was no significant interaction between group*time F(4, 56) = 1.107, p = 0.362,
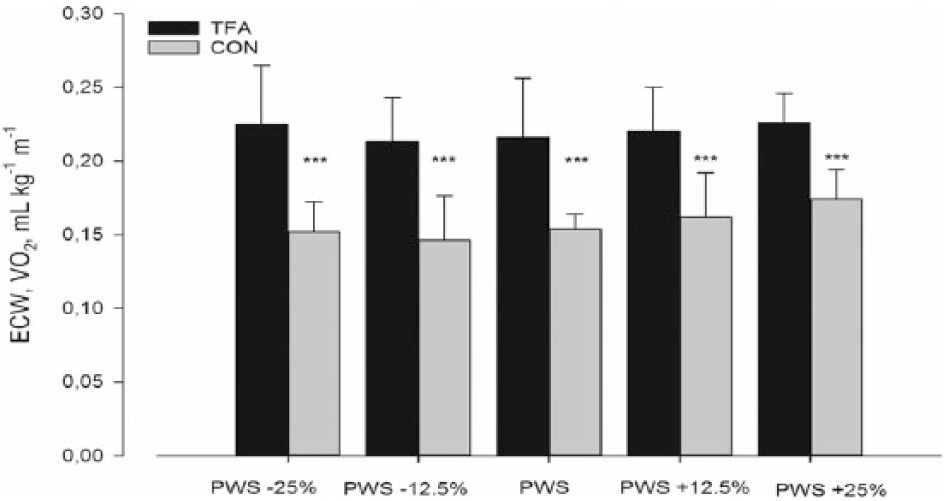
Energy cost of walking (ECW) of the TFA and CON during walking with similar relative speeds. Values are represented as mean ± SD. ***p < 0.001, TFA compared to CON.
Across the different walking speeds, the range of ECW values for the TFA and the CON were 0.213–0.226 and 0.146–0.174, respectively. Hence, since oxygen uptake and walking speed change more or less in parallel, the within-group ECW values show only small changes across the range of walking speeds. Pairwise post hoc comparisons with Bonferroni corrections showed that the ECW of the CON was significantly lower compared to the TFA at the all speeds (all comparisons, p < 0.001). For both the TFA and CON, the ECW at the PWS was similar to the ECW at the other walking speeds.
CHO and fat oxidation rates
For CHO, there was no significant interaction between group*time F(4, 56) = 0.576, p = 0.681,
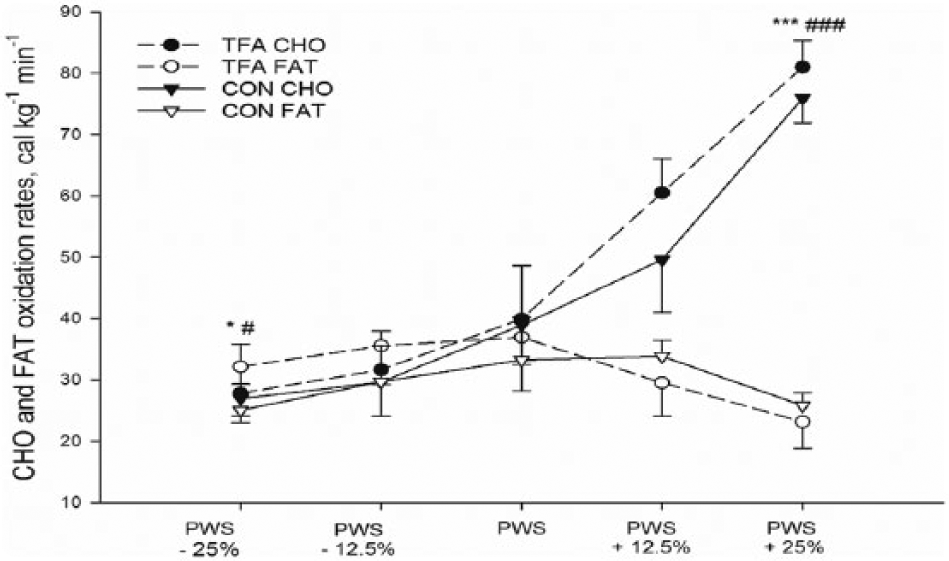
Fuel oxidation rates of the TFA and CON during walking on the floor with different speeds. Values are represented as mean ± SD. ***p < 0.001, CHO oxidation rates at the PWS of the TFA compared to other speeds. ###p < 0.001, CHO oxidation rates at the PWS of the CON compared to other speeds.
At similar relative walking speeds, the mean difference in CHO oxidation rates between the TFA and CON was small and varied between 1 and 10 cal kg−1 min−1. For both the TFA and CON, the CHO oxidation rates at the PWS was significantly higher compared to PWS minus 25% (both, p < 0.05) and lower compared to oxidation rates at PWS plus 25% (p < 0.001).
For fat, there was no significant interaction between group*time F(4, 56) = 0.858, p = 0.495,
At similar relative walking speeds, the fat oxidation rates of the TFA and CON were quite similar, and the mean difference in fat oxidation rates was in the order of 2–7 cal kg−1 min−1. Fat oxidation rates are shown in Figure 2.
Discussion
This study compared walking economy, percent utilization of the
Our results also show that CHO and fat oxidation rates are similar for the TFA and CON when walking with similar relative speeds in the fed state. Thus, in the fed state, there is little support for the hypothesis that the CNS naturally selects a walking speed that requires little or no net CHO depletion.
12
Generally, this study shows that in the fed state, the PWS of the TFA is a metabolic cross-over speed,
23
meaning that when the TFA walking speed exceeds the PWS, the CHO oxidation rates increases more steeply and there is a concomitant reduction in the fat oxidation rates (Figure 2). A similar response is seen for the CON, and at the same relative speeds, the curves are virtually overlapping with the TFA curves. However, at the PWS, the TFA and CON walk at an absolute speed of 73 and 91 m min−1; thus, the metabolic cross-over speed of the CON is at a higher absolute speed compared to the TFA. Furthermore, while the oxygen consumption at the PWS is similar (Table 1), the TFA utilized about 55 % of their
As can be observed in Figure 2, there is a great reliance on CHO oxidation during fast walking, and it is well established that endurance capacity and CHO availability are highly interrelated 24 ; hence, the size of the CHO stores in the body may be of special importance for persons with a lower limb amputation. Pertaining to this, persons with a TFA evidently have less lower extremity muscle mass than healthy persons and many are untrained and have low aerobic capacity.16,25 The CHO (glycogen) stores in skeletal muscles is limited by the quantity of muscle mass and the intrinsic glycogen storage capacity of muscle tissue (80–150 mmol kg−1 wet weight). 26 However, skeletal muscle of untrained individuals may store only 50% of the capacity of trained skeletal muscle.27–29 Thus, it is plausible that an untrained muscle mass and corresponding low intramuscular CHO stores may considerably limit the endurance capacity and walking range of persons with lower limb amputation.
Furthermore, it is important to note that the rates of fat oxidation in the study of Willis et al. 12 are higher than the fat oxidation rates in this study. In the above study, fat accounted for about 65% of the total energy expenditure during walking with the PWS, and in a similar study of persons with post-stroke hemiparesis, fat supplied 58% of the total energy expenditure when walking with the PWS. 30 In this study, fat utilization was about 45% of the total energy expenditure for TFA and CON when walking with the PWS; hence, fat combustion was substantially lower than in the studies of Willis et al. 12 and Ganley et al. 30
The reason for these discrepancies may be related to the fact that the participants in the above studies were tested following an overnight fast, and it is expected that fat oxidation rates are quite high following prolonged fasting (>6 h).
31
On the other hand, to investigate fuel oxidation during normal living, it is important to study the energy metabolism also in the non-fasted state, as in this study. The following example illustrates the impact of prior feeding on fuel partitioning. In Willis et al.’s
12
study, the total energy expenditure of healthy persons during treadmill walking with the treadmill PWS was 63 cal min−1 kg−1, and CHO and fat utilization accounted for 33% and 67% of the total energy expenditure, respectively. Oxygen uptake was 13.2 mL min−1 kg−1, and heart rate was 95 beats min−1. In a previous study in our lab,
32
using the same participants as in this study, we observed that during treadmill walking at the PWS, CON mean oxygen uptake, heart rate, and total energy expenditure were 13.4 mL min−1 kg−1, 92 beats min−1, and 68 cal min−1 kg−1, that is, similar to Willis et al.’s
12
study. However, CHO and fat oxidation rates were 64% and 36% of the total energy expenditure, respectively, and consequently, the fuel partitioning in the fed state (this study) was reversed with regard to the fasted state.
12
This is, however, not unexpected as feeding suppresses fat oxidation during physical activity.
31
Thus, to enable persons with a lower limb amputation to adopt a faster walking speed and at the same time to expend less energy, it is of importance that these persons perform aerobic endurance exercise. Regular endurance exercise will improve the maximal aerobic capacity
Conclusion
In the fed state, the PWS of both the TFA and CON is close to a metabolic cross-over walking speed, above which CHO oxidation rates increases steeply. Thus, when the TFA walking speed exceeds the PWS, there is an increasing reliance on CHO oxidation and a concomitant reduction in the fat oxidation rates. The relative oxygen uptake (VO2, mL min−1 kg−1) did not differ between groups across the range of walking speeds. Within each group, the ECW did not vary across walking speeds. In contrast, the
Possible limitations
The TFA in this study used different types of knee joints (hydraulic or microprocessor controlled) and one may speculate if this in any way could affect measures of ECW or oxygen uptake values. There is no indication in our data that differences in knee joint construction affect these measurements. Nonetheless, it may be prudent to conduct further studies on this matter with a larger number of participants to investigate the relation between walking speed and fuel selection during prosthetic walking.
Footnotes
Acknowledgements
The authors thank the participants for their patience and effort during the walking experiments.
Author contribution
All authors contributed equally in the preparation of this manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.