
Abstract
Background:
This literature review was undertaken to determine if commonly held views about the benefits of a bone bridge technique are supported by the literature.
Methods:
Four databases were searched for articles pertaining to surgical strategies specific to a bone bridge technique of the transtibial amputee. A total of 35 articles were identified as potential articles. Authors included methodology that was applied to separate topics. Following identification, articles were excluded if they were determined to be low quality evidence or not pertinent.
Results:
Nine articles were identified to be pertinent to one of the topics: Perioperative Care, Acute Care, Subjective Analysis and Function. Two articles sorted into multiple topics. Two articles were sorted into the Perioperative Care topic, 4 articles sorted into the Acute Care topic, 2 articles into the Subjective Analysis topic and 5 articles into the Function topic.
Discussion:
There are no high quality (level one or two) clinical trials reporting comparisons of the bone bridge technique to traditional methods. There is limited evidence supporting the clinical outcomes of the bone bridge technique. There is no agreement supporting or discouraging the perioperative and acute care aspects of the bone bridge technique. There is no evidence defining an interventional comparison of the bone bridge technique.
Conclusion:
Current level III evidence supports a bone bridge technique as an equivalent option to the non-bone bridge transtibial amputation technique. Formal level I and II clinical trials will need to be considered in the future to guide clinical practice.
Clinical relevance
Clinical Practice Guidelines are evidence based. This systematic literature review identifies the highest quality evidence to date which reports a consensus of outcomes agreeing bone bridge is as safe and effective as alternatives. The clinical relevance is understanding bone bridge could additionally provide a mechanistic advantage for the transtibial amputee.
Keywords
Background
Amputation can be an inevitable consequence of disease and trauma, where limb salvage is an inferior alternative. There is not a consensus as to the best course of action when both amputation and limb salvage are considered. 1 Physical outcomes of amputation have been reported to be equivalent to limb salvage. Amputation and use of a prosthesis can provide near normal functional outcomes for the transtibial amputee (TTA). The foundation of the outcome is a physiologically sound residual limb (RL). 2 However, traditional techniques of lower extremity amputation can be associated with a number of complications.3,4 Alternative amputation techniques should be considered in guiding clinical practice and improving outcomes when amputation is the best choice. Identifying techniques that might improve outcomes for amputation is the first step to establish these evidence-based practice guidelines.
An alternative addition to transtibial amputation is a bone bridge, which considers limitations of traditional procedures. 5 A bone bridge technique described by Ertl 6 reportedly restores intraosseous pressure through canal obliteration while expanding the area of terminal support by creating a bony bridge between the distal tibia and fibula. 6 The stabilization of the tibia and fibula through this bone bridge eliminates potentially painful movement of the fibula while creating a blunt surface at the distal end of the RL. This may allow improved distal weight bearing while decreasing pain and skin compromise compared to a more commonly practiced non–bone bridge. Distal weight bearing could assist in less dependence on circumferential pressure necessary for prosthesis socket function while improving pressure distribution. This distal weight–bearing capability could improve the distribution of the applied forces in prosthesis socket design while accommodating volume fluctuation or a suboptimal fit socket. 6
These considerations could lead to a superior amputation reconstruction and improved outcomes for the transtibial prosthesis user. Understanding the potential risk and outcome benefit of a bone bridge technique compared to a more traditional amputation would help evaluate a true comparison of techniques and guide clinical practice. It is timely to review the most current, highest quality literature available to address a transtibial bone bridge amputation technique. Therefore, the purpose of this systematic literature review (SR) was to evaluate the highest quality of evidence available to guide clinical practice for adult patients’ outcomes regarding a bone bridge surgical technique compared to a non–bone bridge, when a transtibial amputation is necessary.
Methods
A systematic review was performed on 27 February 2015. Given that the bone bridge (Ertl) technique was first described in 1949, 7 no start date limits were set to the search. The following databases were searched: PubMed, CINAHL, Ovid, and Web of Science. Search statements and strategies by database are outlined (Table 1). General methods for search strategy have been used in two prior prosthesis systematic review studies.8,9 The searches were adjusted for variations in subject headings across individual databases, and subject headings were combined with selected keywords. The number of reference articles retrieved across the databases allowed for direct selection of pertinent research, that is, a study/publication type hedge was deemed unnecessary. Bibliographic citation software (Endnote X6; Thomas Reuters, Carlsbad, CA, USA) was utilized to collect references and remove duplicates. The multi-disciplinary review team also manually searched referenced articles and articles personally known to investigators. Articles were independently reviewed by two investigators according to inclusion/exclusion criteria who classified them as either pertinent or not pertinent. Full text was reviewed by both investigators (Figure 1).
Search terms.
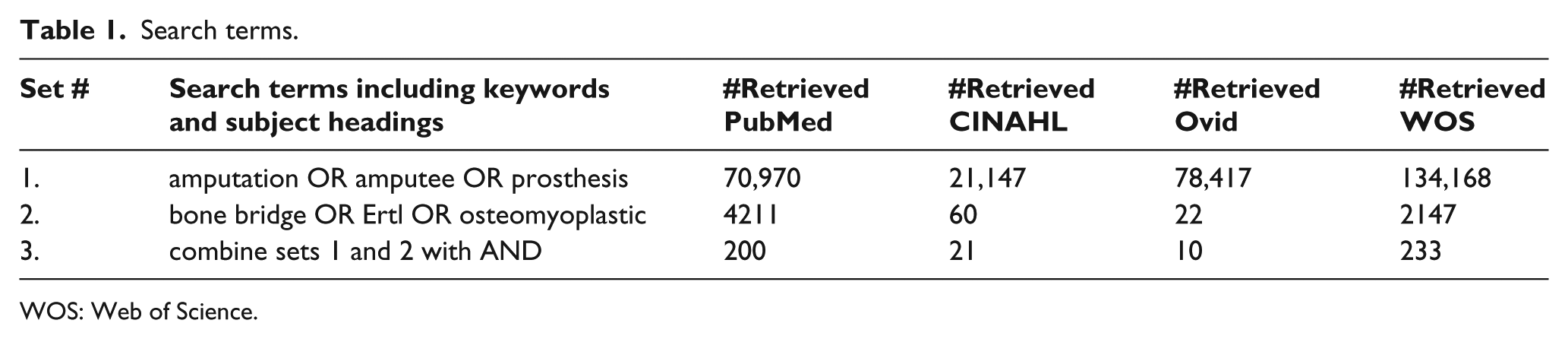
WOS: Web of Science.
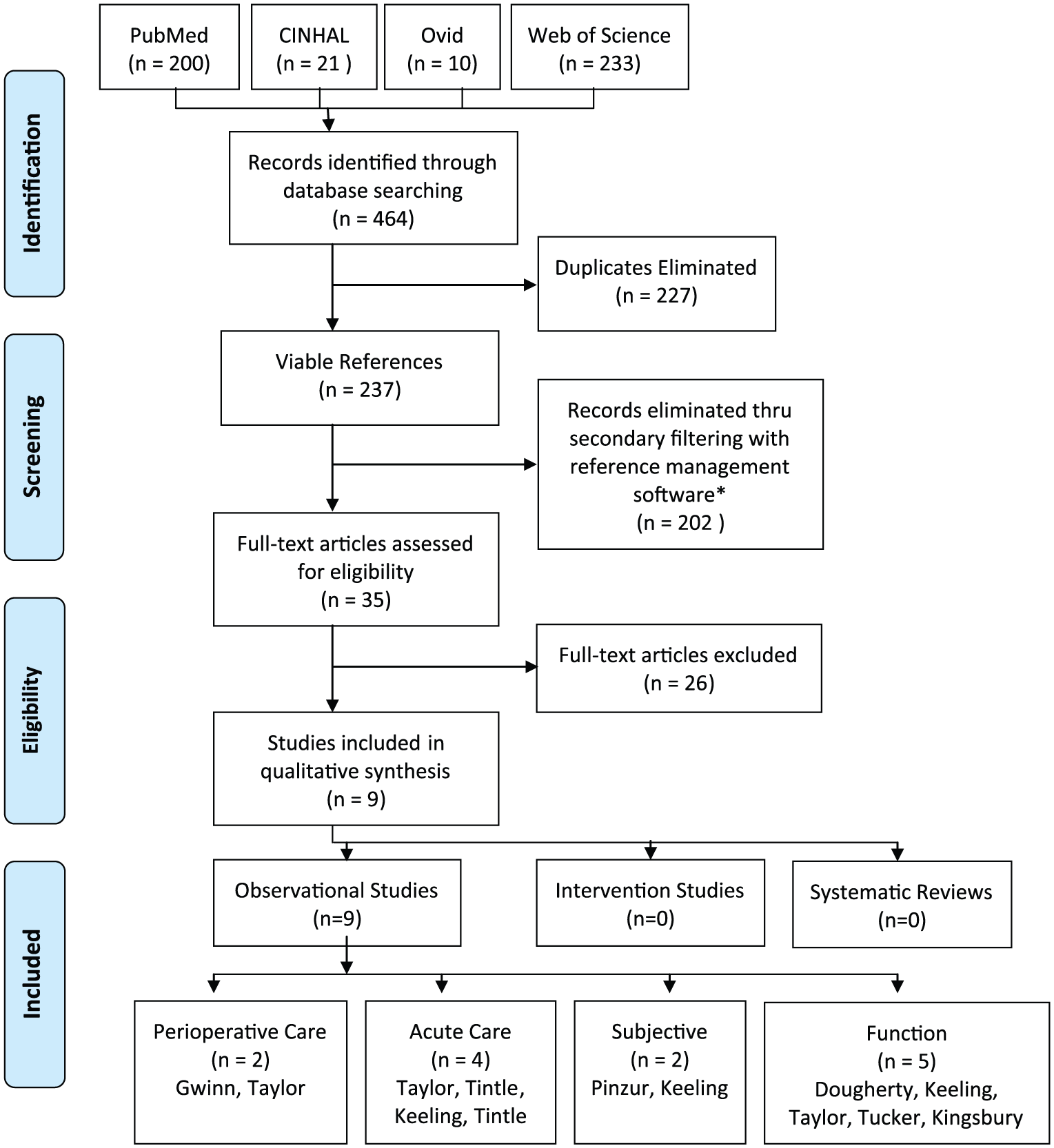
PRISMA flow diagram.
Article screening
To be included, articles had to
Include TTAs;
Compare Ertl or modified Ertl with alternative amputation surgical technique;
Describe one of the surgical techniques as bone bridge, Ertl, or osteomyoplastic;
Be a peer-reviewed journal publication;
Be about Adult subjects.
Articles were excluded, if they
Were any level of amputation beside TTA;
Did not explicitly define or provide data and conclusions regarding surgical technique;
Were non-peer reviewed article;
Were conference proceedings;
Included child subjects.
Articles were preliminarily sorted into study types using levels of evidence. Articles were screened for exclusion if classified as level IV or V (the lowest quality evidence) using the following initial criteria:
Case studies, case report, case series;
Non-human subject (i.e. material science, finite element studies);
Theses or dissertations;
Pediatric studies;
Technical notes;
Editorial style;
Procedure descriptions.
Quality assessment
Following the EndNote search using the aforementioned exclusion criteria, the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines were used to grade each study for methodological quality. Observational studies were identified in this review. These articles may guide clinical practice, as the highest quality contemporary evidence available is presented here. A quality assessment to report transparently of selective analysis or non-publication of results reveals what was planned, what was done, what was found, and what conclusions were drawn. Two investigators who independently screened the articles for a consensus on the STROBE scored the reviewed article.
Results
Following screening, full text articles were reviewed and sorted into the following relevant topics: Perioperative care, Acute care, Subjective analysis, and function. Following database searches and elimination of duplicates via Endnote X6 software, 31 articles were identified. Four additional articles were obtained via manual literature search, giving a total of 35 articles. Following STROBE grading and screening, nine articles were identified to be pertinent to one of the topics. Two articles included methodology that was applied to multiple topics. Two articles were sorted into the Perioperative care topic,11,12 four articles sorted into the Acute care topic,12–15 two articles into the Subjective analysis topic,15,16 and five articles into the Function topic.12,15,17 –19 Data are summarized in Table 2. A total of 585 subjects were examined collectively; 368 subjects enrolled as controls (traditional non–bone bridge amputation), whereas 217 subjects enrolled as having received a bone bridge technique. There was no reported attrition collectively among this body of evidence, where 585 total subjects enrolled and all completed the studies. Collectively, subjects’ mean age ranged from 23 to 53.6 years, with one author not reporting age. A functional level of K3–4 was reported in only one study, while all other authors did not report functional level. Only 27 female subjects were reported in one study, while four studies did not report on gender. In total, 12 dysvascular subjects were reported in one study, while all other studies reported trauma as the cause of amputation. The follow-up range was a wide variance of 90 days to 28 years. STROBE scores ranged from 10 to 19, and the median STROBE score was 16 out of 22 possible. No high-quality (level I or II) evidence existed. The highest quality study represented level III evidence. Due to a lack of sufficient high-quality studies and dissimilar analyses with of inconsistent outcome measures, meta-analyses were not possible.
Research data.
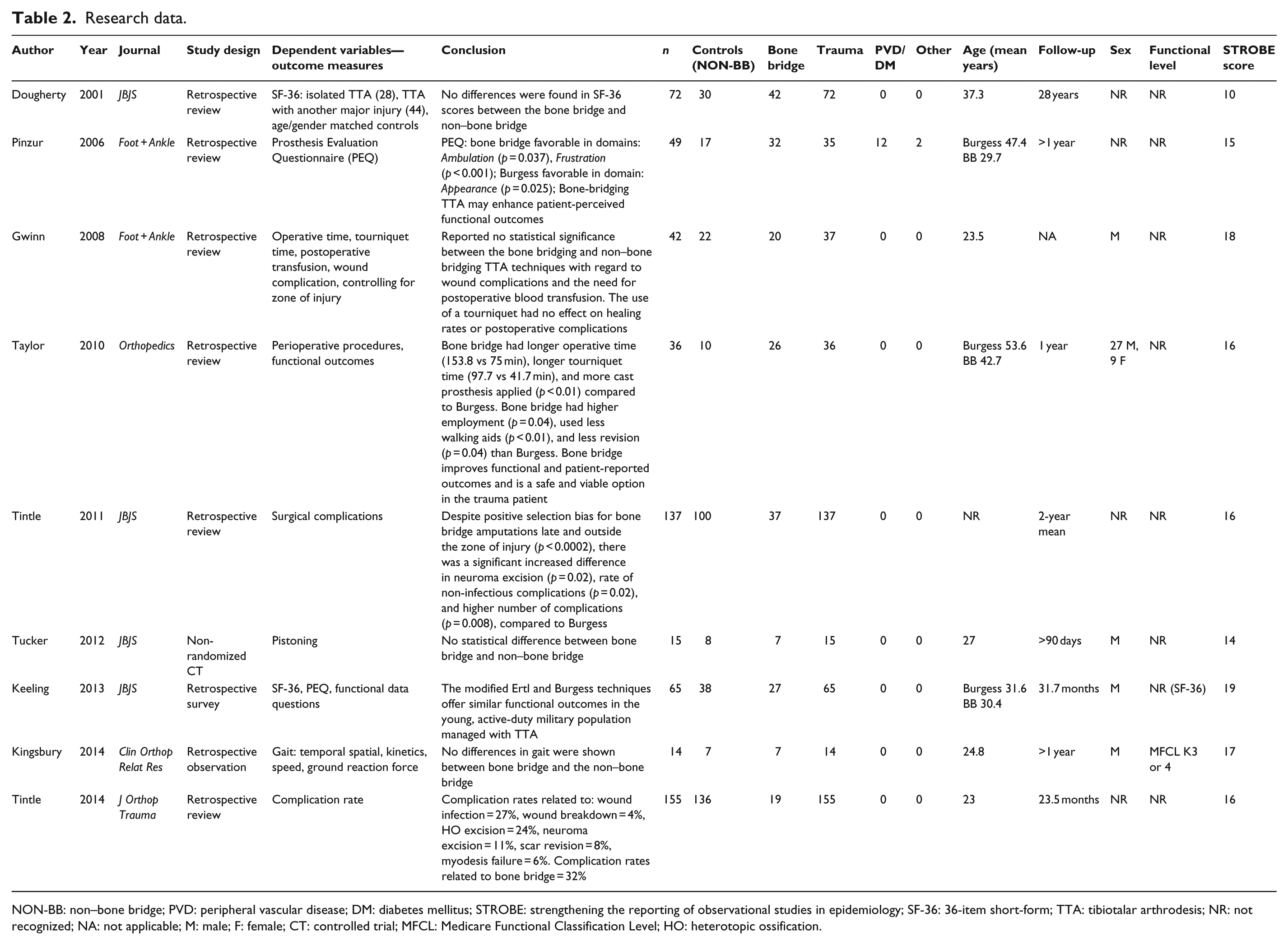
NON-BB: non–bone bridge; PVD: peripheral vascular disease; DM: diabetes mellitus; STROBE: strengthening the reporting of observational studies in epidemiology; SF-36: 36-item short-form; TTA: tibiotalar arthrodesis; NR: not recognized; NA: not applicable; M: male; F: female; CT: controlled trial; MFCL: Medicare Functional Classification Level; HO: heterotopic ossification.
Perioperative care
Gwinn et al. reported the preoperative differences between the bone bridging and non–bone bridging transtibial amputation in patients who sustained a wartime blast injury. Gwinn et al. reported an average age of 23.5 (19–36) years. Functional level and prosthesis accommodation of the subjects were not reported. Significant increase in mean operative time for the bone bridge technique compared to the non–bone bridge was 178 versus 112 min (p < 0.0005), respectively. The mean tourniquet time was 115 min in the bone bridge and 71 min in the non–bone bridge (p < 0.0005) subjects. 11 Taylor et al. reported an average age of 42.7 (18–77) years for the bone bridge and 53.6 (30–83) years for the non–bone bridge, although not reported as significant (p = 0.09). Time of injury to amputation was 1604 (5–13,870) days for the bone bridge versus 47.3 (0–322) days (p < 0.01) for the non–bone bridge. Again, mean operative time was significantly increased for the bone bridge technique compared to the non–bone bridge, 153.8 (136–187) min versus 75.8 (43–112) min, respectively. Also increased was mean tourniquet time for the bone bridge versus the non–bone bridge, 97.7 (65–131) min versus 41.7 (33–51) min, respectively. 12
Acute care
Additionally, Taylor et al. reported data in the acute care topic. A significant number of postoperative casts were applied in bone bridge (96%) versus non–bone bridge (30%) cases (p < 0.01). In total, 15% of bone bridge subjects required surgical revision versus 70% of the non–bone bridge subjects (p = 0.04). 12 Conversely, Tintle et al. reported on complication rates of bone bridge compared to non–bone bridge and found a statistically higher rate of complications related to the bone bridge (p = 0.02). Tintle et al. further reported complications specific to patients undergoing a bone bridge technique compared with a non–bone bridge transtibial amputation. Not reported was gender, age, or functional level. Follow-up time of 24 (9–48) months was reported. Additionally, Tintle et al. reported there were a total of 129 complications in 72 limbs (53%), leading to 222 re-operations. There were significantly more non-infectious complications in a bone bridge than the non–bone bridge subjects; 62% versus 49% (p = 0.02), respectively. Neuroma excision was more frequent in the bone bridge 30% compared with the non–bone bridge subjects 13% (p = 0.02). 13 In a latter report, Tintle et al. reported on combat-related re-operation complication rates in all levels of amputation. Regarding transtibial amputation, the indication for re-operation from bone bridge complications was 32%, while the indication for all other reasons for re-operations ranged from 6% to 27% and comprised the remaining 68% of re-operations required for amputation complications. 14 While the data of Keeling et al. most appropriately fits within the subjective analysis section, their anthropometric data bear consideration at or near the time of surgery and are thus included here. Reported RL length was significantly longer among the bone bridge than among the non–bone bridge subjects (164.5 ± 25 vs 139.6 ± 28.1 mm, respectively, p < 0.005). Delayed amputation was also reported as significantly greater for the bone bridge technique (18 vs 3 weeks, p < 0.005). 15
Subjective analysis
Pinzur et al. reported subjective analysis using the Prosthesis Evaluation Questionnaire (PEQ). Pinzur et al. reported an average age of 29.7 (15–74) years, while follow-up time was 16.3 months. Functional level was not reported. Bone bridge subjects scored the PEQ improved in the domains of Ambulation (p = 0.037) and Frustration (p < 0.001), while less favorable in the Appearance (p = 0.025) domain, than subjects receiving the non–bone bridge technique. Pinzur et al. reports the non–bone bridge group’s (n = 17) etiology as trauma, an average age of 47.4 (36–68) years, and highly functional prosthesis users. The average follow-up time was 14.7 years. The bone bridge group (n = 32) consisted of 18 traumas, 12 diabetic dysvasculars, and two others. 16 Keeling et al. also reported analysis using the PEQ. An average age of 30.4 (±6.9) years for the bone bridge technique and 31.6 (±7.3) for the non–bone bridge technique subjects were reported. No statistically significant differences in PEQ scores were reported between groups. 15
Function
Additionally, Keeling et al. reported function using the Short Form (SF)-36 and an ad hoc three-question survey. As with the PEQ scores, no statistically significant differences were found between groups in either the SF-36 or their ad hoc functional survey. 15 Dougherty et al. reported a 28-year follow-up to the Vietnam war primarily observing amputees with complications to those without. Reported were an average age of 48.4 years and a follow-up time of 28 (25–30) years. The bone bridge technique was performed on 68% of group one (no other major injury) and 52% of group two (TTA and a major injury). Dougherty 17 reported no significant difference between the bone bridge and non–bone bridge subjects in regard to SF-36 scores. Taylor et al. reported functional outcomes using the Sickness Impact Profile (SIP). The mean postoperative length of time until SIP overall scores was significantly improved 7.95 ± 3.18 in the bone bridge group and 15.18 ± 2.90 in the non–bone bridge group (p = 0.01). Statistically significant improvements were also seen in both the physical and psychosocial domains in the bone bridge group (p ⩽ 0.01, respectively). The SIP revealed significantly lower scores for the bone bridge group for the following categories: sleep and rest, work, ambulation, body care and movement, emotional behavior, and social interaction. In total, 15% of the bone bridge group used walking aids compared to 70% of the non–bone bridge subjects (p < 0.01). 12 Tucker et al. measured vertical limb displacement in the prosthesis. The mean age was 27 (22–33) years, all subjects were male and received an amputation as a result of trauma. Functional level and accommodation time were not reported. There were no significant differences between the bone bridge and non–bone bridge subjects. 18 Finally, Kingsbury et al. measured differences in gait, including spatiotemporal and kinetic parameters. In total, 14 subjects comprised the study, the median age was 23 years, and all subjects were high functioning with at least 23 months of use prior to follow-up with their prosthesis. No significant differences between the bone bridge and non–bone bridge groups were reported. 19
Discussion
We hypothesized that evidence may have been available to support improved distal weight bearing and reduced fibular movement when the tibia is bridged to fibula during amputation. Surprisingly, no high-quality studies substantiated either benefit presently. Two studies reported evidence in favor of the bone bridge compared to the non–bone bridge TTA, in the topics of Subjective analysis and Function (patient-reported functional outcomes).12,16 A favorable outcome is consistent with a large body of articles,5,20–27 not considered in this review due to the screening process; primarily because they were level IV and V case studies or reports. These reports add to the reported benefits of the bone bridge technique compared to the non–bone bridge technique. Conversely, two studies reported evidence in favor of the non–bone bridge technique compared to the bone bridge TTA. The same first author and similar co-investigators reported both studies.13,14 Both articles related to the Acute care topic of the amputation and more specifically complications as a result of the bone bridge technique. There is a small body of level IV and V evidence, 28 not considered in this review, which further supports the non–bone bridge technique. The remaining five studies reported across all four topic areas in this review identified the bone bridge as equivalent to the non–bone bridge technique.11,15,17–19
The studies compared in this systematic review were all level III evidence and primarily utilized survey instruments and retrospective data. There are no level I or II randomized prospective clinical trials. Little evidence is available comparing actual physical functional performance between these techniques. Furthermore, there are no studies comparing functional differences following successful bone bridge amputation to limb salvage or healthy controls. There is no agreed upon evidence to suggest that bone bridge would be contraindicated across any topic. Most studies examined in this review collectively concluded the need for more research. Specifically, a larger randomized, prospective study to help clarify when the bone bridge technique should be used when considering limb salvage or TTA would be beneficial.
Most studies reported the use of a “modified Ertl” technique, while many did not describe that technique. Knowing the exact technique used would be important to understanding the predictive success of the outcome. 29 There are reported benefits associated with the bone bridging transtibial amputation technique. Of these, creating a distal weight bearing surface through a bone bridge while stabilizing the fibula is primary.23,30 The potential benefit of a bone bridge is greater distal weight bearing and eliminating potentially painful fibular motion. The potential ability for a patient to end bear would be helpful in designing a prosthesis socket because the entire surface of the RL could be utilized for weight bearing. Gait and weight distribution symmetry could help prevent overuse to the contralateral limb of the prosthesis user.31,32 Furthermore, daily and chronic volume fluctuations may affect the quality of prosthesis comfort and use. During volume loss, it is crucial that the RL be able to tolerate the redistribution of pressure, particularly to the distal end, while not creating excessive pain or cause for skin breakdown. These are important potential benefits that should be prospectively explored, which have not yet been studied beyond case studies and reports. Data reported in the articles included in this review do not address the outcomes and effect of weight bearing, fibular stabilization, volume fluctuation, and physical functional performance. This leaves important benefits of the bone bridge technique to be determined.
Limitations of available evidence
This systematic review was limited as a level III SR because only observational and predominately retrospective (level III) evidence exists regarding bone bridge technique. Surgical technique studies present interesting challenges and can be difficult to conduct for several reasons. There are a variety of surgical techniques and skill-sets that are not equal or measurable. Unfamiliarity or loss of confidence can lead to defaulting to a technique specific to that surgeon’s skill set. Non-reporting on the elements of a procedure or technique limits our understanding when not fully described. Weak methodology, poor study design, and bias were consistent across most articles included in this systematic review. These elements can make conclusions misleading. Poor study design and bias were found regarding articles both for and against the bone bridge technique. Ultimately, lower STROBE scores encapsulate the limitations of each study. Only one study in this review was prospective, yet did not randomize or control for their main outcome, pistoning; most commonly attributed to suspension. 18 Future studies should include a prospective randomized design to include physical functional performance outcomes, postoperative care, and long-term prosthesis use. Superior functional outcome of prosthesis users may surpass that of limb salvage.
Conclusion
The bone bridge technique could provide a mechanistic advantage to the prosthesis user. The bone bridge technique is reported to increase tourniquet and surgical time. There is not agreement on acute complications related to a bone bridge technique. Perceptive measure of function reveals equivalence to improvements when subjects were amputated using the bone bridge technique. However, no actual physical functional performance measures corroborate subjective measures of improvement. There are no level I and II high-quality studies on the topic of bone bridge compared to a non–bone bridge technique. Level I and II evidence to answer primary research questions and benefit to the bone bridge technique need to be conducted in the future to establish clinical practice guidelines.
Footnotes
Acknowledgements
This original work is not being reviewed by any other journal and will not be submitted for publication in any other medical journal without written consent.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.