
Abstract
Background and aim:
Rotationplasty is an important and demanding challenge for physiotherapists. The aim of this paper is to describe the functional outcome achieved by a patient undergoing rotationplasty in adult age following osteosarcoma.
Case description and Methods:
The patient was followed throughout the rehabilitation course and the results achieved were recorded at 6, 9 and 12 months after surgery.
Findings and outcomes:
The results progressively improved in terms of function, functional performance and quality of life. The MSTS and TESS scales showed an improvement respectively of 20 and 23 percentage points, reaching levels of 80% and 87%. The quality of life perceived by the patient increased in the three assessments, the mental health score at one-year follow-up is higher than that expected for the population.
Conclusions:
Rotationplasty, even in adult age, produces good results and in the treatment of tumours in adults this operation should be taken into consideration.
Clinical relevance
Rotationplasty in adult age following osteosarcoma combined with a rehabilitation program enabled a patient to reach a successful outcome in terms of functional performance and quality of life.
Background
Rotationplasty was described for the first time in 1930 by Borggreve 1 to treat a shortening of the lower limb due to a tuberculosis infection in the knee. In 1975, Kristen et al. 2 introduced rotationplasty for the first time in the treatment of musculoskeletal system tumour in a patient with a recurrence of osteosarcoma in the distal femur. Surgical treatment consisted of removing the tumour while preserving the neurovascular bundle, the distal portion of the tibia and the foot. The tibia and foot were then turned 180° and attached to the salvaged portion of the distal femur. 2 From a functional point of view, the rotated ankle could also perform the tasks of the knee. Where it is not possible to salvage the lower limb, rotationplasty has an important role in treating osteosarcomas.3,4 Patients undergoing rotationplasty achieve satisfactory functional results compared with patients undergoing amputation and limb salvage treatment; 5 in some cases, it has also been possible to return to competitive sports.6,7 Several studies3,5,8–11 report the main results obtained from patients in terms of functional recovery, motor skills and quality of life. The target population of these studies is children and young adults where this surgery is performed more often. The role of the physical therapist is fundamental in the treatment and management of patients affected by osteosarcoma. 12 Shehadeh et al. 13 underline the importance of designing rehabilitation protocols for patients undergoing lower limb salvage to improve their outcome. For patients undergoing rotationplasty, there is little literature describing an adequate rehabilitation course; in particular, a description of this course in patients treated surgically in adult age is lacking. The following case report, based on our knowledge, is the first study that shows the functional outcome achieved by a patient undergoing rotationplasty in adult age following osteosarcoma and chemotherapy, describing the course and strategies of the rehabilitation treatment adopted.
Case description and method
The patient, a 31-year-old woman, complained of pain and swelling in the right thigh for about 8 years. A magnetic resonance imaging (MRI) performed in 2005 showed a solid, inhomogeneous growth in the distal femur. In 2012, a needle biopsy gave a negative outcome. A year later, the swelling was of large proportions in the middle-distal third of the thigh (Figure 1). A new biopsy enabled a diagnosis of dedifferentiated parosteal osteosarcoma of the right femur. X-rays of the chest were negative for metastases. In November of the same year, she underwent rotationplasty type A-I according to Winkelmann 14 (Figure 1). After surgery, the patient started chemotherapy with the combined administration of methotrexate, cisplatin and adriamycin according to the protocol in use at our institute 15 for a total of 18 cycles. The patient was followed directly throughout the rehabilitation course up to the ninth month during the periods of hospitalization for chemotherapy. At discharge, indications were given to continue treatment. According to the Italian legislation, the request from the ethical committee to carry out the present case report was not needed. The patient consented to publication of this report.
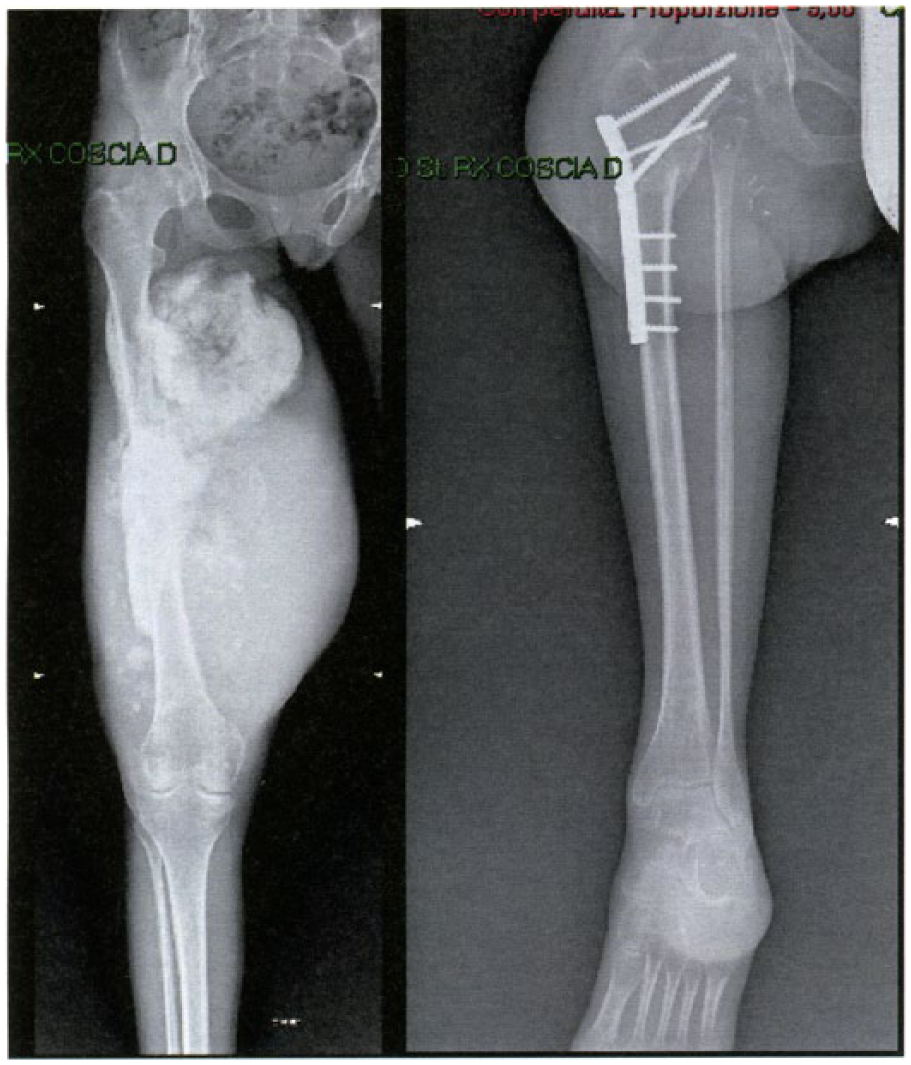
Pre- and post-surgery X-rays of rotationplasty.
The rehabilitation strategy
First phase: preparation for the use of the prosthesis
Active and passive mobilization of the ankle, within the limits of pain, started on the second post-operative day on the bed, in a supine position and with a small support under the ankle. The patient has been trained to change her position from supine to lateral while helping herself with a pillow between her legs. On the fourth day, a pelvis-thigh cast was applied with a Thomas splint to enable standing and walking exercises. Isometric exercises and some active mobilization have been gradually introduced using different positions: supine, on a side and static, to improve blood circulation, the joint mobility and the familiarity with the new knee. An effort to increase the walking resistance was made day after day through the ambulation exercises. At the time of discharge from hospital, on the 12th day, the patient could walk a short distance with the help of two forearm crutches and without load on the treated limb. When the cast was removed (23rd day), mobilization of the hip was begun. Within the range of free movement given by the hip joint, it was possible to perform some limb mobilization exercises in the supine, prone and sitting positions.
Second phase: use of the prosthesis with ischiatic support
The aim of temporary prosthesis with ischiatic support, worn in the fourth week, was to protect the femoral-tibial fixation and enable the start of training to use the prosthesis itself. The use of the prosthesis enabled the patient to test the mobility of the new knee through ambulation and allowed her to set a correct walking cycle. Muscular support exercises were practised by the patient both lying down and sitting up on the bed, wearing the prosthesis but also without it, paying specific attention to recovering the active extension of the new knee (Figure 2). By the eighth week, the patient complained of the onset of pain in the gluteal region and scar. Treatment with electro-analgesia and massage of the scar was effective at controlling and reducing the pain. Using the prosthesis and increasing the time spent standing during the day were probably the cause of the pain, which slightly slowed down functional recovery. By the 10th week, following the indication to increase the load, from partial (20%) to progressive, progressively more complex exercises were proposed with particular attention on controlling the new knee in the standing position (Figure 2). After 4 months, the patient could walk with the help of a single crutch while maintaining good postural control. Progressively, free walking is achieved with a slight compensatory inclination of the pelvis.
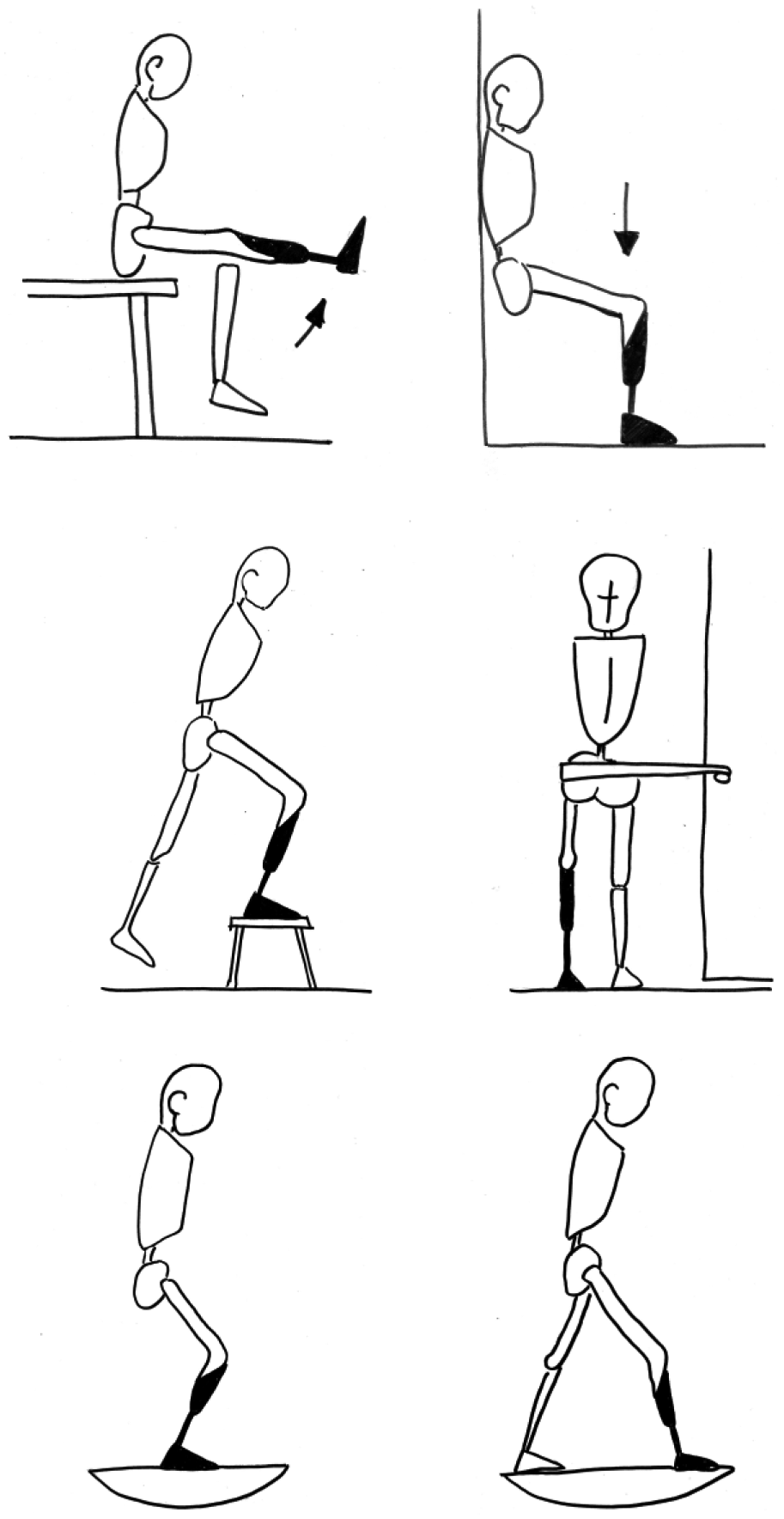
Strength, weight bearing and balance exercises.
Third phase: use of the prosthesis without ischiatic support
The 6-month radiographic follow-up showed that the prosthesis had been modified by removing the ischiatic support. The prosthesis that was used in this phase was still temporary, heavier and less comfortable, making the rehabilitation of the correct walking pattern more difficult. Only with a full-body recovery and with the elimination of the liquid excess at the end of the chemotherapy, it was possible to create the final prosthesis. At first, the patient presented a regression of performance and motor skills. This was accompanied by a feeling of soreness and fatigue around the new contact areas of the foot. Therefore, the two forearm crutches were used again to take some of the load off the limb and enable a more correct gait without deviations of the pelvis and trunk. In a short time (2–3 weeks), the patient was able to walk with one crutch. Free walking led again to the onset of compensations. Step ascending and descending revealed difficulties in controlling the knee in the final degrees of extension. In the descent phase, the healthy limb is moved forward, while the treated limb has difficulty controlling and slowing down the fall of the body forwards, thus producing a feeling of slight discomfort and insecurity in the patient. In the more advanced phase of treatment, rehabilitation training involved the use of the Wii Fit Balance Board. The patient received immediate visual feedback on her ability to distribute and control load on the lower limbs and therefore had to try and modify and adjust it to achieve the target required by the game.
Clinical outcome
The results achieved by the patient in first year were recorded at 6, 9 and 12 months after surgery. Function was measured by range of motion (ROM) 16 of the new knee and muscle strength 17 in the extension movement with the prosthesis worn in the sitting position. Functional recovery was recorded by the Musculoskeletal Tumour Society Score (MSTS), 18 the Toronto Extremity Salvage Score (TESS) 19 and some specific gait tests which described speed (10-m test), 20 strength (6-min walking test, 6mWT) 21 and balance (Timed up and go, TUG). 22 Short Form 36 (SF-36) scale was used to measure the quality of life. 23
Findings and outcomes
The results achieved are collected in Table 1 with regard to functional recovery and in Table 2 concerning health status as perceived by the patient. The results progressively improved in terms of function, functional performance and quality of life. The MSTS and TESS scales showed an improvement, respectively, of 20 and 23 percentage points, reaching levels of 80% and 87%, thus showing significant levels of autonomy for the patient. The results concerning the specific gait tests such as speed, strength and balance supported this trend. From the 6th to the 12th month gait speed, calculated using the 10-m test, increased by 0.3 m/s from 1 to 1.3 m/s. In particular, the TUG test which showed a deficit at 6 months had a marked improvement at only 9 months. Table 2 shows the results collected by administering the SF-36 scale. The quality of life perceived by the patient increased in the three assessments, although a differentiation is evident between physical recovery, which occurred after a longer time, and mental recovery, which started to improve immediately. One year after surgery, the item concerning limitations of the physical role showed a lower score (50 out of 100) when compared with the other items on the scale. The perceived health status was summarized in two indexes, physical and mental; the value of the mental health status of the patient was above the average perceived of the population with the same demographic characteristics.
Comparison of the functional results at 1 year with the literature data for patients with rotationplasty.
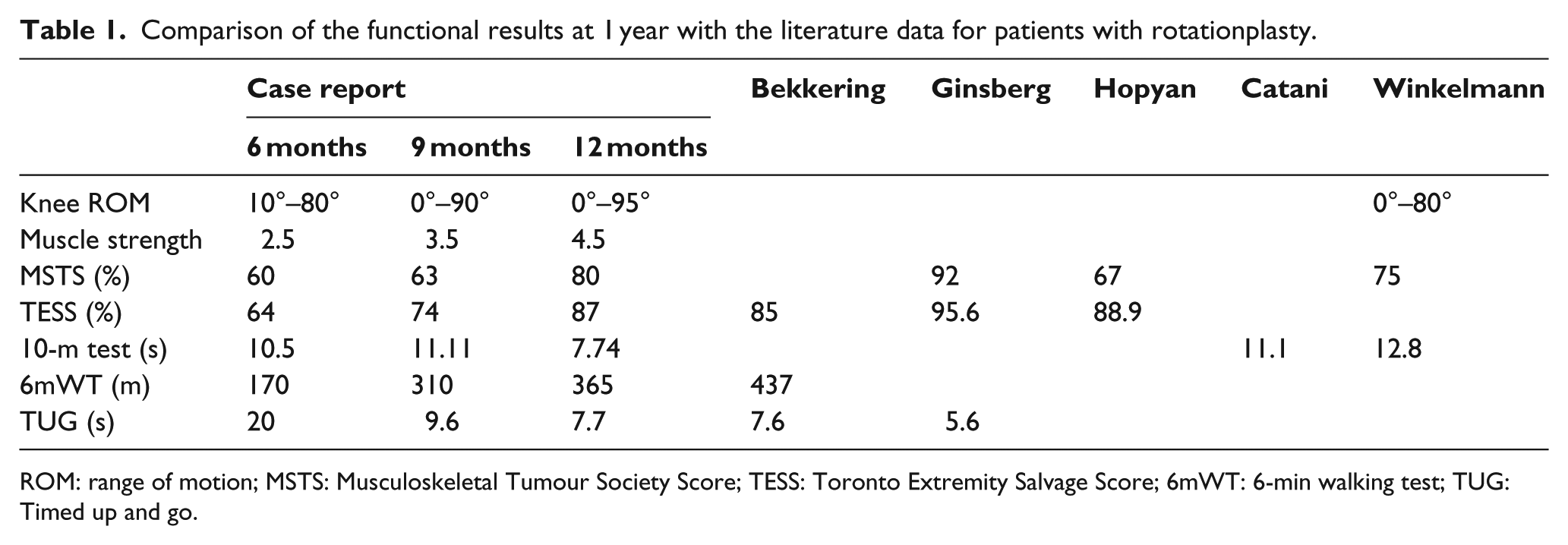
ROM: range of motion; MSTS: Musculoskeletal Tumour Society Score; TESS: Toronto Extremity Salvage Score; 6mWT: 6-min walking test; TUG: Timed up and go.
Comparison of the quality of life at 1 year with the literature data for patients with rotationplasty.
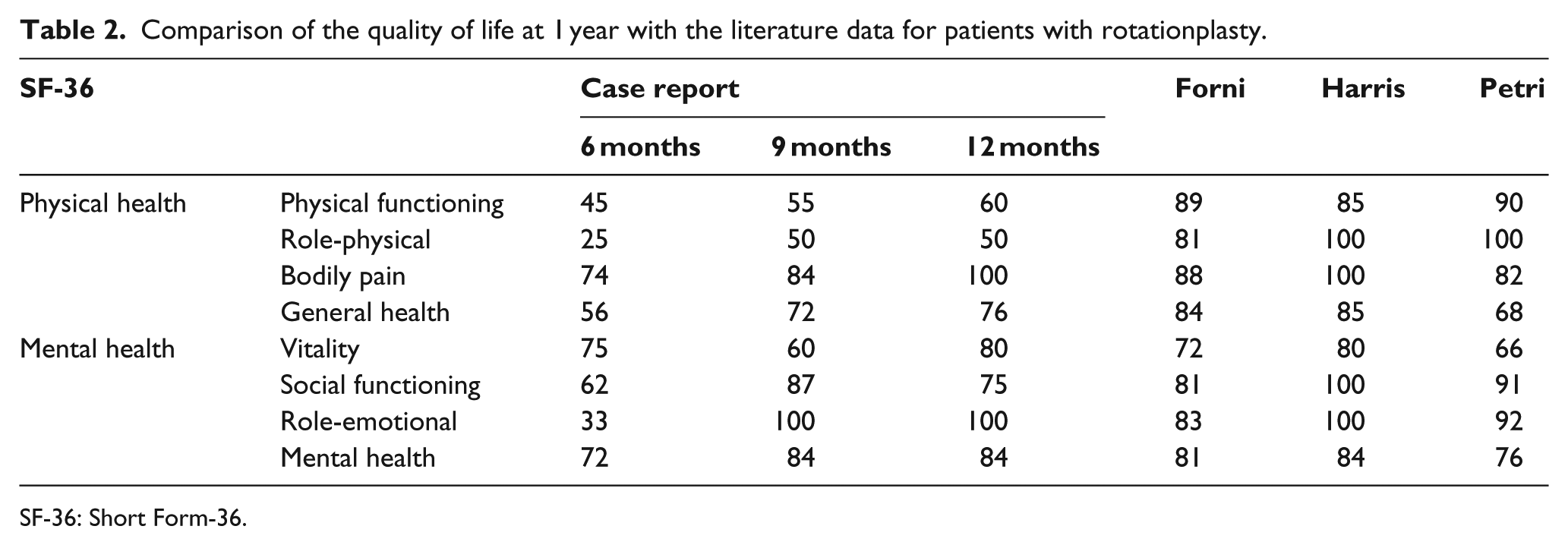
SF-36: Short Form-36.
Discussion
Rotationplasty is a rare surgical treatment, especially in patients of adult age, but at the same time, from a rehabilitation point of view, it is an important and demanding challenge. The post-op rehab programme in patients affected by bone tumour is particularly long and complex, with the need to adapt continuously to the patient’s conditions.12–13 The chemotherapy treatment influenced both the patient’s general physical recovery, by producing a feeling of tiredness, and the speed for allowing load on the limb. Exploiting the ankle joint to replace the knee was the central aspect of the physiotherapy treatment. The proprioceptive training programme was chosen according to the motor skills achieved, physical condition of the patient and the limitation of load imposed by the surgeon, and aimed at putting the neuromotor control ability of the new knee constantly under stress. The ankle joint, also in adult patients, can change its function and adapt to new loads. The 1-year follow-up in this study is surely too short a period to have a full understanding of the mid-long-term outcomes, but it helps to understand the role of the rehab programme in the initial post-op period. The results obtained from the patient studied and treated in adult age generally match those published in the literature where the population studied consisted of children and young adults3,5,8,10,11 (Table 1). The result produced by the 6mWT was the one that differed most from the findings presented by Bekkering et al. 8 The 6mWT is a test that mainly examines the strength of the gait. From this point of view, in the case report shown, performing the assessment before finishing the course of chemotherapy after only 3 months might have been a key factor for the effect of more fatigue that chemotherapy produces. To support this hypothesis, it can be seen that in the patient studied the time of 7.7 s to walk a short distance (10 m) was better than the times published by other authors which were 12.8 and 11.1 s in studies by Winkelmann 3 and Catani et al., 11 respectively. It was precisely Catani et al. 11 who highlighted how, from a biomechanical and functional point of view, rotationplasty can be an acceptable operation that offers a coordinated and harmonious gait. Looking at the results, the same results can be achieved in the adult patient. The quality-of-life assessment using the SF-36 scale showed a difference between the physical and mental recovery. Although an improvement was perceived in both mental and physical health status, that of the physical health status was still worse 1 year after surgery than that reported in the literature7,9,13 (Table 2). If perceived mental and physical health indexes are compared with the average values expected for a population with similar age and sex characteristics, it can be seen how items such as vitality, social activity and limitations in the emotional and psychological role that defines mental health indicators (MHI) showed above-average values. Rotationplasty is well accepted by the patient even in adult age. Items such as physical activity, limitations in the physical role, physical pain and general health that form physical health indicators (PHI) show a marked difference. According to the present authors, this finding is connected to several factors. The short follow-up and the very long chemotherapy treatment are certainly elements that impaired physical recovery as also found in the 6mWT. The physical health status scores of patients undergoing rotationplasty in the studies of other authors,7,9,13 where follow-up was longer, were higher. Therefore, we can hypothesize that at 1 year of follow-up, the patient still has some margin for improvement from a physical recovery point of view and that rehab treatment should be continued.
Conclusion
Rotationplasty is an operation that even in adult age produces good results that can be compared with those of a population of young patients. In the treatment of tumours in adults, this operation should be taken into consideration. The rehabilitation programme should be continued over a long period of time to minimize functional deficit and improve quality of life.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.