
Abstract
Background:
Older adults with amputations secondary to vascular etiologies may additionally present with cognitive impairment. Cognition plays an important role in the adoption of a prosthetic limb, although the degree and type of impact are debated. Previous literature reviews have not been directed at the specific population of older adults who underwent vascular-related lower limb amputation.
Objectives:
First, to assess extant literature for relationships between cognitive function and prosthesis-related outcomes in older adults who underwent lower limb amputation for vascular-related etiologies. Second, to perform a critical analysis of prosthesis-related outcomes and cognitive assessments performed in the studies.
Study design:
Systematic literature review.
Methods:
A systematic review of the literature was performed in databases using keyword combinations. A total of nine articles were selected to be included in this review.
Results:
Seven of the nine included studies found a relationship between decreased cognitive function and reduced performance on a prosthesis-related outcome. There were eight different prosthesis-related outcome measures, with only one study utilizing a comprehensive outcome measure.
Conclusion:
Cognitive impairment can negatively impact successful prosthesis use in older adults with lower limb amputation secondary to vascular complications. Future studies should utilize comprehensive outcome measures that represent the multifaceted constructs of cognition and prosthesis use.
Clinical relevance
Cognitive assessment of older adults who have undergone lower limb amputation secondary to diabetes related complications or vascular disease can be used to inform clinical decision-making. Clinicians should consider selecting prosthesis-related outcome measures that capture the full breadth of prosthesis use when evaluating patients with cognitive impairment.
Background
The greatest incidence of non-traumatic amputation occurs in older adults secondary to complications related to vascular etiologies, including complications from diabetes, arterial/venous insufficiency, and peripheral vascular disease.1,2 It is predicted that the aging US population will yield an increased number of amputations due to vascular complications from less than 1 million in 2005 to a projected 2.3 million by the year 2050. 3 Following the amputation, eligible individuals may undergo the rehabilitation process to achieve a stable residual limb capable of supporting a prosthesis that can be used in activities of daily living. Due to the nature of vascular disease, the post-amputation rehabilitation process can be complicated by a common comorbidity: cognitive impairment.4–6 Compared to younger adults, healthy older adults demonstrate a higher incidence of cognitive impairment, and when coupled with vascular disease, an even greater incidence is observed.7,8 Successfully adopting a prosthetic limb requires that individuals be able to both physically perform functional movements and problem solve sequencing issues regarding their prosthetic fit and self-management of their residual limb. 9 Severe sequencing deficits can require a higher degree of personal care and support. 10 Therefore, it is imperative that the cognitive abilities of the individual undergoing amputation be understood, as they can inform decisions regarding prosthetic prescription.
Several literature reviews have examined the relationship between cognition and function following an amputation. O’Neill 11 reviewed whether cognition, among other predictors, had a predictive outcome in the rehabilitation process of lower limb amputees as defined by a graded mobility scale, disability, or prosthesis use. The review was not exclusive to any age group or etiology. The findings indicated that in the majority of studies reviewed, cognitive function did have a predictive relationship for a number of different mobility and prosthesis-related outcomes. Coffey et al. 12 performed a review evaluating the relationship between cognition and outcome following amputation, among other purposes. This review included both prosthesis users and non-prosthesis users, as well as all outcomes following amputation. Findings indicated a prognostic link between cognition and a variety of outcomes, particularly that deficits in the areas of memory and executive function are predictive of greater functional limitations over time.
While these reviews demonstrate an apparent relationship between cognition and function following an amputation, neither focused completely on older adults who underwent a lower limb amputation (LLA) for reasons directly related to vascular etiologies. Furthermore, while these previous reviews examine a number of different outcomes, not all were specific to the nature of the prosthesis user. Recovery following an amputation is multifaceted and comprised numerous constructs: functional mobility, psychological adjustment, self-management, societal participation, and quality of life. 13 Some individuals will go on to use a prosthetic limb, while others may not. For those who go on to use a prosthesis, there are numerous measures that can be used to assess their level of recovery. Some measures are limited to ambulation,14–16 while others may focus more on the psychosocial aspect of life following an amputation. 17 Other measures are more comprehensive and have the ability to measure the spectrum of factors influencing life with a prosthesis.18,19 It is the varied nature of these prosthesis-related outcome measures that can obfuscate true recovery in older adult amputees, for a single-facet assessment does not consider the multivariate nature of prosthesis use. 20 Cognitive function is itself multivariate in nature, with multiple subdomains comprising the overall construct, including memory, attention, decision-making, problem-solving, and language. 21 Any or all of these cognitive subdomains may differentially affect success rates in prosthesis use. Therefore, any assessment of how cognition affects prosthesis use should take into consideration the variety and quality of cognitive measures available.
Accordingly the purpose of this review is twofold: (1) to review and synthesize the current literature regarding cognitive abilities and prosthesis-related outcomes in older adults who underwent LLA secondary to vascular etiologies and (2) to critically analyze the prosthesis-related outcome measures and the cognitive-related assessments represented in the included body of the literature.
Methods
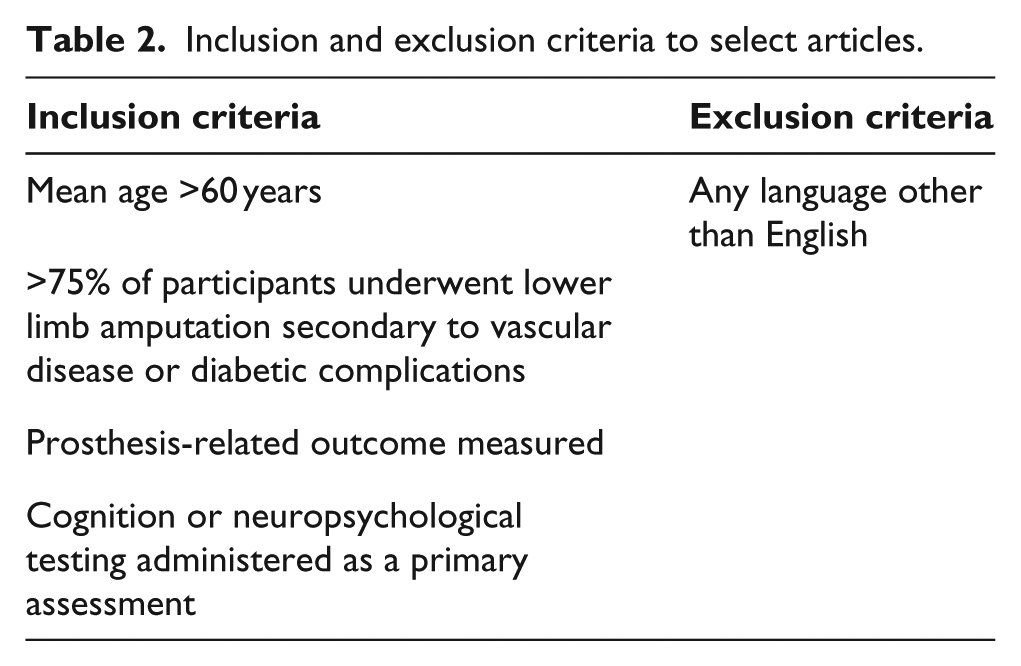
The literature review was performed by the authors in March of 2016. A combination of population, cognition, and prosthesis-related outcome keywords were searched in the following databases: CINAHL, PubMed, PsycINFO, Cochrane Library, and Web of Science. Search keywords used are presented in Table 1, and the inclusion and exclusion criteria are presented in Table 2. Due to the narrow scope of the search field, exclusion criteria were minimized to allow for a broader result pool. Articles included in the study were downloaded to citation management software and all duplicates were removed. A standardized evaluation form was created to guide the review process based on the inclusion/exclusion criteria. The authors independently evaluated the article abstracts for inclusion using the form and utilized the consensus method to manage any discrepancies in scoring. Full-text articles were then obtained based on the agreement of the authors and were evaluated for inclusion in the review. References from select articles were searched for additional citations of interest to the review and evaluated as above. The quality of each included study was evaluated using the UK National Framework for Long-term Conditions. 22 The framework is appropriate for evaluating non-randomized control trials and has been utilized in another review of a lower limb loss population. 23 The authors independently reviewed the quality of each included article and assigned it a grade of high, medium, or poor based on the scoring rubric.
Search keywords.

Inclusion and exclusion criteria to select articles.
Results
Following the selection and evaluation process, a total of nine articles were included in the review. A modified Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement is presented in figure 1. An overview of the included articles is presented in Table 3. The results presented below will only focus on cognitive/neuropsychological tests and outcomes directly related to prosthesis use. Sections are organized by the prosthesis-related outcome measure.
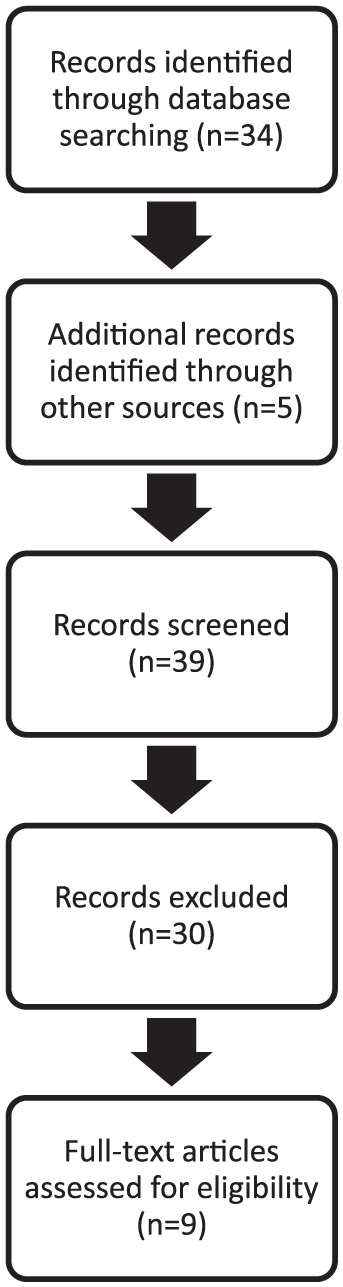
Procedure for article selection using a modified PRISMA format.
Overview of studies included in the literature review based on meeting necessary inclusionary criteria.
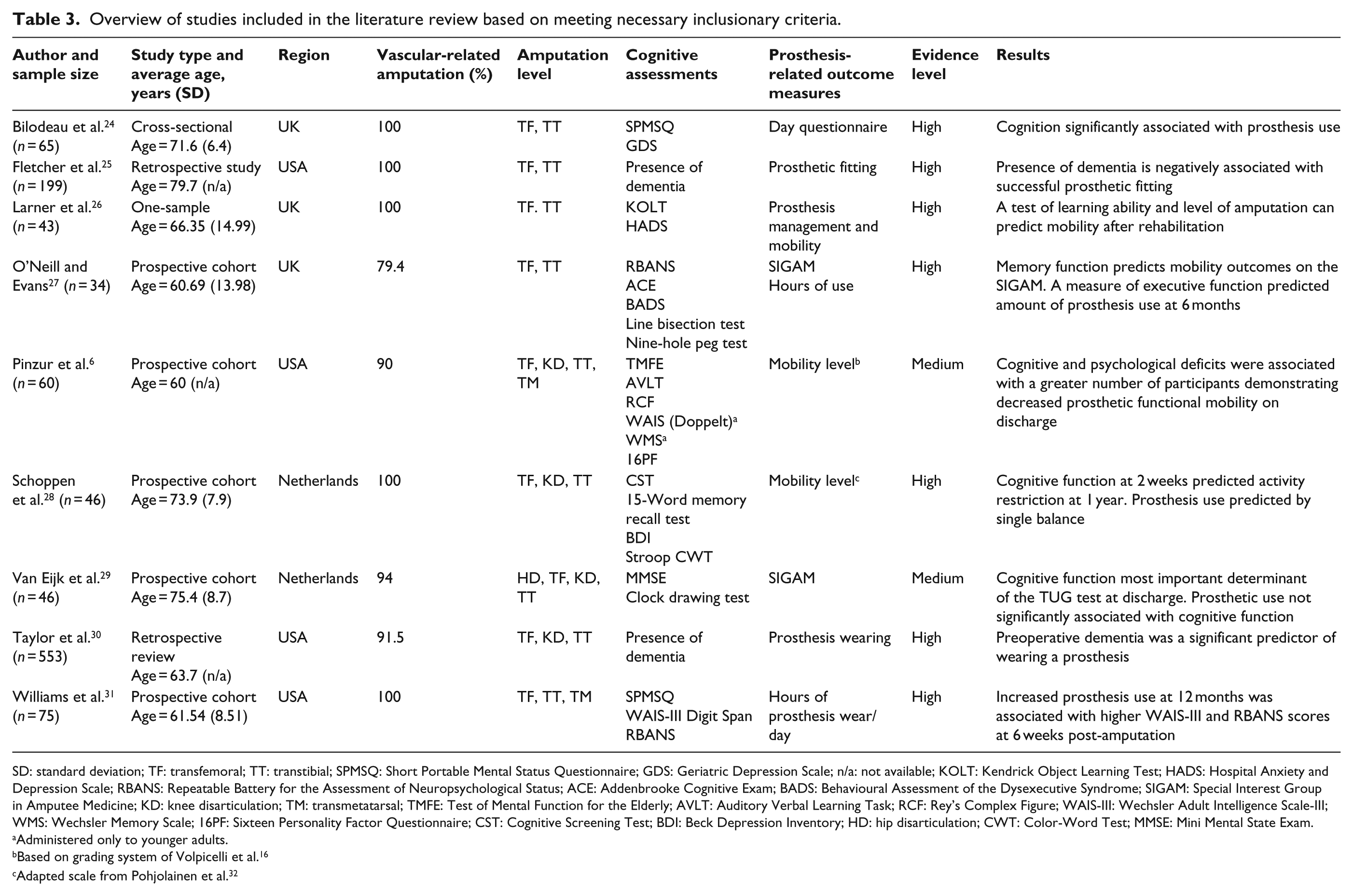
SD: standard deviation; TF: transfemoral; TT: transtibial; SPMSQ: Short Portable Mental Status Questionnaire; GDS: Geriatric Depression Scale; n/a: not available; KOLT: Kendrick Object Learning Test; HADS: Hospital Anxiety and Depression Scale; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; ACE: Addenbrooke Cognitive Exam; BADS: Behavioural Assessment of the Dysexecutive Syndrome; SIGAM: Special Interest Group in Amputee Medicine; KD: knee disarticulation; TM: transmetatarsal; TMFE: Test of Mental Function for the Elderly; AVLT: Auditory Verbal Learning Task; RCF: Rey’s Complex Figure; WAIS-III: Wechsler Adult Intelligence Scale-III; WMS: Wechsler Memory Scale; 16PF: Sixteen Personality Factor Questionnaire; CST: Cognitive Screening Test; BDI: Beck Depression Inventory; HD: hip disarticulation; CWT: Color-Word Test; MMSE: Mini Mental State Exam.
Administered only to younger adults.
Based on grading system of Volpicelli et al. 16
Adapted scale from Pohjolainen et al. 32
Functional mobility
Several studies have indicated that cognitive ability is linked to functional mobility outcomes. Schoppen et al. 28 assessed physical function, cognitive abilities, memory, information processing, and concentration to see whether these functions had a predictive value on prosthesis use at 1 year post LLA. The average age of the participants was 73.9 years, and the etiology of amputation was 100% vascular-related. Prosthesis use was measured using an 8-point scale adapted from the previously established scale by Pohjolainen and Alaranta. 32 The scale considers ambulatory level, wheelchair use, the ability to ambulate indoors versus outdoors, and the necessity of assistive devices during gait. At the 1-year assessment, functional prosthesis use was reached by 49% of participants. Two weeks after amputation, single-leg balance significantly correlated with prosthesis use at 1 year. However, cognitive function demonstrated a predictive capacity for activity restriction as based on the Groningen Activity Restriction Scale (GARS). 33
Van Eijk et al. 29 assessed baseline orientation, attention, memory, language, constructive abilities, verbal understanding, and spatially coded knowledge using the Mini Mental State Exam (MMSE) and clock drawing test. The average age of the participants was 75.4 years and 94% had an amputation due to vascular-related complications. Prosthesis use was assessed with the Special Interest Group in Amputee Medicine (SIGAM), 14 which measures mobility using a 6-point grading scale at the time of discharge from inpatient rehabilitation. At discharge, 50% of participants were fit for a prosthesis. The results demonstrated no significant relationship between cognition and prosthesis use, but did find a significant relationship between cognition and discharge timed-up-and-go (TUG) test scores. The higher the level of cognitive impairment, the greater the time it took to complete the TUG, indicating a less desirable performance.
Pinzur et al. 6 assessed upon admission participant attention, concentration, memory, organizational skills, and perceptual skills to examine the relationship with successful prosthesis mobility following discharge from inpatient rehabilitation. The average age of the participants was 60 years and 90% had an amputation due to vascular-related complications. Mobility was graded using a 7-point scale based on the grading system introduced by Volpicelli et al. 16 This scale rates participants based on their ability to walk in the home with or without supervision, in a limited or unlimited capacity, and whether they could ambulate in the community or not. Findings demonstrated that subjects without cognitive or psychiatric deficits were able to meet or stay within one mobility grade, per the 7-point Volpicelli scale, following amputation. In comparison, some of those with deficits demonstrated declines greater than one level in mobility and had a lower percentage of those meeting their previous mobility level.
Wearing time
Two studies have indicated that higher cognitive function is associated with increased wearing times. Williams et al. 31 assessed a battery of cognitive functions: orientation, basic awareness of current information, auditory-verbal memory, attention/working memory, ability to initiate problem-solving behaviors, cognitive flexibility, response inhibition, and executive function. The average age of the participants was 61.5 years and 100% had an amputation due to vascular complications. Assessments were performed at 6 weeks and 4 months following amputation, and the relationship with prosthesis wearing time at 1 year was one of the outcomes of interest. At the 1-year follow-up, 92% of participants had been fitted for a prosthesis. Higher scores at 6 weeks on attention/working memory (Wechsler Adult Intelligence Scale-III (WAIS): 34 Digit Span) and auditory-verbal memory tests (Repeated Battery for the Assessment of Neuropsychological Status (RBANS) 35 List recall) were associated with increased wear of the prosthesis at 1 year. Specifically, an increase in the z-score by 1 standard deviation (SD) on either test was associated with approximately an increase in wear by 2 h per day.
Taylor et al. 30 defined prosthesis wear as donning the prosthetic limb for at least 1 h a day. The authors performed a retrospective chart review, and the cognitive outcome of interest was the presence of dementia in the participant’s medical record. 30 The average age of the participants was 63.7 years, and 91.5% had an amputation due to vascular complications. A finding of preoperative dementia was a significant predictor of wearing a prosthesis, indicating that the presence of dementia was negatively correlated with being fit for a prosthesis.
Prosthesis fitting
One study found a relationship between being fit for a prosthesis and cognitive function. Fletcher et al. 25 performed a retrospective chart review to see whether the presence of cognitive dysfunction was associated with prosthesis fitting. The average age of the participants was 79.7 years, and 100% had an amputation due to vascular complications. For this study, successful prosthesis fit was determined if the participant was discharged from rehabilitation with a definitive prosthesis. About 36% of all participants were fit for a prosthesis successfully. The presence of dementia was negatively associated with prosthesis fitting, indicating that those having the diagnosis would be unlikely to be fit for a prosthetic limb.
Combined measures
Three studies had outcome measures that were multifaceted in nature. Larner et al. 26 defined prosthesis use as the participant’s ability to don/doff the prosthesis independently as well as that they could walk indoors modified independently with an assistive device. The average age of the participants was 66.4 years, and 100% had an amputation due to vascular complications. The cognitive measure used to assess learning ability was the Kendrick Object Learning Test (KOLT). At admission to the rehabilitation unit, the KOLT was administered, and then prosthesis use was evaluated upon discharge. The predictive power for the final statistical model was 81% using the KOLT score and the level of amputation.
O’Neill and Evans 27 assessed memory, executive function, and visuospatial ability at approximately 5 weeks post-amputation to see whether it predicted hours of prosthesis wearing and mobility (SIGAM) at approximately 8 months post-amputation. The average age of the participants was 60.7 years, and 79.4% had an amputation due to vascular complications. Verbal fluency (FAS 36 test) was the only variable significantly associated with hours of prosthesis wear, such that higher verbal fluency was associated with greater wearing. SIGAM scores were significantly associated with memory function, with lower mobility associated with lower memory recall.
Bilodeau et al. 24 assessed orientation and general mental status to explore potential association with prosthesis use (measured by the Day’s 37 questionnaire). The average age of the participants was 71.6 years, and 100% had an amputation due to vascular complications. 24 Day’s questionnaire evaluates prosthesis donning/doffing, wear time, functional mobility, and social interaction. Measurements were assessed in several phases following their prosthesis prescription by phone and survey. Prosthesis use was significantly associated with cognition function; those with a higher score on the Short Portable Mental Status Questionnaire (SPMSQ) 38 demonstrated greater use of a prosthesis.
Discussion
The current literature review was developed to evaluate the association between cognitive function and prosthesis use in older adults who underwent LLA secondary to vascular disease, with a particular focus on how prosthesis use was defined. Of the nine studies included in this review, seven demonstrated a predictive relationship between a measure of cognitive ability and prosthesis use.6,25 –27,30,31 Of the two studies that did not find a relationship between cognition and a prosthesis use, a relationship was found with a mobility outcome (non-prosthesis specific).28,29 A total of eight distinct prosthesis-related outcomes were utilized in defining prosthesis use. The weighted average age of participants of included studies was 67.6 years, and 95% of the participant’s included in this review had an amputation due to vascular etiology, including diabetic complications.
This literature review is discernibly different from previous reviews as it focuses exclusively on vascular LLA cases, only includes studies where prosthesis use and cognitive function were assessed as a discrete measure, and includes any articles published since 2012. Previous literature reviews have indicated that superior cognitive function is associated with better prosthesis-related outcomes. Sansam et al. 23 examined factors influencing walking after an amputation, with all ages and etiologies considered eligible for inclusion. Of the 57 articles reviewed, 6 studies26,28,30,39 –41 reported cognitive ability as a significant predictor of walking ability. Of those six studies, one study looked at participants with a dual diagnosis of hemiparesis and amputation 41 and one included a study that failed to report amputation etiology. 40 O’Neill 11 published a review examining the psychological and demographic predictors of rehabilitation outcomes following amputation. The average age range in the study was 60.3–79.7 years. All etiologies were eligible for inclusion. Outcomes considered for inclusion were disability, mobility on a graded scale, and prosthesis use. Cognitive abilities were assessed in 9 of the 13 reviews, with 8 published studies demonstrating a predictive relationship between cognitive ability and functional/motor outcome following amputation.6,25,26,28,32,40,42,43 Coffey et al. 12 performed a review that examined cognitive function in persons with LLAs. Ages 18+ years were included in the study, and assessment of cognitive function had to be assessed as a discrete variable to be eligible for inclusion. All outcomes were considered for this review. Thirty studies were reviewed, and 13 found an association between cognitive impairment and success with a variety of prosthesis-related and mobility outcomes.4,6,24 –27,30,39 –41,43 –45
Prosthesis use measurement issues
Based on the included studies, it is evident is that prosthesis use is defined in a multitude of different manners: functional mobility, gait, hours of prosthesis wearing, fitting, and activity level. This raises the question of how best to measure prosthesis use. However, prosthesis use is a much broader construct that is made up of numerous facets, including but not limited to donning/doffing, transfers, ambulation, environmental navigation, and occupational utilization. When only including functional mobility outcomes specific to prosthesis users, a number of measures were used: SIGAM, Volpicelli scale, and the scale adapted by Pohjolainen. The Schoppen et al. study evaluated prosthesis use by ranking the ability to ambulate with or without an assistive device, use of a wheelchair, and the type of environment that is traversed. The scale does not take into consideration distance ambulated or the type of activities being performed. It also fails to capture the patient’s ability to don/doff the prosthesis, which would be the precursor to any functional mobility. Since donning presents an issue to older adult prosthesis users, it is specious to measure functional mobility without considering the impact of self-management. 9 A similar issue was found in other included studies which predicted prosthesis use using strictly mobility measures that are insensitive to the multifaceted construct of true prosthesis use.
Bilodeau et al. did include a robust prosthesis-related outcome measure. Day’s questionnaire is an example of a measure that is sensitive to more than just functional mobility or other singular facets of prosthesis use. Day’s questionnaire evaluates the ability to don/doff the prosthesis, wearing time, elevation negotiation, living environment, ambulation assisted devices, activities of daily living, walking habits, and social/occupational participation. The scored questionnaire gives an overall perspective that demonstrates the subject’s general activity level. It was correlated to the number of steps per year measured by a counter inserted in the heel of the prosthesis. 37 Other comprehensive prosthesis-related outcome measures are the Prosthesis Evaluation Questionnaire (PEQ) and Orthotic Prosthetic User Survey (OPUS). The PEQ consists of nine validated scales that can be run independently of each other and is a self-reported survey utilizing a visual analog scale for responses. 18 The scale is limited in that it assesses mobility only in global sense, but offers insight into the ability of the patient to self-manage, their coping skills, prosthesis satisfaction, and social well-being. OPUS evaluates mobility, self-management, wearing time, and satisfaction. 19 While multi-dimensional outcomes can complicate data analysis in some instances, these measures would be better suited in evaluating the predictive relationship between cognition and prosthesis-related outcomes as they are comprehensive and consider prosthesis use as a multifaceted construct.
Cognitive ability assessment issues
One complication in summarizing the findings from this literature review was the wide variability in operational definitions of cognition, a broad theoretical construct with multiple information processing subdomains, including memory, attention, inhibitory control, and decision-making. 46 Studies that fail to assess cognitive subdomains are inherently limited in their explanatory power. There were several studies designed with the possibility that different cognitive subdomains may have differential effects on prosthesis use. Three of the surveyed studies provided an appropriately wide array of cognitive measures: (1) O’Neill and Evans, 27 who conducted a broad battery of tests sensitive for several cognitive subdomains (including memory, executive function, visuospatial cognition, and language fluency); (2) Schoppen et al., 28 who included measures of memory and response inhibition; and (3) Williams et al., 31 who included a range of neuropsychological assessments beyond general mental status that measured verbal intelligence, attention, and memory. Pinzur et al. 6 included a number of cognitive measures for mental function, memory, perceptual skills, and personality. However, this study has been criticized for not properly presenting either performance results or cognitive assessment methods 5 and additionally utilized disparate cognitive assessments between their younger and older adult cohorts, thereby complicating age group analyses.
Multiple studies were limited by relying solely on cognitive measures designed to assess dementia-level impairments, such as the MMSE 47 and clock test.25,29,30 As such, these studies address only gross cognitive decline rather than detailing which specific cognitive subdomains are most operative in prosthesis use. Furthermore, research has challenged the sensitivity of the MMSE in detecting mild cognitive impairment (MCI).48,49 For instance, recent studies comparing the sensitivity of the MMSE and Montreal Cognitive Assessment (MoCA) in detecting cognitive impairments in older adults have found that while the MMSE is sensitive for detecting profound cognitive impairments, it is inferior to the MoCA in detecting MCI.50,51 Accordingly, studies that failed to demonstrate a predictive relationship between the MMSE score and prosthesis use 29 may be insensitive to a potential predictive relationship (i.e. a Type 2 error).
Interestingly, several of the sampled studies included within their cognitive battery measures of anxiety and depression.24,26 –28 Including emotional state measures is reasonable, given that depression and anxiety are joint risk factors for cognitive decline and dementia. 52 However, the surveyed studies were often imperfect in implementing the emotional measures. In two studies,24,27 emotional adjustment capacity was measured but was not included in the regression models. Thus, the potential role of emotion on cognition and prosthesis adoption success remains largely unexplored.
The studies included in this review were focused on prosthesis use as the primary outcome variable, and the cognitive measures were included as potential predictors but were often underdeveloped. Although this does not invalidate the link between cognition (broadly construed) and prosthesis use, it represents a fundamental limitation in both the extent of their relationship and the specificity of cognitive factors involved in successful prosthesis use. Future research should be directed to tease out which specific cognitive subdomains are of greatest relevance in predicting successful use of prosthetic devices.
A limitation of the study was the narrow search criteria, which restricted which prosthesis-related outcome measures could be included. While insight into the nature and depth of the included measures was garnered, the constructs represented in other prosthesis-related outcome measures should be studied further. Further limiting the generalizability of the study is the small sample of included articles published at the time of this review.
Conclusion
Cognitive ability demonstrates a predictive role in prosthesis use among older adults who underwent amputation due to a vascular etiology in 78% of the included studies. Evidence of dementia, decreased verbal or immediate memory, decreased learning capacity, and decreased attention were all associated with poor prosthesis-related outcomes. Prosthesis use is defined using different constructs depending on the study, making it difficult to draw comparisons. While no singular measure can account for all dimensions, the inclusion of at least one multifaceted outcome measures, such as OPUS and the Day’s questionnaire, is recommended. Future studies should evaluate prosthesis use with outcomes capable of representing the multifaceted construct of functioning with a prosthetic limb. This review supports the use of cognitive assessment in the comprehensive evaluation of the older adult undergoing amputation due to vascular etiologies.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.