
Abstract
Background:
Fall prevention is essential in patients after arthroscopic rotator cuff repair because of the high risk of re-rupture. However, there are no reports related to falls that occur during the early postoperative period, while the affected limb is immobilized.
Objectives:
This study assessed gait performance and falls in patients using a shoulder abduction brace after arthroscopic rotator cuff repair.
Study design:
Prospective cohort and postoperative repeated measures.
Methods:
This study included 29 patients (mean age, 67.1 ± 7.4 years) who underwent arthroscopic rotator cuff repair followed by rehabilitation. The timed up and go test, Geriatric Depression Scale, and Falls Efficacy Scale were measured, and the numbers of falls were compared between those shoulder abduction brace users and patients who had undergone total hip or knee arthroplasty.
Results:
In arthroscopic rotator cuff repair patients, there were significant improvements in timed up and go test and Geriatric Depression Scale, but no significant differences in Falls Efficacy Scale, between the second and fifth postoperative weeks (p < 0.05). Additionally, arthroscopic rotator cuff repair patients fell more often than patients with total hip arthroplasty or total knee arthroplasty during the same period.
Conclusion:
The findings suggest that rehabilitation in arthroscopic rotator cuff repair patients is beneficial, but decreased gait performance due to the immobilizing shoulder abduction brace can lead to falls.
Clinical relevance
Although rehabilitation helps motor function and mental health after arthroscopic rotator cuff repair, shoulder abduction brace use is associated with impaired gait performance, high Falls Efficacy Scale scores, and risk of falls, so awareness of risk factors including medications and lower limb dysfunctions is especially important after arthroscopic rotator cuff repair.
Background
Arthroscopic rotator cuff repair (ARCR) to treat rotator cuff tendon tears is a common orthopedic surgical procedure in Japan. Compared to open rotator cuff repair, ARCR is less invasive to the deltoid muscle and typically has earlier and better postoperative functional recovery.1–3 Previous studies have shown good clinical results, including improved joint range of motion (ROM) and reduced pain in post-ARCR patients;4–6 recent studies have also shown that rehabilitation is important for improving muscle strength for performing activities of daily living. 7 Complications after ARCR include re-tear of the rotator cuff, anchor-related trouble, shoulder joint contracture, anesthesia complications, complex regional pain syndrome (CRPS), carpal–cubital tunnel syndrome, infection, and deep vein thrombosis. 8 Risk factors such as age, number of ruptured tendons, tear size, fatty degeneration, and thickness of the supraspinatus also affect the postoperative results of ARCR. Re-rupture is the most problematic complication, and rotator cuff tears are still commonly reported after ARCR.9–12 A shoulder abduction brace (SAB) is often used in order to prevent postoperative tears and promote healing of the repaired tendon. In addition, early ROM exercise is customarily performed in conjunction with fixation by an SAB in order to avoid shoulder contracture.13,14 However, previous studies on the adverse effects and complications of wearing a brace have only evaluated computer operation, discomfort while wearing certain types of brace, 15 and differences in comfort depending on external rotation angle. 16 Although the effects of wearing an abduction brace have not been thoroughly studied, the nature of the aforementioned complications, particularly CRPS, cubital tunnel syndrome, and contracture, would be consistent with being caused by the use of a brace. Shoulder surgery does not necessarily attract much attention to the need to prevent falls, but postoperative falls may lead to injuries including to re-rupture. Common factors related to falls include internal factors (e.g. disorder or disability, drugs, body and mind impairment associated with aging, and lower limb weakness affecting walking stability) and external factors (e.g. material environment),17,18 but any factors specifically contributing to falls in postoperative ARCR patients remain unclear. Perhaps they may differ from those affecting patients who have undergone lower limb surgery. This study was intended to clarify the relative needs for fall prevention among ARCR patients in an orthopedic postoperative setting, in perspective with the recognized needs of other patients after total hip arthroplasty (THA) or total knee arthroplasty (TKA) by (1) evaluating walking-related indicators and changes in peripheral symptoms during brace use and (2) comparing the number of falls and gait performance in postoperative ARCR patients to those of patients who had undergone lower limb surgery.
Methods
Subjects
All patients who underwent ARCR at the Department of Orthopedic Surgery at Shiga University of Medical Science Hospital between June 2013 and April 2014 were enrolled in this study. An SAB (Kenbag, REHABITECH, Rakuhoku Prosthetic and Orthotic Manufacturing Co., Ltd, Kyoto, Japan) was used to immobilize the joint after surgery. The control group consisted of patients who had undergone lower limb arthroplasty during the same period, including THA and TKA. All patients in all three groups began rehabilitation from the day after surgery until hospital discharge and were transferred to the convalescence rehabilitation ward (CRW) from the orthopedic ward. The criteria for admission to this study were C-reactive protein (CRP) levels ⩽3 mg/dL (CRP above 3 mg/dL indicating inflammation, possibly due to infection) and independent gait. The exclusion criteria included osteonecrosis or rheumatoid arthritis, neurological symptoms such as stroke or Parkinson’s disease, advanced disuse syndrome, and cancer. This study was performed in accordance with the principles of the Declaration of Helsinki. The medical ethics committee of our university approved the protocol, and all participants provided written informed consent before participating in the study.
Procedures
For all patients enrolled in this study, receiving ARCR or THA or TKA, the following parameters were examined at the time of study admission (transfer from orthopedic department to rehabilitation unit) and at the time of hospital discharge. Motor functions were assessed using grip strength, knee extension force (KEF), and timed up and go test (TUG) findings. KEF was assessed using an IsoForce GT-360 (OG Giken Co. Ltd, Okayama, Japan) measuring isometric contraction for 3 s. Torque was calculated by multiplying the length of the lever arm (distance between the force sensor and the knee pivot) by the measured force, and KEF was expressed as a ratio of torque to body weight (N m/kg). The TUG was used to measure the time (in seconds) required for the participant to stand up from an armless chair (chair seat height ~ 40 cm) and walk a distance of 3 m, then turn, walk back to the chair, and sit down, and it was used to assess ambulatory ability and balance; for each patient, the better score of two trials was used. Cognitive function was assessed using the mini-mental state examination (MMSE; score range, 0–30; lower scores indicate worse performance). 19 Depression was assessed using the Geriatric Depression Scale (Short Form) (GDS-15; score range, 0–15; higher scores indicate worse performance).20,21 Health-related quality of life was assessed using the Medical Outcomes Survey 8-Item Short-Form Health Survey (SF-8; norm-based score, 50; lower scores indicate worse performance).22,23 In order to evaluate the fear of falling and self-efficacy, we used the Falls Efficacy Scale (FES), 24 developed by Hill et al. 25 to examine 14 activities associated with activities of daily living. In this test, 10 stages of self-confidence against falling (1: absolutely no confidence to 10: extremely confident) were evaluated, with higher scores showing strong confidence to not fall. Additionally, gender, age, body mass index (BMI), dominant hand, any impairment of vision and hearing, comorbidities (hypertension, heart failure, diabetes, hyperlipidemia, or respiratory disease), discharge destination and family structure, regular prescription drugs, and the incidence of in-hospital falls (during brace therapy for ARCR patients) were all investigated. We used the following tools to assess preoperative joint function: tear size (according to the classification proposed by Cofield) and Japanese Orthopaedic Association Shoulder Score (JOA-SS) in ARCR patients; modified Harris Hip Score (mHHS) in THA patients; and Knee Society score (KSS) in TKA patients.
The ARCR-critical path in our hospital requires 4 weeks with an SAB for medium-size or smaller tears or 5 weeks for large-size or greater tears. Upon admission to the rehabilitation unit, all patients are wearing “DON” the abduction brace at 45° (Figure 1). Depending on the tear size, the braces are removed “DOFF” 4 or 5 weeks after surgery, and the patients are discharged on the next day, unless their pain worsens. The rehabilitation program for ARCR patients at our hospital is shown in Figure 1. When the pain is nonexistent or bearable, we start isometric strength training around the shoulder joint and scapula during the early period. Muscle strengthening exercises of the lower limbs are not performed; however, patients are instructed to walk to prevent deep vein thrombosis and maintain lower limb muscle strength (Figure 1). The THA or TKA rehabilitation program lasts 4 weeks. Walking is started from the next day after surgery. 26
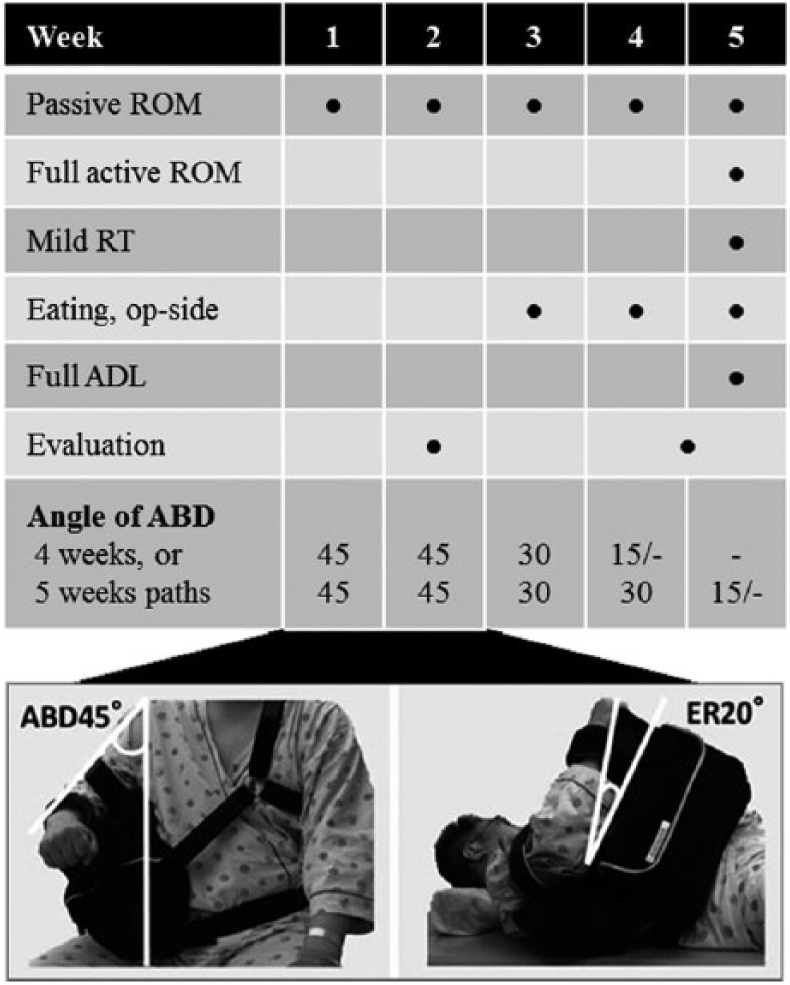
Arm positioning of the shoulder brace at admission.
Statistical analysis
Data were expressed as medians and quantiles, or percentages of number. Kruskal–Wallis one-way analysis of variance (ANOVA) with Mann–Whitney U post hoc test or Chi-square test was used to determine the significance of differences among the three groups. Wilcoxon signed-rank test was used to determine the significance of differences between DON and DOFF in the ARCR group. In addition, in TUG of DON (or THA or TKA at admission), the correlation of each indicator was used to determine Spearman’s rank correlations; those that showed significant differences were included as explanatory variables in stepwise multiple regression analysis. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Tokyo, Japan) and Bonferroni-corrected p-values <0.05 were considered statistically significant.
Results
In accordance with the inclusion criteria, the ARCR group consisted of 29 patients (8 women and 21 men), with a mean age of 67.1 ± 7.4 years (51–84 years) and mean BMI of 23.7 ± 2.4 kg/m2 (20.0–29.3 kg/m2). The THA group included 39 patients (35 women and 4 men) with a mean age of 67.7 ± 9.0 years (49–81 years) and a mean BMI of 23.4 ± 3.7 kg/m2 (17.5–33.7 kg/m2). The TKA group consisted of 56 patients (46 women and 10 men), with a mean age of 71.6 ± 8.3 years (52–86 years) and mean BMI of 25.9 ± 3.7 kg/m2 (19.4–35.0 kg/m2). Table 1 summarizes the patient characteristics. There were significant differences between ARCR and THA or TKA patients regarding the length of stay, sex ratio, and physique, but there were no significant differences among the three groups in terms of the number of drugs and comorbidities (Table 1). The leading comorbidity among the ARCR patients was hyperlipidemia (55.2%), followed by hypertension (37.9%). Drugs prescribed to treat comorbidities included analgesics (72.4%) and soporifics (44.8%). Soporifics were used by 13 of 29 patients: 9 and 4 patients were taking benzodiazepines and non-benzodiazepines, respectively. ARCR patients more often used hypnotics than did THA or TKA patients, although this difference was not statistically significant (Table 1). Moreover, compared to THA or TKA, ARCR patients had significantly better TUG times, KEF, and FES scores, but also more reported falls (Table 1). CRPS was not observed in any postoperative patients within this study period.
Patient characteristics.
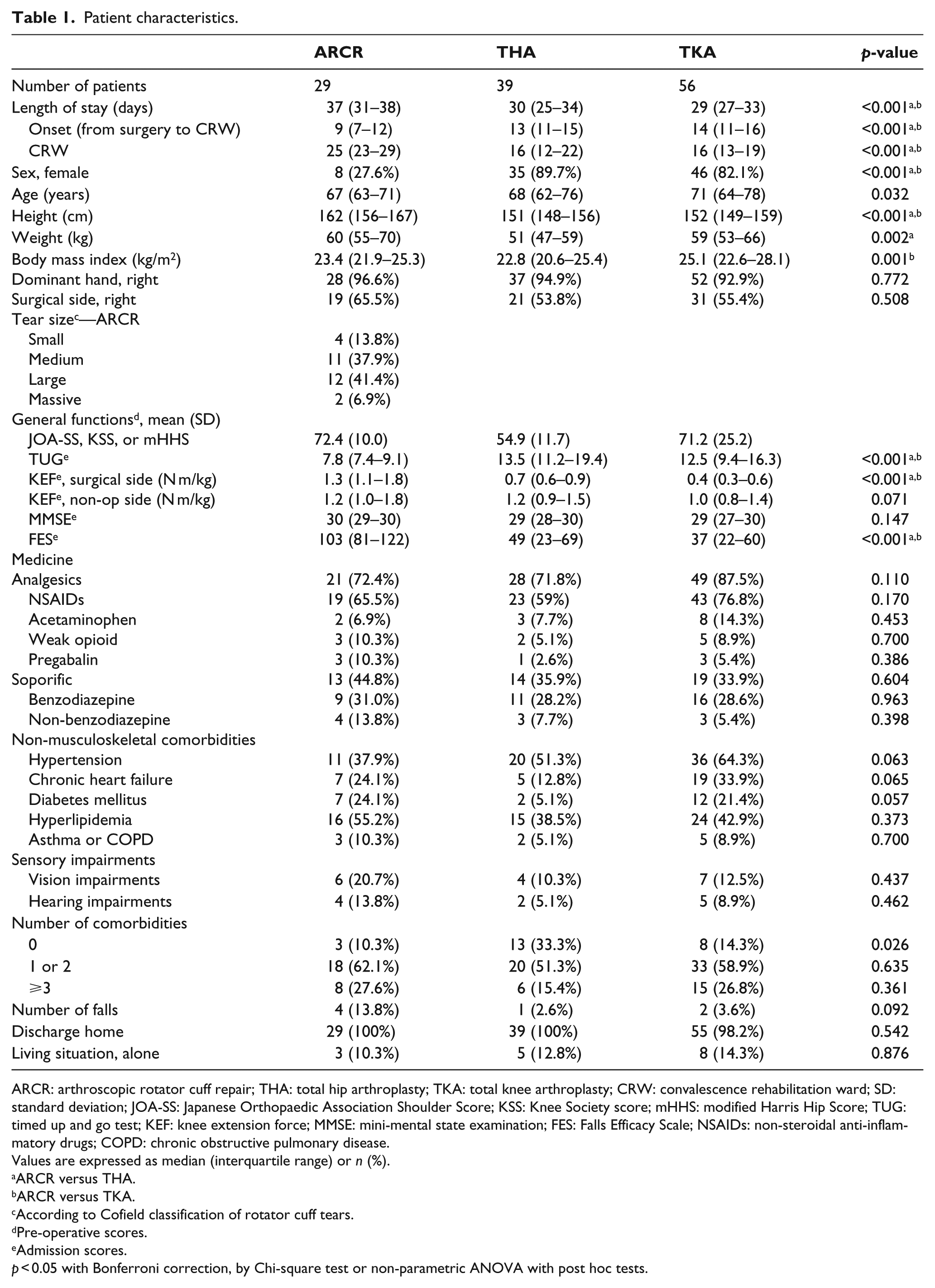
ARCR: arthroscopic rotator cuff repair; THA: total hip arthroplasty; TKA: total knee arthroplasty; CRW: convalescence rehabilitation ward; SD: standard deviation; JOA-SS: Japanese Orthopaedic Association Shoulder Score; KSS: Knee Society score; mHHS: modified Harris Hip Score; TUG: timed up and go test; KEF: knee extension force; MMSE: mini-mental state examination; FES: Falls Efficacy Scale; NSAIDs: non-steroidal anti-inflammatory drugs; COPD: chronic obstructive pulmonary disease.
Values are expressed as median (interquartile range) or n (%).
ARCR versus THA.
ARCR versus TKA.
According to Cofield classification of rotator cuff tears.
Pre-operative scores.
Admission scores.
p < 0.05 with Bonferroni correction, by Chi-square test or non-parametric ANOVA with post hoc tests.
The presence or absence of the brace (DON or DOFF) was associated with significant differences in non-surgical side KEF, TUG, GDS-15, and vitality and role emotional in the SF-8 (Table 2). There was no significant difference in grip strength, MMSE score, body pain in SF-8, and FES score.
Functional evaluation in the presence and absence of shoulder abduction brace.
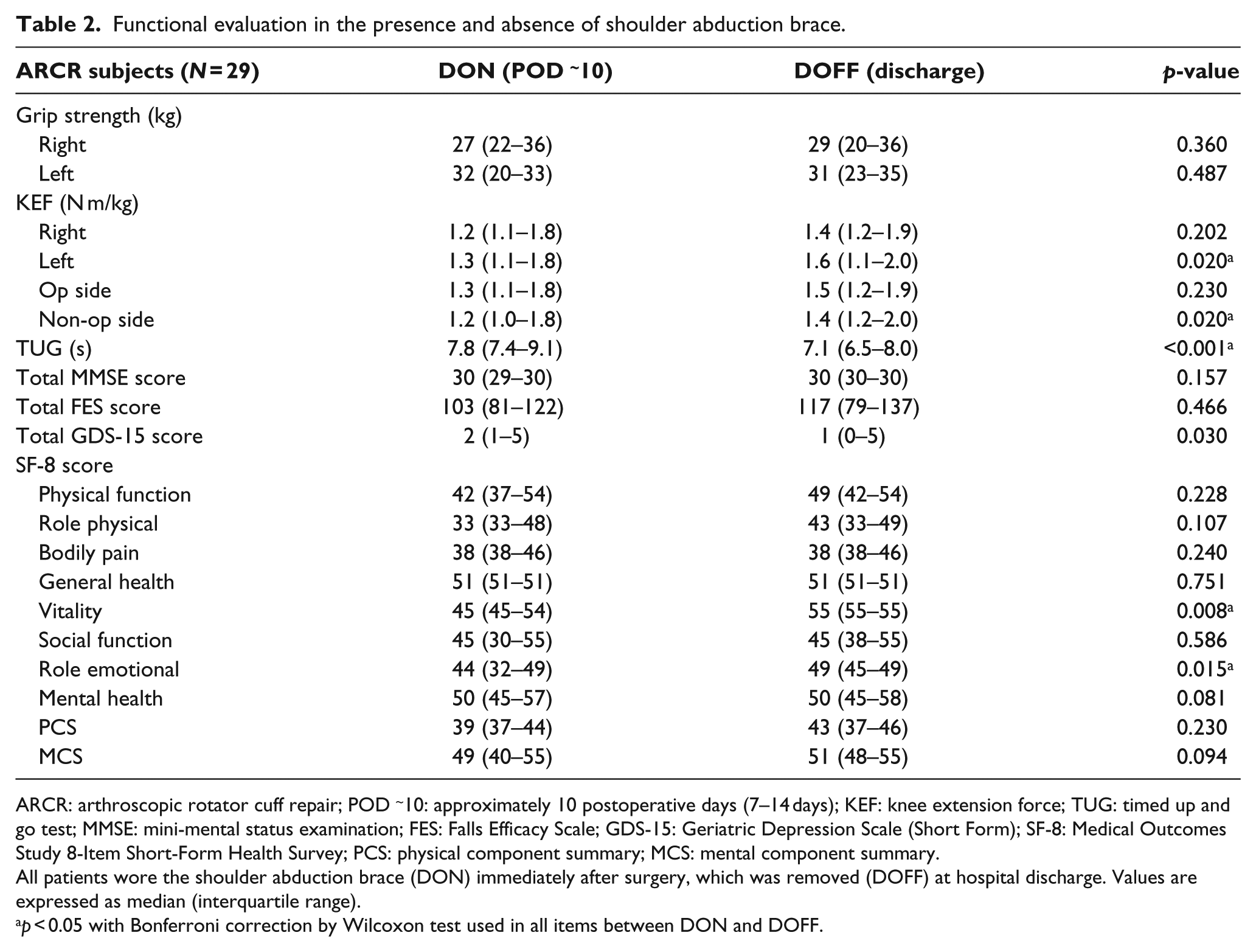
ARCR: arthroscopic rotator cuff repair; POD ~10: approximately 10 postoperative days (7–14 days); KEF: knee extension force; TUG: timed up and go test; MMSE: mini-mental status examination; FES: Falls Efficacy Scale; GDS-15: Geriatric Depression Scale (Short Form); SF-8: Medical Outcomes Study 8-Item Short-Form Health Survey; PCS: physical component summary; MCS: mental component summary.
All patients wore the shoulder abduction brace (DON) immediately after surgery, which was removed (DOFF) at hospital discharge. Values are expressed as median (interquartile range).
p < 0.05 with Bonferroni correction by Wilcoxon test used in all items between DON and DOFF.
At admission to the CRW, analysis of TUG-values among SAB-wearers (DON-TUG) revealed a correlation between age, JOA-SS, and KEF (Table 3). Multiple regression analysis (adjusted R2 = 0.493, p < 0.0001) indicated independent associations between DON-TUG and significant correlation with non-surgical-side KEF (partial correlation r = −0.567, p = 0.002) and JOA-SS (partial correlation r = −0.499, p = 0.007). In contrast, THA-TUG or TKA-TUG analysis revealed a correlation between age, non-surgical-side KEF, MMSE score, FES, GDS-15, and number of medicines or comorbidities (Table 3). Multiple regression analysis (adjusted R2 = 0.186, p < 0.0001) indicated independent associations between DON-TUG and significant correlation with non-surgical-side KEF (partial correlation r = −0.442, p < 0.0001).
Correlation of timed up and go test results in postoperative persons using a shoulder abduction brace: comparison with lower limb surgery.
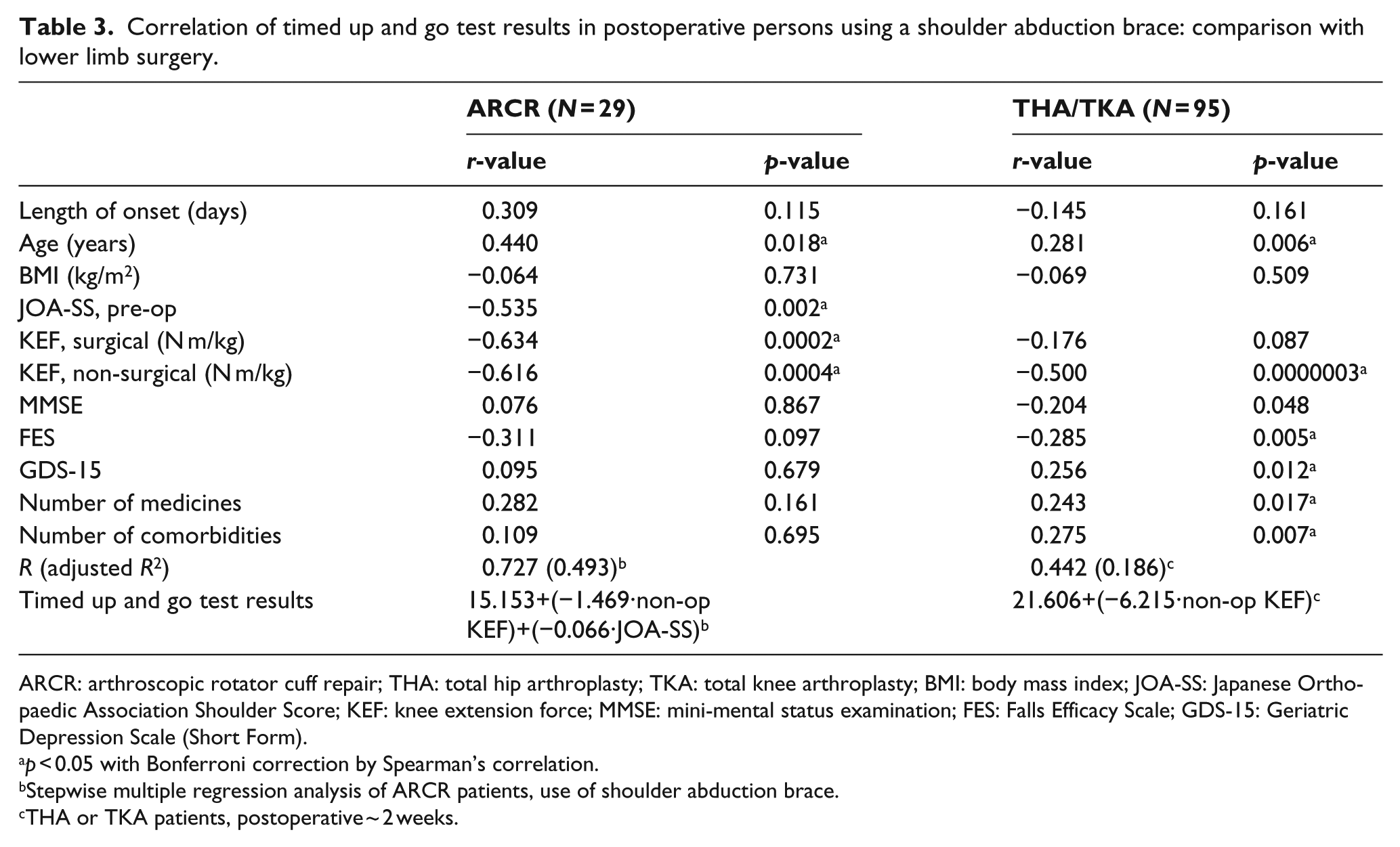
ARCR: arthroscopic rotator cuff repair; THA: total hip arthroplasty; TKA: total knee arthroplasty; BMI: body mass index; JOA-SS: Japanese Orthopaedic Association Shoulder Score; KEF: knee extension force; MMSE: mini-mental status examination; FES: Falls Efficacy Scale; GDS-15: Geriatric Depression Scale (Short Form).
p < 0.05 with Bonferroni correction by Spearman’s correlation.
Stepwise multiple regression analysis of ARCR patients, use of shoulder abduction brace.
THA or TKA patients, postoperative ~ 2 weeks.
The postoperative fall incidence was 13.8% (4/29) after ARCR, higher than after THA (2.6%, 1/39) and TKA (3.6%, 2/56) during the same period (Table 1). Additionally, all four ARCR patients who fell had undergone surgery on their dominant-hand side, and they fell while reaching with the non-dominant hand. The ARCR patients who fell had slower TUG and poor walking balance, had ⩾2 comorbidities including impaired vision (cataract), and had used benzodiazepine drugs.
Discussion
This study evaluated a range of factors including the relative rate of falls while wearing a brace after ARCR. Comparison of DON and DOFF (discharge) measurements in ARCR patients revealed significant improvements in non-surgical-side KEF, TUG, and vitality and role emotional functioning in the SF-8. These results suggest that the abduction brace has negative effects on walking balance, mood, and quality of life, and/or that those improvements occurred during the time of rehabilitation. The median TUG times of the ARCR patients fell from 7.8 s with the SAB on to 7.1 s without it, consistent with less alacrity while wearing a brace, which is plausibly a risk factor for falls. Coleman and Clifft 27 showed that shoulder immobilization can impair balance and increase the risk of falls, but here FES was relatively high (fear of falling was low) and there was no significant difference in FES between DON and DOFF. This discrepancy between confidence and performance suggests that overconfidence may lead to falls. Although the TUG cut-off for considering a person to be at high risk for falling is 13.5 s, 28 none of our ARCR patients was considered to be at high risk of falling, even while wearing a brace, as their TUG and KEF scores were good (Table 1). Nevertheless, the number of ARCR patients who experienced postoperative falls was greater than the number of THA and TKA patients with poor walking function. The confounding factors of TUG include age, BMI, and KEF; in addition, it is not possible to predict falls with the TUG test alone. 28 Therefore, in order to prevent falls, as shown in this study, multiple indicators should be used to evaluate walking ability and the risk factors of falls. There was a significant difference in non-operated-side KEF values between brace-wearing ARCR patients and THA/TKA patients, and a corresponding difference was seen also in the TUG measurements. This non-operated-side KEF difference existed in cases whose operated side was the dominant-hand side (>90% being right-handed) and in those which were contralateral. TUG differences between brace-wearing ARCR patients and THA/TKA patients differed in magnitude according to whether the non-operated side was ipsilateral with the dominant-hand side. Thus, we suspect that brace use has asymmetric effects on weight-distribution and gait-agility, and we speculate that where the dominant-side shoulder (the right side in >90% of ARCR patients) was immobilized, unaccustomed use of the other hand led to a change in weight-bearing and an increase in contralateral (i.e. left side) KEF.
Fall risk is multi-factorial: loss of mental function can also lead to reduced motor function,17–25 and additional fall risks in ARCR patients include uncertain footing due to visual field loss caused by the abduction brace, and lightheadedness and balance disorder due to medications. Vision impairments such as those resulting from cataracts have been associated with hip fractures and falls in the elderly. 29 In our study, 20.7% of ARCR patients presented with visual impediments, likely increasing fall risk among those who fell while wearing the brace. Moreover, use of medications and administration of multiple drugs (e.g. soporific, antipsychotic, antihypertensive, diuretic, analgesic/non-steroid anti-inflammatory drugs, anticonvulsant, antiparkinsonian drugs, and iron) may lead to increased incidence of adverse events such as falls and delirium. Richardson et al. 30 reported that the use of multiple medications including soporifics was associated with an increased risk of falls; use of benzodiazepines was a harmful independent factor for falls, while other drugs such as antihypertensive agents, diuretics, and antipsychotics were not associated with falls. Benzodiazepines as well as non-benzodiazepines also reportedly increase fall risk.31–33 In this study, 44.8% of patients who underwent ARCR used soporifics, and all the patients who fell used soporifics; of these, 75% of the patients were using benzodiazepines. Thus, we believe that use of benzodiazepines is a risk factor for falls in post-ARCR patients.
In order to clarify the characteristics that led to falls in patients who had undergone ARCR, this study compared walking and falling-related indicators in this group to those of THA or TKA patients. Both TUG and KEF were better in the ARCR patients, despite their upper limb impairment, compared to those of patients with lower limb impairment who underwent THA or TKA with rehabilitation; however, the incidence of falls among ARCR patients was extremely high. In addition to the aforementioned overconfidence in their ability, visual defects due to the brace, and medication use, an additional factor related to falling was the dominance of the operated side. Patients were more likely to fall when reaching out with their non-dominant hand; it is possible that they could not maintain their balance when required to move in non-routine ways. In one of the many studies on the risk of falling, Robinovitch et al. 34 investigated an actual fall scene using a video monitor and showed that slipping was rare; most falls were caused by incorrect weight shifts immediately after walking or sitting. Unfamiliar weight shifts associated with reaching motions using their non-dominant side may have contributed to the higher rate of falls in this study. Therefore, preoperative guidance may be important to prevent falls after ARCR. The confounding factors of TUG at DON, which is unlike the THA and TKA groups, included preoperative JOA-SS in addition to age and KEF, which might lead to reduced balance while walking due to shoulder joint dysfunction. Regardless of immobilization of the affected limb, this is likely due to decreased arm swing due to pain and dysfunction in the affected shoulder joint. It is necessary to verify these observations using three-dimensional gait analysis, including the upper extremities.
In this study, we examined the implications of an SAB for walking balance and falls in a cohort study of ARCR patients. This study has several limitations, including not being implemented as a randomized controlled trial, the unclear impact of the brace or the effect of rehabilitation on different lengths of brace use (and non-use), and the fact that differences in the number of postoperative days elapsed and the intensity of corresponding pain might have affected each index, though most patients received analgesics. Despite these limitations, there were no significant differences in body pain as assessed by SF-8 between postoperative weeks 2 and 5, and CRPS was not reported. Therefore, because there was little difference in secondary dysfunction due to pain between DON and DOFF in ARCR patients, we believe the significant differences observed in this study to be predominantly an effect of shoulder brace use (immobilization) and rehabilitation.
Conclusion
To our knowledge, this is the first study to examine the impact of the SAB on factors related to falls in patients undergoing ARCR. We assessed the impact of the fixed brace on walking and falling in postoperative ARCR patients by comparing the brace worn in 45° abduction (2 weeks after the operation) and immediately after removing the brace (at discharge). We also examined differences between ARCR and THA or TKA patients in the same period. Our results revealed that ARCR patients fell more often than THA or TKA patients; in addition, although rehabilitation has a significant effect on motor function and mental health shortly after ARCR surgery, use of an immobilization brace was associated with impaired gait performance and with falls.
Footnotes
Acknowledgements
This study was approved by the research ethics committee of Shiga University of Medical Science (24-3).
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.