
Abstract
Background and aim:
Clients’ acceptance and adherence with orthoses can be influenced by a clinician’s communication skills. In this clinical note, we describe two communication techniques, in the context of therapeutic footwear.
Technique:
Person-centred communication involves engaging with and listening to the attitudes of the client towards their condition, as well as discussing acceptance and expectations, in a structured consultation. Building a relationship is crucial and requires clients to feel heard and understood. An important influence on the acceptance and adherence is that a client makes a conscious decision to receive their device. This active receipt can be facilitated through shared decision making, wherein clinicians give clear, relevant and meaningful examples, based on clinical evidence, and ensure this is understood.
Discussion:
Two communication techniques for clinicians providing therapeutic footwear are described. These can be adapted for use with provision of other assistive technologies to improve client acceptance and adherence.
Clinical relevance
Small changes in how clinicians communicate to their clients in daily practice can have a big influence on the subsequent acceptance and adherence with therapeutic footwear and indeed other prescribed assistive technologies.
Keywords
Background and aim
When a client chooses not to wear technically sound therapeutic footwear, the opportunity for achieving the maximum potential for good health and mobility is lost; such footwear may end up in the cupboard.1–4
Perhaps the most important reason for not adhering with therapeutic footwear is a lack of acceptance.5,6 This acceptance may concern the client’s acceptance of their condition; if the underlying illness is not accepted, the footwear will not be accepted. Or acceptance may concern the client’s need for therapeutic footwear; footwear is a normal part of someone’s identity, and therapeutic footwear then replaces what is normally worn.5,6 An additional factor that influences adherence is how well the footwear actually meets a client’s expectations. In short, does the footwear look, fit, feel and deliver on the outcomes as the client had imagined? When expectations are not matched by the outcomes, a client is far less likely to adhere with their footwear. 7
These two factors – acceptance and expectations – cannot be easily seen or assessed during a client’s examination. Communication is needed for the provider to understand the client’s thoughts on both factors. The importance of communication is also realised from negative consequences such as non-adherence and dissatisfaction when clients feel they have not been listened to or understood by their provider.5,6,8–12
Similar to other core clinical skills, such as physical examination or analysis of biomechanics and gait patterns,8–11 communication requires learning and mastering techniques and putting them into practice. Compared to core skills needed to build therapeutic footwear, communication to improve acceptance and adherence of the footwear receives scant attention in both practice and research. The aim of this clinical note is to describe two techniques for improved communication, in the context of therapeutic footwear – person-centred communication and shared decision making.
Technique
Technique 1: person-centred communication applied to the footwear provision process
The main feature of person-centred communication is involving the client in all steps of the process of therapeutic footwear provision. This integration can be achieved through a structured consultation model, organised as per Figure 1.13,14 Involving the client is not simply asking what colour or style of footwear they prefer. Rather, involvement is fundamental to the service, through engaging with and hearing the attitudes of the client to their condition, and to their experiences with their body no longer functioning as they would like it to.5,6
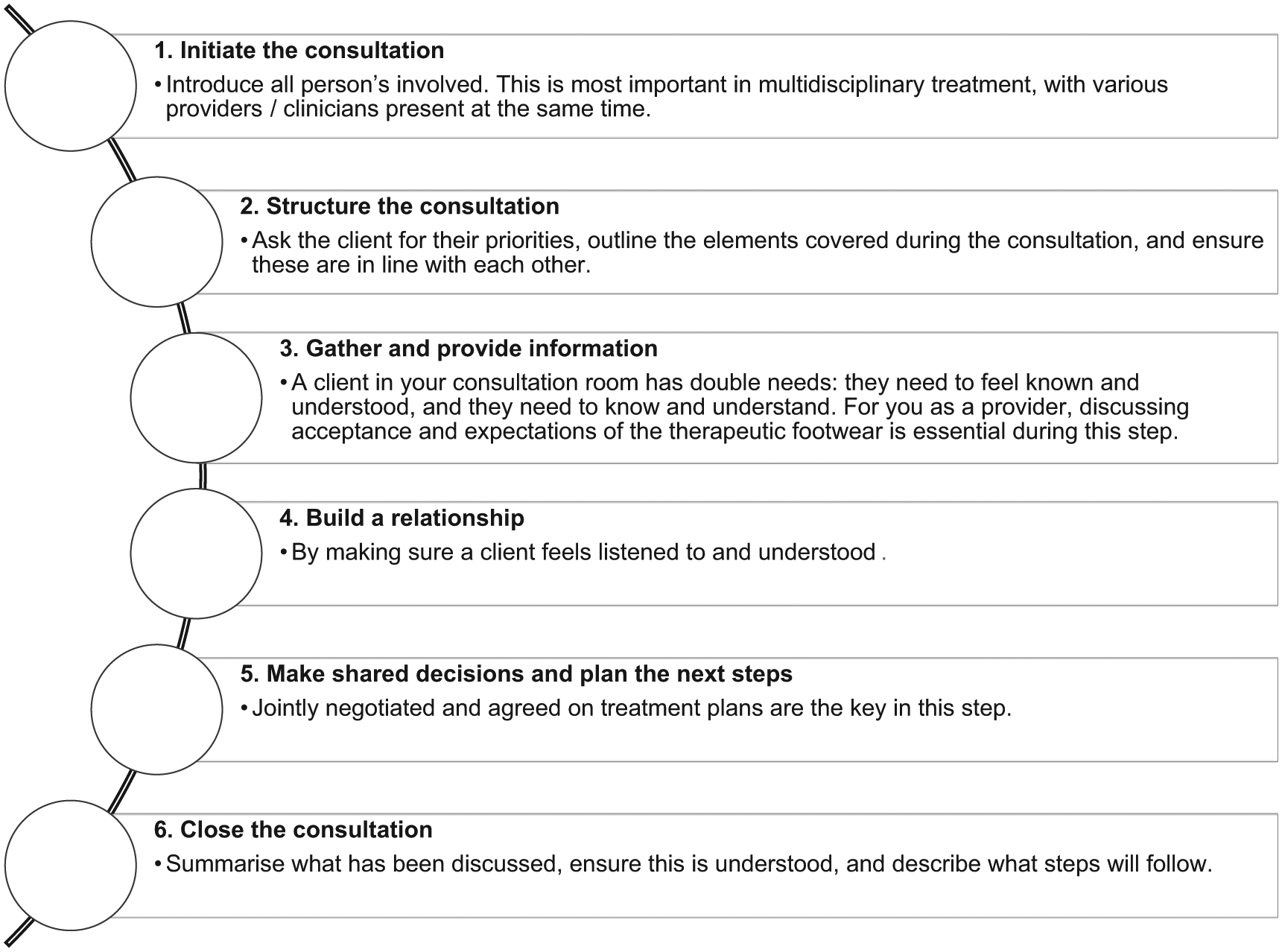
Elements of a structured footwear provision consultation to support shared decision making in the provision of therapeutic footwear.
Building a relationship is crucial in person-centred communication. To ensure a client feels listened to and understood, it is important to relate back to the patient a summary of they have said to you. Another important part of building the relationship is to avoid negative emotional language. As an example, a provider may describe the foot of someone with rheumatoid arthritis as being ‘difficult’. This can impart a feeling of guilt or shame from the client towards their feet or towards the extra work required by the clinician for their care. 6 This negative communication breaks down the client–provider relationship and removes opportunities for the client to have a voice on any part of the prescription process. 6
Technique 2: shared decision making applied to the footwear provision process
The second technique is shared decision making, which largely comes in at step 5 in the structured consultation (Figure 1). This can be described as the clinician and client working together towards best health care choices and is the intersection between evidence-based medicine and person-centred communication.15–17 When applied to the process of footwear provision, shared decision making means that provision should not continue until the client has confirmed they are actively choosing the therapeutic footwear, rather than passively receiving them (and subsequently not wearing them).
A condition for shared decision making is a real understanding of the disorder and the intervention by the client. This requires providers to give clear, relevant and meaningful clinical evidence to inform the client. 18 Information provision involves explaining the disorder, the treatment goals and options, and the available clinical evidence supporting the options, without the use of emotional language or medical jargon.
An understanding of the disorder may be clear to the provider, but they also need to be certain it is understood by the client receiving the footwear. For example, a provider may state ‘15 in every 100 people with diabetes will experience a foot ulcer’. A client’s understanding of what this information means to them remains unclear unless you ask an essential follow-up question: ‘in your own words, can you tell me what this means to you?’15–18 This questioning is an important tool in shared decision making and ensures that the focus is on the client’s understanding of the information provided.
The use of visualisation tools such as option grids can also assist in the decision making process and may be particularly useful at low levels of health literacy. The previous statement can be easily pictured with 100 people, of which 15 are coloured differently to indicate those with a foot ulceration.
Ensuring a clinical explanation is understood by the client cannot be overemphasised. A qualitative study of people’s expectations of footwear identified a person with diabetes who needed therapeutic footwear after a foot ulcer. 19 The clinician had assumed at that stage that the client understood what the footwear would be for. However, the client’s confusion was clear: ‘Well, the doctor seriously just kept talking, saying it is to protect your feet. I was left wondering, to protect them from what?’ 19 As such, the assumed knowledge, and poor communication, threatened the person’s foot health.
Discussion
Communication is part of every waking hour of every day. However, this does not necessarily make us experts in communication. When we communicate in specialised settings, such as therapeutic footwear provision, communication is a skill that needs practice and adjustment to the audience. The requirements for communication during this process have changed over the last decade. This is a consequence of the increasing importance of evidence-based medicine and shared decision making and also of the change towards user-oriented provision of assistive technologies; rather than treating a specific disorder, it is often a client’s goals that determine treatment needs.
The process of providing therapeutic footwear has been used as an example for this clinical note as the importance of communication is well exemplified in this sector, with increasing clinical evidence.3,5–9,12 However, the techniques described here likely apply equally well for provision of other orthoses and indeed assistive technology in general. These techniques are ultimately aimed at supporting the clinician to not only gain a better appreciation of the client’s acceptance and adherence of assistive technologies but also to moderate these in line with likely clinical outcomes.
Key points
To increase acceptance of and adherence with therapeutic footwear, person-centred communication is essential.
Person-centred communication involves engaging with and hearing the attitudes of the client to their condition, as well as discussing acceptance and expectations, in a structured consultation.
The process of shared decision making needs to be embedded in person-centred communication and is greatly enhanced when simple tools are applied to ensure the communication is effective and understood.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.