
Abstract
Background:
Epidermolysis bullosa dystrophica is a rare dermatological disease characterized by extreme skin fragility and elevated risk of developing a squamous cell carcinoma. In some cases, amputation of a limb is necessary.
Case description and methods:
A 37-year-old man with recessive, severe generalized epidermolysis bullosa dystrophica developed a squamous cell carcinoma on the right forearm requiring a below-elbow amputation. Preoperative advice concerning indication and level of amputation was given. Due to potential skin problems, a conventional prosthesis was not feasible.
Findings and outcomes:
A custom-designed adaptive prosthesis with an upper arm cuff was trialed and was well tolerated. Multiple working tools, attached with a rotation and inclination system, allowed independence and return to work.
Conclusion:
Despite multiple potential skin problems of the stump, the patient was successfully fitted with a custom-designed adaptive prosthesis. Preparation for this fitting was done by a comprehensive multidisciplinary patient-centered approach.
Clinical relevance
Despite severe skin fragility, a patient with epidermolysis bullosa dystrophica was successfully fitted with a custom-designed adaptive upper limb prosthesis allowing good functional outcome. This required a multidisciplinary and patient-centered approach.
Keywords
Background
Epidermolysis bullosa (EB) comprises a clinically and genetically heterogeneous group of rare congenital disorders characterized by marked mechanical fragility of the epithelial skin and mucosa with blistering and erosions, spontaneous or following minor trauma.
Epidemiologically, the most reliable data are derived from the National EB registry. 1 An incidence of 19 per million live births over a 5-year period, across the continental United States, was reported. 1
Based on the level of skin splicing, EB is divided into four major groups: epidermolysis bullosa simplex (EBS), junctional epidermolysis bullosa (JEB), Kindler syndrome, and dystrophic epidermolysis bullosa (DEB). 1
We describe the case of a patient with a severe generalized recessive form of DEB, who required forearm amputation and was fitted with a prosthesis.
To our best knowledge, only four cases of successful prosthetic fitting in persons with this type of dermatological background have been reported.2–5
The multidisciplinary approach with oncological and plastic surgeons, dermatologists, and the full rehabilitation team is of great value in the management of these patients.
Case description and methods
A 37-year-old man was the second child of nonrelated parents. At birth, multiple bullae filled with liquid were found all over his body. Eruptions of these bullae were associated with loss of skin. A diagnosis of epidermolysis bullosa dystrophica, severe generalized, was confirmed by immunofluorescent techniques. Recurrence of these wounds led to a significant atrophy and scarring of the entire skin.
At the age of 37, he already underwent five desyndactylization operations, five endoscopic esophagus dilatations, one restorative proctectomy with a coloanal anastomosis, and tooth extractions with substitution by a denture.
On 5 January 2015, he was diagnosed with a squamous cell carcinoma (SCC) on the right forearm (Figure 1). Initial therapy consisted of wide local resection and skin grafting. With an Integra® dressing, the extensive wound healed rather well, but new skin lesions with hypergranulation appeared at the border. New biopsies confirmed a multifocal SCC relapse. After discussion with the patient, an amputation was considered as a therapeutic option by the oncologic surgeons and the dermatologist. He was referred to the rehabilitation center for multidisciplinary preoperative advice concerning indication and level of amputation as well as to define rehabilitation goals and plan. The rehabilitation team was composed of a Physical and Rehabilitation Medicine (PRM) physician, an occupational therapist, a physiotherapist, and a prosthetist.

Squamous cell carcinoma of the right forearm.
The clinical examination showed wound dressings over the entire body from neck to toes. Mitten deformities were seen on both hands and feet, with total absence of nails. On the left hand, the patient had two fingertips, and on the right hand, only the thumb remained. Shoulder range of motion (ROM) was limited to 120° in flexion and abduction, elbow ROM to 100°. ROM of the wrist was absent on both sides due to contractures in a 60° flexed, ulnar-deviated position. No deficits in strength of the shoulders and elbows were noticed.
Functional assessment at intake showed need of assistance for daily wound care, which was performed by his father. Daily wound care consists of piercing the blisters, covering the wounds with zinc oxide paste and compresses, as well as for larger wounds with silicone foam dressings and alginogels. 6 Food and drinks are consumed independently, but meat has to be cut by the father.
The patient is working full time in informatics and he performs voluntary work for the Dystrophic Epidermolysis Bullosa Research Association (DEBRA) foundation. He is independent for transport. He drives his personal adapted car equipped with an automatic transmission system and Velcros on the handlebars. Psychologically, the man has an ultra-positive spirit and pragmatic attitude as well as very good cognitive abilities.
The patient was referred to the rehabilitation center for advise concerning treatment options and rehabilitation, more specifically following an eventual amputation. The biggest concern of the patient was that he could lose his already limited functionality. At that point, he was firm in stating that quality of life was more important to him than quantity, but if functional recovery with a prosthesis may be a perspective, he would consider amputation. Based on his medical record, his clinical and functional state, it was decided that an adaptive forearm prosthesis with adjustments for his skin frailty could preserve his current state of functionality. But clearly no guarantees for success could be given because of the extreme skin frailty. So the surgery recommendation consisted of a preference for a below-elbow amputation. This was discussed with the dermatologist, the oncologic surgeons, and the patient, and the decision for an amputation was taken after gaining informed consent of the patient.
An amputation was performed on 3 June 2015. After 27 days, he consulted the rehabilitation center. The right upper extremity presented a below-elbow stump, with a good healing and intact suture line, and a preserved ROM at elbow and shoulder levels. The skin was protected by non-adhering bandages. The prosthesis design consisted of a normal socket, adjusted with an upper elbow cuff for distributing local pressure, provided with Velcro closures to secure. No liner, pin lock system of vacuum with sleeve system was used because of the extreme skin frailty and regular need for extensive wound dressing. In dialogue with the patient, two working tools have initially been designed: one for switching the gearshift of his car, typing on his computer, and unzipping his trousers and another for computer use. They were attached through a clicking system.
Findings and outcomes
At 3-month follow-up, the patient complained about the weight of the working tools. In shared decision with the patient, a switch to a modified, lighter, working hook seemed a better option (Figure 2).
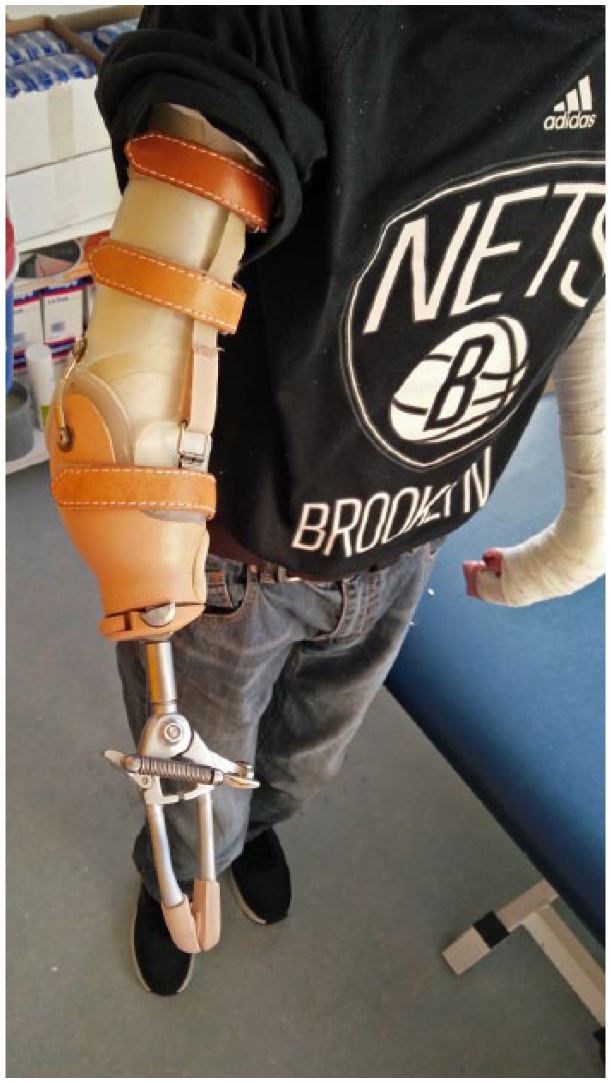
Final prosthesis design.
At 18-month follow-up, the patient experienced a good tolerance of the prosthesis. No extra wound problems were mentioned compared to the left side. Unfortunately, he did not become independent in donning and doffing the prosthesis, but was able to fulfill his proposed goals and is still working as an informatician. A fatigue feeling of the shoulder after a busy day at work was reported. Therefore, he reduced his working time from 5 to 4 days per week. The voluntary work remained at the same level.
Discussion
DEB is one of the subtypes of EB. Its phenotypical presentation is caused by different mutations in the gene for collagen VII. Polymers of collagen VII are fibrils which anchor the lower part of the epidermal basement membrane with the dermis. 7 The spectrum of mutations generates a continuum of biological phenotypes, explaining the varying clinical severity in DEB. In the present case, the patient suffers from the severe generalized recessive form, one of the harshest subtypes.
Blistering, extreme fragility, and wound formation are the clinical signs. Wound healing occurs with atrophy and scarring of the skin and mucous membranes. The most characteristic sign is the disproportionate scarring of the hands and feet, leading to mitten deformities. Contractures due to scarring are often seen. Current therapy consists of intensive daily wound care, general care including restoration of deficiencies and minimization of external harming factors.6,8 Systemic therapy is generally not required. However, anti-histaminic therapy can be indicated to reduce the itch.
SCC is an atypical proliferation of spinous cells of the skin. A high correlation is seen with recessive dystrophic epidermolysis bullosa (RDEB).9,10 Analysis over a 20-year period in the United States showed a cumulative risk of developing SCC of 90% at age 55. 9 Unlike SCC in general population, where these tumors develop on sun-exposed sites, EB-associated SCC is more often seen at places of chronic scarring and wounds.9,10
A biopsy for histological evaluation is necessary to assess the diagnosis of SCC. 10 Computed tomography (CT), magnetic resonance imaging (MRI), and the more performant FDG-positron emission tomography (PET) scans are used for staging. 10
SCC treatment is function of the stage of disease and the patient’s general condition. In general, tumor excision with wide surgical margins is the first-line treatment.
In case of adjacent tendons or soft tissue involvement, with or without local lymphatic tumor spread, or tumor recurrence, amputation may be the only therapeutic option. 10
For the design of the prosthesis, a vacuum-assisted or pin lock system was not considered due to extreme skin frailty of the stump (Figure 3). A maximal distribution of pressure from the prosthesis arm interface was a main purpose. Therefore, an upper elbow cuff was used, composed of light and flexible thermoplastic polyethylene. It was attached to the socket with flexible hinges and was designed with Velcro attachments to secure and adapt for daily variance in bandage thickness.

Post-operative stump.
Due to the daily bandages with variable volume, a too high risk of transpiration, and moistening of the skin with a liner, we have chosen not to use a liner. Also, the local pressure and shear of a liner could give skin problems in this type of dermatological diseases. As the patient would not have been able to put on the liner himself, it would again have increased dependence. During follow-up, good skin tolerance with this design was noticed.
An inclination and rotation system provided to switch working tools was adapted to the needs of the patient. A gear shift-working tool, also providing the possibility to type, was experienced as too heavy by the patient. A working hook was lighter and retained the same functionality (Figure 2).
In the present case, in shared decision making between team and patient, it was possible to achieve a fair functional outcome with prosthetic fitting in a patient with epidermolysis bullosa dystrophica, severe generalized. Because of the important implications for the patient’s life, a multidisciplinary, patient-centered approach was crucial for counseling in the preoperative phase and for designing the prosthesis in the post-operative phase. At 3-month follow-up, he was able to fulfill his driving goal and had already limited typing skills. The working tools were fine-tuned for weight and comfort in the follow-up period. Initially, he started with two working tools, but in the follow-up period, a modified working hook seemed better tolerated (Figure 2). During his follow-up period, no wound problems were mentioned due to the prosthesis. However, because of the rigidity of the prosthesis, he is not yet able to reach the same functional level as before the amputation.
Conclusion
A multidisciplinary approach was able to successfully fit a modified forearm prosthesis in a patient with below-elbow amputation due to a SCC caused by epidermolysis bullosa dystrophica, severe generalized.
The multidisciplinary approach consisted of giving realistic prognosis for accomplishing functional goals with a prosthesis preoperatively and to discuss the design of the prosthesis post-operatively in the second place.
This prosthetic design was based on the patient’s goals and adjusted for his skin fragility.
The adapted prosthesis allowed fair preservation of functionality and independence of the patient. Although in this case the patient tolerated the prosthesis well, each case will still be a process of trial and error.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.