
Abstract
Background:
Limited information is available concerning the effects of prosthetic foot components on energy costs and ambulatory performance for transfemoral amputees.
Objectives:
Compare energy costs (VO2; gait economy) and ambulatory performance (self-selected walking speeds, self-selected running speeds, peak running speeds) differences during walking and running for transfemoral amputees and matched, non-amputee runners.
Study design:
Repeated measures.
Methods:
Transfemoral amputees were accommodated and tested with three prosthetic feet: conventional foot, solid-ankle cushioned heel (SACH); energy storing and return foot, Renegade; and running-specific energy storing and return foot, Nitro.
Results:
During walking, VO2 was similar between transfemoral amputees but was increased compared to controls. Self-selected walking speeds were slower for SACH compared to Renegade and Nitro. For transfemoral amputees, gait economy was decreased and self-selected walking speeds were slower compared to controls. During fixed running speeds, transfemoral amputees ran using Nitro, and VO2 was greater compared to controls. Transfemoral amputees ran at self-selected running speeds using Renegade and Nitro. Self-selected running speeds were slower for Renegade compared to Nitro. For transfemoral amputees, gait economy was decreased and self-selected running speeds were slower compared to controls. VO2 peak was similar between transfemoral amputees and controls, but controls achieved greater peak running speeds and % grade.
Conclusion:
Energy costs were greater and ambulatory performance was lower for transfemoral amputees compared to matched, non-amputee controls for all prosthetic foot conditions.
Clinical relevance
Both types of energy storing and return feet may improve walking performance for transfemoral amputees by providing faster self-selected walking speeds. For transfemoral amputees interested in performing vigorous running (exercise and running competition), clinicians should recommend a running-specific energy storing and return foot.
Background
For most studies, energy costs during ambulation for lower extremity amputees have been determined by measuring oxygen uptake (VO2) and/or gait economy (GE). GE (also called in some studies, gait efficiency) is determined as VO2 per meter traveled. Ambulatory performance for amputees has been reported by various gait velocity measures (self-selected walking speeds (SSWS), fastest possible or peak walking speed, self-selected running speeds (SSRS), and peak running speeds).
The energy costs (VO2) of walking for transfemoral amputees (TFA) due to non-vascular causes have been reported to be 30%–60% greater than non-amputee control subjects. 1 As walking speeds are increased, the relative difference in energy costs for TFA becomes more pronounced. 1 Additionally, SSWS are significantly slower for TFA than non-amputees. Studies have reported that SSWS for TFA2–5 range between 0.87 and 1.04 m s−1 compared to non-amputees whose SSWS range between 1.36 and 1.45 m s−1. 6 Thus, any prosthetic component that could improve energy costs and ambulatory performance would be functionally important to persons with TFA.
An important consideration in evaluating studies involving energy costs and ambulatory performance in amputees is the etiology of amputation. Waters et al. 7 have reported that energy costs (VO2 and GE) and walking performance (SSWS and fastest possible walking speeds) are significantly better in persons with TFA due to non-vascular causes compared to persons with TFA due to vascular causes. Two studies have compared the energy costs of walking for persons with TFA (due to non-vascular causes) using energy storing and return (ESAR) prosthetic feet compared to conventional prosthetic feet. Macfarlane et al. 8 compared the conventional solid-ankle cushioned heel (SACH) foot to the ESAR Flex-foot. They found that during walking at five fixed treadmill speeds, VO2 was lower and GE was improved for TFA using the ESAR Flex-foot compared to the conventional SACH foot. Graham et al. 9 compared the Multiflex foot, a composite foot classified as having a flexible keel, to the ESAR Vari-Flex foot. They found that during walking at fixed treadmill speeds, VO2 was lower for TFA using the ESAR Vari-Flex foot but VO2 was only significantly different at two of the eight walking speeds. A limitation of these studies8,9 was that no non-amputee, control subjects were evaluated. Thus, differences in energy costs during walking for TFA using these prosthetic feet components compared to non-amputees are not known.
Although some limited information is available concerning gait biomechanics10–12 during running for TFA, the energy costs of running for TFA have not been reported.
Since data concerning the effects of prosthetic components on energy costs and performance during walking for TFA compared to non-amputee controls are limited, and have not been reported for TFA during running, more research is warranted. Therefore, the primary purpose of this pilot study was to determine energy costs (VO2 and GE) and ambulatory performance (SSWS, SSRS, peak running speeds) differences during walking and running for TFA runners, using a conventional prosthetic foot and two types of ESAR prosthetic feet, compared to matched non-amputee runners. We hypothesized that the energy costs would be greater and ambulatory performance would be lower for TFA compared to matched, non-amputee controls for all prosthetic foot conditions. Nonetheless, our secondary purpose was to determine if various prosthetic foot components did improve energy costs and ambulatory performance for persons with TFA, in order to provide clinicians with research evidence to support recommendation/prescription of their use.
Methods
Subjects
Three male, unilateral, TFA runners with amputation due to non-vascular causes and three male, non-amputee control runners matched by age, physical characteristics, and physical activity levels were recruited for this study (Table 1). Participants were healthy, recreational runners who performed run training ⩾4 h week−1, for ⩾1 year and competed regularly in competitive running events. The study was conducted in accordance with ethical standards recommended by the Belmont Report. 13 The study protocol was approved by the University’s Institutional Review Board, and each study participant provided written informed consent.
Physical characteristics and peak performance responses of transfemoral amputees (TFA) and non-amputee controls.
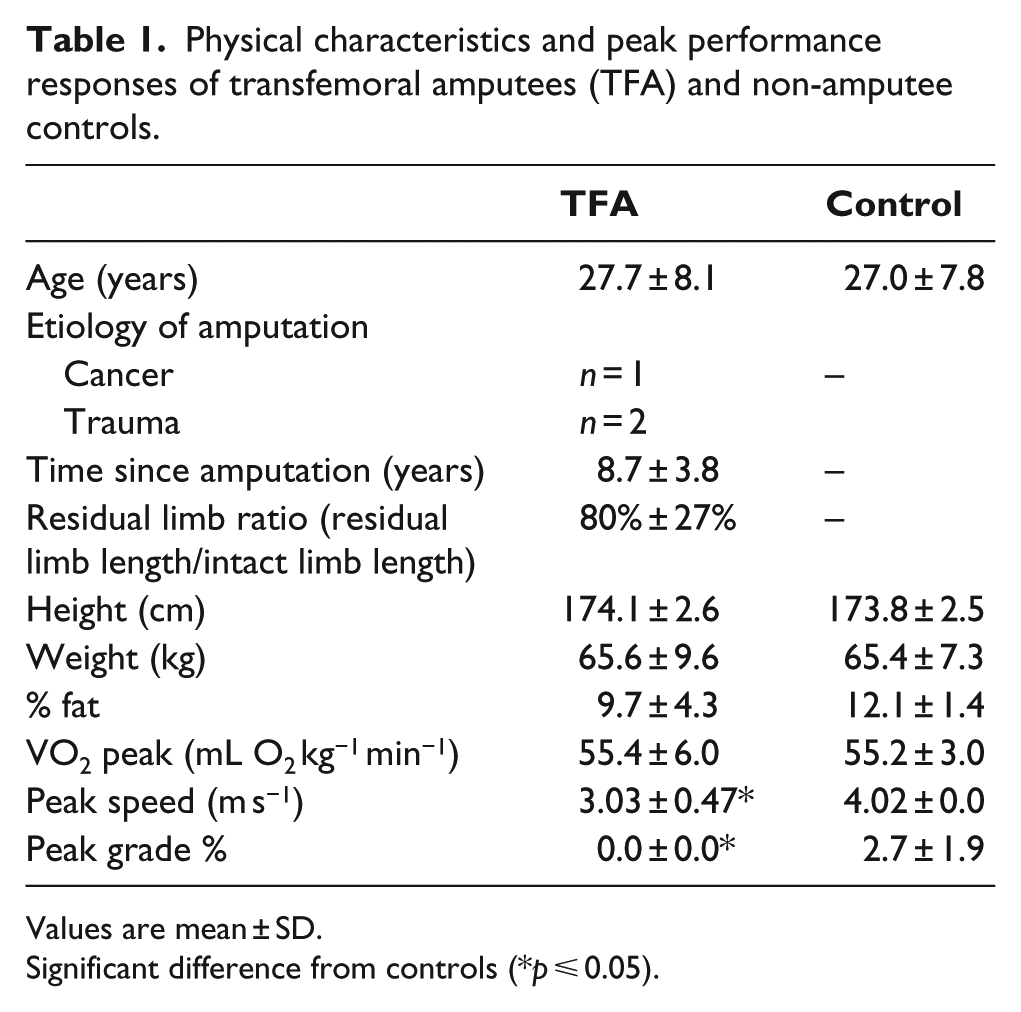
Values are mean ± SD.
Significant difference from controls (*p ⩽ 0.05).
Study design
The study utilized a repeated-measures design with case–control matching. Each TFA participant was tested with three prosthetic feet conditions: (1) conventional SACH foot (K08 SACH Strider®; Kingsley Manufacturing Co., Costa Mesa, CA, USA; Figure 1(a)), (2) general-purpose ESAR foot (Renegade®; Freedom Innovations, Irvine, CA, USA; Figure 1(b)), and (3) run-specific ESAR foot (Nitro®; Freedom Innovations; Figure 1(c)).
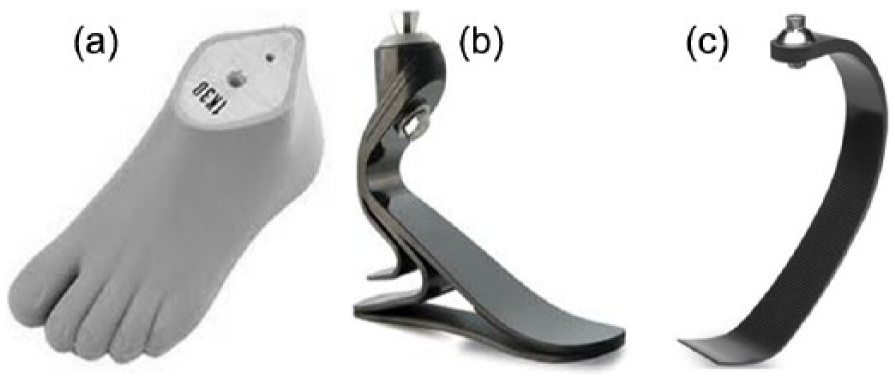
Three prosthetic feet conditions: (a) solid-ankle cushioned heel (SACH) foot, (b) general-purpose energy storing and return (ESAR) Renegade foot, and (c) run-specific ESAR Nitro foot.
The SACH foot is a conventional prosthetic foot which consists of a rigid keel (solid ankle) that terminates at a level that approximates the metatarsophalangeal joints. 14 It has a cushioned heel that provides passive plantarflexion in early stance and molded foam toes that allow the toes to passively hyperextend during late stance. A brief description of the general biomechanical principle of ESAR carbon fiber feet is that during initial-mid stance phases of gait, the prosthetic foot compresses and stores potential energy. During terminal stance, the prosthetic foot decompresses to its original shape, and the energy stored in the prosthetic foot is then returned to help propel the limb forward, effectively providing a push-off. 15 ESAR feet have multiple sub-types. One sub-type is a general-purpose walking and running foot, which incorporates a carbon fiber keel and ankle. 15 Another sub-type is a running-specific foot, which incorporates a carbon fiber, C-shaped keel, but is heel-less. 15
TFA participants had each prosthetic foot condition fitted to their usual running prosthesis by the study’s prosthetists (J.T.K. and M.J.H.). All TFA participants running prostheses utilized a mechanical hydraulic knee system (Total Knee 2100® (Ossur, Reykjavik, Iceland), n = 2; Mauch SNS® (Ossur), n = 1). TFA participants then accommodated to each prosthetic foot for a minimum of 2 weeks and performed a minimum of three of their usual exercise training sessions prior to testing. When TFA participants were interviewed to confirm their training and accommodation to each prosthetic foot condition they reported that when using the SACH foot during running they felt that it did not absorb impact well and that their residual limb often experienced pain sometimes for hours post exercise. Based on this information, the study researchers felt that there was risk of causing harm to the subjects and did not test the participants during running with the SACH foot.
To ensure the assignment of the order of testing for the three prosthetic feet conditions was balanced and randomized, a block randomization method was used.16,17
Exercise testing procedures
For exercise testing, participants reported to the laboratory in the morning following a minimum 8-h fasting period and had refrained from exercise approximately 48 h. Participants performed peak effort exercise testing for each test condition, using an incremental treadmill (Quinton TM65™; Cardiac Science, Waukesha, WI, USA) walking and running protocol. Testing began at 0.67 m s−1, 0% grade. Speed increased every 2 min, by 0.233 m s−1. If the participant was able to complete the running stage at 4.02 m s−1, 0% grade, then grade was increased by 2% for each additional stage until the participant reached his peak exercise tolerance. Approximately 48–72 h prior to exercise testing, participants came to the laboratory for a treadmill familiarization session. During the familiarization session, individual SSWS and SSRS were determined for each prosthetic foot condition for TFA and non-amputee control runners. The individual’s SSWS and SSRS were then programmed into their exercise test(s).
Measurements
The primary energy expenditure measurement for this study was oxygen uptake (VO2) measured continuously by breath-by-breath gas exchange analysis (Vmax Encore 229®; Care Fusion, Palm Springs, CA, USA). Calibration of the metabolic cart was performed immediately prior to testing according to manufacturer’s specifications. Flow volume measures were calibrated using a 3-L syringe, and gas analyzers were calibrated to known gas mixtures. For TFA, body weight measurements without their prosthesis were used for VO2 (mL O2 kg−1 min−1) measurements relative to body weight.
Because SSWS and SSRS are variable between subjects, a relative measure that integrates speed and energy costs is needed to determine GE. The criterion measure for GE is defined as energy expenditure per meter traveled and determined from the ratio of VO2 divided by ambulation speed (mL O2 kg−1 m−1). 18 Lower numerical values for GE signify better GE.
For TFA, body weight and body composition measurements were determined without their prosthesis. Percent body fat was determined using air displacement plethysmography, with measured thoracic gas volume (BOD POD GS®; COSMED, Rome, Italy).
Data analysis
Data were entered into a database and verified for accuracy, completeness, and normality. Paired samples t-tests were used to compare physical characteristics and peak performance responses between TFA and non-amputee control runners. VO2 and GE data were averaged over the final 20 s of each ambulatory speed.
During walking (at fixed speeds and SSWS), mean values for VO2 and GE were compared using a mixed model analysis of variance (ANOVA). A repeated-measures ANOVA was used for comparison of the three prosthetic feet conditions for the TFA group. A one-way ANOVA was used for the comparison of the non-amputee control runners to the TFA group’s three prosthetic feet conditions.
During running at fixed speeds, TFA used only the Nitro prosthetic foot, and mean values for VO2 and GE at each ambulatory speed were compared to non-amputee control runners using independent samples t-tests. During SSRS, TFA were able to use both the Renegade and Nitro prosthetic feet, and mean values for VO2 and GE were compared between feet conditions using paired samples t-tests. A one-way ANOVA was used for the comparison of the non-amputee control runners to the TFA group’s two prosthetic feet conditions.
It was expected that during running, TFA participants would have variable speed/stage end-points for peak exercise tolerance for each prosthetic foot condition. Thus, as higher speeds were attained, we expected some TFA participants would drop out, and there would be missing data for the TFA group for some prosthetic foot conditions. 19 We used the following intention-to-treat strategy for imputation of missing data. At any ambulatory speed/stage, where the number of TFA participants was less than three for a prosthetic foot condition, the mean value substitution method, 20 which is also referred to as the missing patient’s own group mean or MOWN technique, 21 was utilized. That is, the mean value for the available subjects was determined and imputed for the missing subject’s data points for that prosthetic foot condition. Statistical analyses were performed using SPSS software (Version 22, SPSS Inc., Chicago, IL, USA). For all procedures, statistical significance was p ⩽ 0.05. Values are reported as means ± standard deviation (SD).
Results
Table 1 compares physical characteristics and peak performance responses of TFA and non-amputee control runners. TFA were closely matched to non-amputee control runners in physical characteristics (age, height, weight, % fat). At peak exercise tolerance, TFA using the Nitro foot and non-amputee control runners achieved similar VO2 peak values, but non-amputee control runners achieved significantly greater peak running speeds (25%) and % grade (2.7%).
During exercise testing, TFA participants performed to their peak exercise tolerance for each prosthetic foot condition. TFA participants thus had variable end-points for each prosthetic foot condition. TFA participants completed all fixed walking speed stages and SSWS with each prosthetic foot condition. However, during any running condition (SSRS or fixed speed stages), no TFA participants ran with the SACH foot. During SSRS testing, two of three TFA participants were able to run using the Renegade foot, and three of three TFA participants were able to run using the Nitro foot. During running with fixed running speed stages, TFA participants only ran using the Nitro foot, as the fixed running speeds started at a faster speed than the TFA participants could run with utilizing the Renegade foot. All control subjects were able to run at and beyond 3.35 m s−1, whereas only two TFA participants could complete this stage/speed of the test while using the Nitro foot.
VO2 responses during fixed walking and running speeds
During walking at fixed speeds, mean (± SD) VO2 responses were similar between prosthetic feet conditions for TFA (Figure 2). However, VO2 was significantly greater for TFA with all prosthetic feet conditions compared to non-amputee controls: SACH, 45%–62% greater; Renegade, 49%–77% greater; and Nitro, 45%–78% greater.
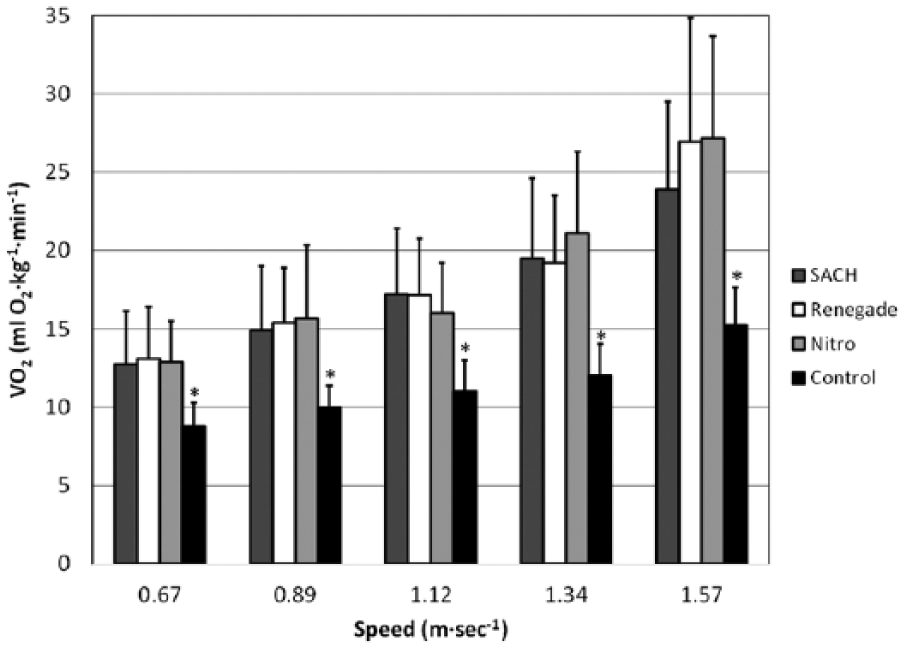
Oxygen uptake (VO2) responses (mean ± SD) during walking for transfemoral amputees (TFA) using three prosthetic feet conditions compared to non-amputee controls.
During running at fixed speeds, VO2 was significantly greater (29%–34%) for TFA using the Nitro foot, at all speeds, compared to non-amputee controls (Figure 3).
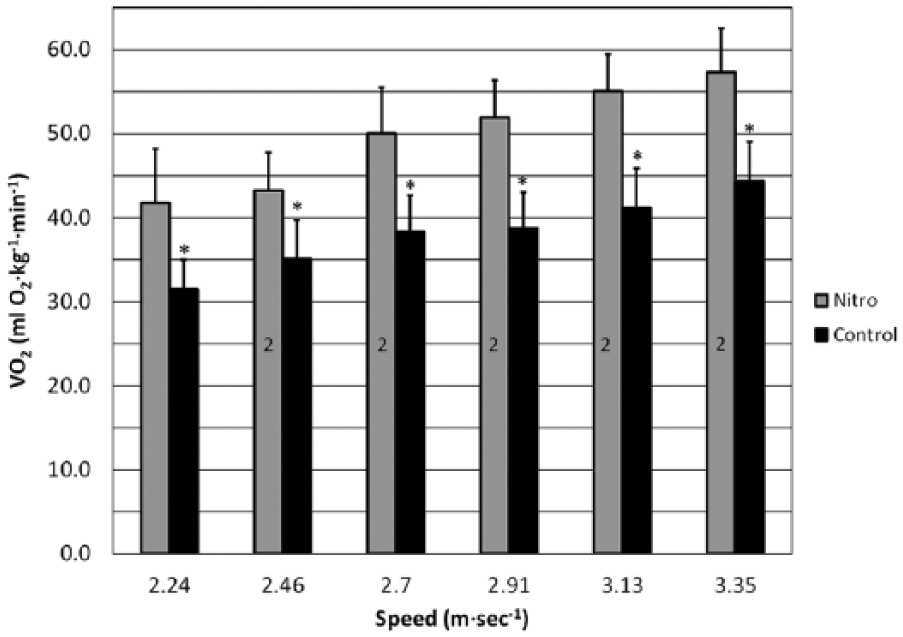
Oxygen uptake (VO2) responses (mean ± SD) during running for transfemoral amputees (TFA) using the Nitro prosthetic foot compared to non-amputee controls.
GE during self-selected walking and running speeds
At SSWS, GE was similar between prosthetic feet conditions for TFA (Figure 4). However, for TFA, mean GE values were significantly higher (i.e. reduced GE) for all prosthetic feet conditions for TFA (SACH, 47%; Renegade, 59%; Nitro, 47%) compared to non-amputee controls. SSWS were significantly slower for the SACH foot compared to Renegade and Nitro feet (7% and 9%, respectively). Additionally, SSWS for all prosthetic feet conditions were significantly slower for TFA (SACH, 29%; Renegade, 24%; Nitro, 23%) than non-amputee controls.
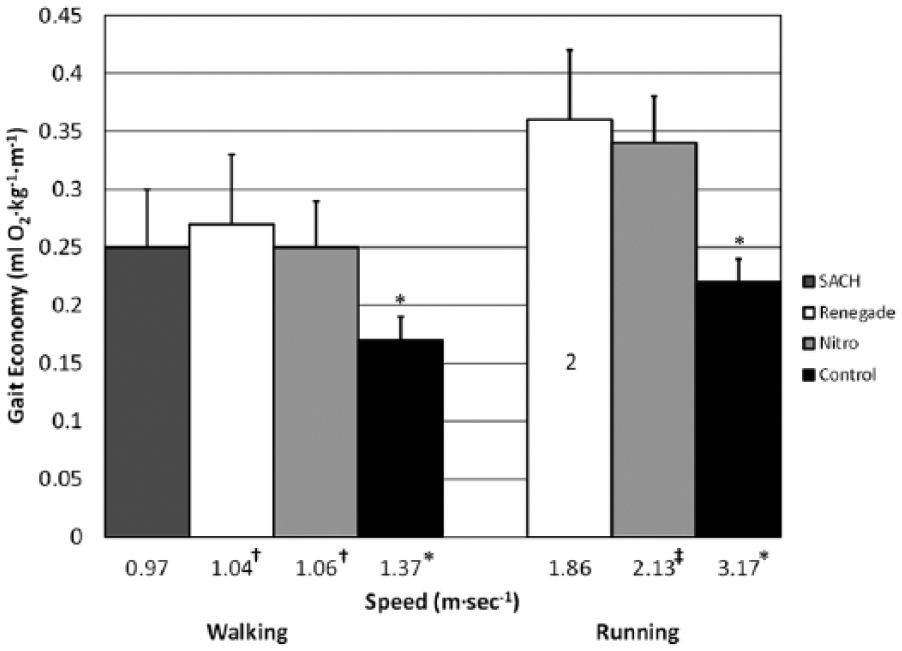
Gait economy (mL O2 kg−1 m−1) at self-selected walking and running speeds (SSWS and SSRS) for transfemoral amputees (TFA) using three prosthetic feet conditions compared to non-amputee controls.
At SSRS, GE was similar for TFA using Renegade compared to Nitro (Figure 4). However, for TFA mean GE values were significantly higher (i.e. reduced GE) for TFA (Renegade, 64%; Nitro, 55%) compared to non-amputee controls. SSRS were significantly slower for the Renegade foot (13%) compared to the Nitro foot. Similar to SSWS, SSRS were significantly slower for TFA (Renegade, 42%; Nitro, 33%) than non-amputee controls.
Discussion
During walking for TFA, at both fixed speeds and SSWS, no significant differences were observed for energy costs (VO2 and GE) between the three prosthetic feet conditions. However, TFA demonstrated significantly increased VO2 and decreased GE compared to non-amputee controls. At SSWS, TFA demonstrated significantly improved speed with the Renegade and Nitro compared to the SACH (7% and 9%, respectively), but SSWS for TFA were significantly slower for all feet conditions compared to non-amputee controls. These results during walking for TFA compared to non-amputee controls were similar to what we reported for transtibial amputee (TTA) runners compared to non-amputee controls. 22 For TFA, the increase in VO2 compared to controls ranged from 45% to 78%, whereas for TTA the difference was smaller and ranged from 21% to 33% (Table 2). Compared to controls, SSWS for TFA were 23%–29% slower and TTA 16%–22% slower (Table 2).
Percent increase in oxygen uptake (VO2) and percent decrease in self-selected walking and running speeds for transfemoral amputees (this study) and transtibial amputees (Mengelkoch et al. 22 ) compared to matched, non-amputee control runners.
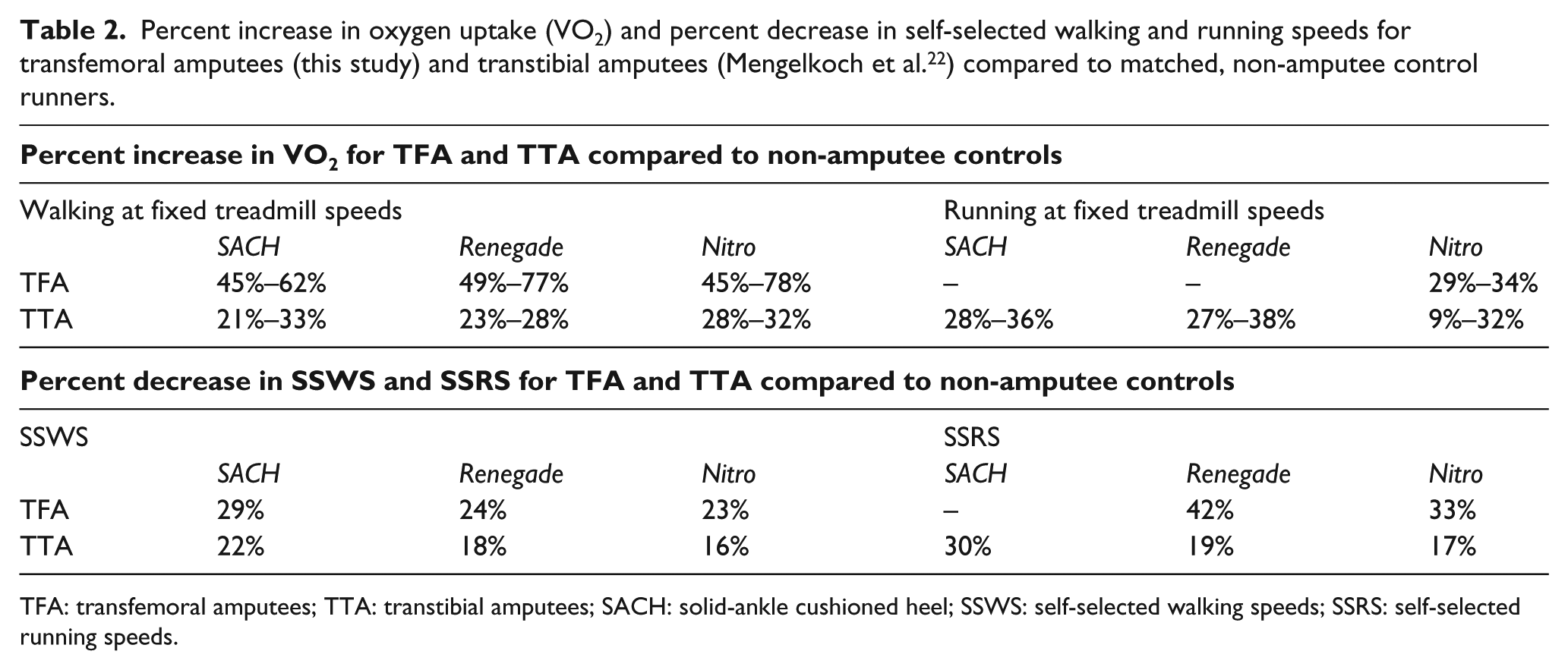
TFA: transfemoral amputees; TTA: transtibial amputees; SACH: solid-ankle cushioned heel; SSWS: self-selected walking speeds; SSRS: self-selected running speeds.
In our previous study, 22 we compared energy costs (VO2 and GE) and ambulatory performance (SSWS, SSRS, peak running speeds) during walking and running for TTA runners and matched non-amputee control runners using the same study design. In our previous study, 22 the aerobic capacities (VO2 peak) of TTA (51.6 ± 7.8 mL O2 kg−1 min−1) and controls (50.7 ± 9.3 mL O2 kg−1 min−1) were similar, but slightly less (approximately 7%) than the participants in this study (TFA, 55.4 ± 6.0 mL O2 kg−1 min−1; controls, 55.2 ± 3.2 mL O2 kg−1 min−1). These data indicate that TFA, TTA, and non-amputee control participants in both studies were well-matched and well-trained recreational runners, and reasonable comparisons might be made between studies.
The data in this study demonstrating significant increased VO2 during walking for TFA are in agreement with the early study by Genin et al. 1 which reported that compared to non-amputee control subjects, the VO2 of walking for TFA were much greater (30%–60%), and as walking speeds increased, the relative difference in VO2 for TFA becomes more pronounced.
The data in this study demonstrating that SSWS are significantly slower for TFA also agree well with the literature. Various studies have reported a range of SSWS for TFA between 0.87 and 1.04 m s−1.2–5 In this study, SSWS for the three feet conditions were as follows: SACH, 0.97 m s−1; Renegade, 1.04 m s−1; and Nitro, 1.06 m s−1. Additionally, the SSWS of the non-amputee controls in this study (1.37 m s−1) agree well with the range of SSWS reported for able-bodied, non-amputee subjects (1.36–1.45 m s−1). 6
To our knowledge, no study has provided information concerning the energy costs and ambulatory performance during running for TFA. As described in the “Methods” section, we determined that TFA were unable to safely and/or comfortably run using the conventional SACH foot. This differed from our previous study 22 in which two of three TTA participants were able to run at their SSRS and the slowest fixed running speed, using the SACH foot. It seems likely that the inability of TFA to safely utilize the SACH foot during running was due to the combination of the poor energy-absorbing characteristics of the SACH foot and the loss of the knee joint and distal muscles to absorb the increased forces during running. We suggest that for TFA interested in engaging in running activities, the SACH foot should not be recommended/prescribed. Additionally, in this study, only two of three TFA participants were able to run at their SSRS using the general-purpose ESAR Renegade foot. At SSRS, GE was similar for TFA using Renegade compared to Nitro. However, for TFA, the trade-off in performance was that SSRS were significantly slower using the Renegade foot (13%) compared to the Nitro foot.
During running with fixed running speed stages, TFA participants only ran using the Nitro foot, as the fixed running speeds started at a faster speed than the TFA participants’ SSRS with the Renegade foot. The inability of TFA to effectively utilize the Renegade foot for running also differed from our previous study 22 in which TTA participants were able to run at high running speeds (3.13–3.35 ms−1) using the Renegade foot. Similar to our previous study 22 with TTA runners, we observed that TFA runners using the run-specific ESAR Nitro foot expended significantly more energy in terms of VO2 at every speed and ran slower at VO2 peak than closely matched non-amputee control runners. Interestingly, unlike walking, where TFA demonstrated approximately 2× greater VO2 than TTA, the high end of the range of the increase in VO2 during running using the Nitro foot was relatively similar between TFA (34%) and TTA (32%) (Table 2). As seen in Table 2, the magnitude of the range of the percent decrease in SSRS for TFA compared to TTA (TFA, 33%–42%; TTA, 17%–19%) was more pronounced than their differences in SSWS (TFA, 23%–29%; TTA, 16%–22%). A final functional difference in running for TFA runners in this study compared to TTA runners in our previous study 22 was that mean peak running speed at VO2 peak was approximately 10% slower (TFA 3.03 ± 0.47 m s−1 and TTA 3.35 ± 0.22 m s−1) even though mean aerobic capacity was slightly higher for the TFA runners. Together, this information provides further evidence that as the level of lower limb amputation goes higher, energy costs increase and functional walking and running performance declines, regardless of prosthetic foot interventions.
Study limitations
The primary limitation for this pilot study was sample size. It was difficult to recruit TFA participants who met the relatively high level of training for our study’s inclusion criteria. However, our study design utilized case–control matching with repeated measures which is a well-accepted methodological approach to studying rare conditions, that is, in this case well-conditioned TFA runners.23–25
Conclusion
Our hypothesis that energy costs would be greater (i.e. increased VO2 and decreased GE) and ambulatory performance would be lower (i.e. SSWS, SSRS, peak running speeds) for TFA compared to matched, non-amputee controls for all prosthetic foot conditions was supported. Clinically, our data suggest that for TFA walking on level surfaces, energy costs (VO2 and GE) are mostly similar between prosthetic feet conditions, but both types of ESAR feet may improve walking performance as they likely provide faster SSWS. For running recommendations, the SACH foot does not appear to adequately support running activities for TFA. However, both types of ESAR feet appear to provide TFA at least some potential for running on level surfaces. The general-purpose ESAR foot appeared to support running speeds up to SSRS and thus would be suitable for some recreational activities and assessing a TFA’s capacity to run. For TFA interested in performing more vigorous, distance-type running (i.e. for exercise and running competition), clinicians should recommend and prescribe a run-specific ESAR foot, as only a run-specific ESAR foot appeared to provide adequate running function at and above SSRS. Although distance-type running performance was relatively improved for both TFA and TTA 22 using the run-specific ESAR foot, energy costs were increased at all speeds and peak running speeds and SSRS were slower for TFA and TTA 22 when compared to non-amputee controls.
Footnotes
Acknowledgements
The authors wish to thank Freedom Innovations, Irvine, CA, for providing the Renegade and Nitro prosthetic feet for the study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the University of South Florida’s Signature Interdisciplinary Program in Cardiovascular Research Award (#10009-614101).