
Abstract
Background:
Adaptive seating supports for cerebral palsy are recommended to develop and maintain optimum posture, and functional use of upper extremities.
Objectives:
To compare the effectiveness of different seating adaptations regarding postural alignment and related functions and to investigate the effects of these seating adaptations on different motor levels.
Study design:
Prospective study.
Methods:
A total of 20 children with spastic cerebral palsy (Gross Motor Function Classification System 3–5) were included. Postural control and function (Seated Postural Control Measure, Sitting Assessment Scale) were measured in three different systems: standard chair, adjustable seating system and custom-made orthosis.
Results:
In results of all participants ungrouped, there was a significant difference in most parameters of both measurement tools in favor of custom-made orthosis and adjustable seating system when compared to standard chair (p < 0.0017). There was a difference among interventions in most of the Seated Postural Control Measure results in Level 4 when subjects were grouped according to Gross Motor Function Classification System levels. A difference was observed between standard chair and adjustable seating system in foot control, arm control, and total Sitting Assessment Scale scores; and between standard chair and custom-made orthosis in trunk control, arm control, and total Sitting Assessment Scale score in Level 4. There was no difference in adjustable seating system and custom-made orthosis in Sitting Assessment Scale in this group of children (p < 0.017).
Conclusion:
Although custom-made orthosis fabrication is time consuming, it is still recommended since it is custom made, easy to use, and low-cost. On the other hand, the adjustable seating system can be modified according to a patient’s height and weight.
Clinical relevance
It was found that Gross Motor Function Classification System Level 4 children benefitted most from the seating support systems. It was presented that standard chair is sufficient in providing postural alignment. Both custom-made orthosis and adjustable seating system have pros and cons and the best solution for each will be dependent on a number of factors.
Background
Children with spastic or dyskinetic cerebral palsy (CP) have several musculoskeletal problems. One of the musculoskeletal problems seen in children with CP is shortened hip and knee flexors. In order to compensate the posterior tilt of the pelvis, the thoracic-lumbar vertebrae are flexed. Compensation of back-shifting balance causes thoracic kyphosis. 1 Increased flexion in the thoraco-lumbar region complicates head control and the child tries to keep the head in balance by tilting it anteriorly or posteriorly, which generates swallowing and speech problems. The deterioration in motor behavior is closely related with decrease in postural control, and together they create a vicious cycle and deteriorate the child’s static and dynamic stabilization. 2 Secondary to deteriorated stabilization, functional inadequacies of head, body, and extremities appear. Since abnormal muscle tonus and primitive reflexes are inhibited by sitting in a proper position, an increase in postural control is achieved.1,2
Children with spastic or dyskinetic CP struggle to stand still and they spend most of their time seated. Therefore, the primary aim of rehabilitation in non-ambulant children with CP is to maximize independence and functionality in sitting position.3,4
Even in cases where children with CP can walk, they experience more difficulty in maintaining normal posture compared to their healthy counterparts.5,6 An effective sitting position provides the optimum posture for feeding, breathing, and bowel movement. Moreover, effective sitting positions enable head control, which is crucial for the development of the child’s social, cognitive, and communicative skills, by which an increase in the functional movement capacity is obtained.1,6
Several seating devices have been developed since 1960s, enabling proper postural control in sitting position. 7 Researchers’ aim in developing such seating systems is to avoid abnormal movements, enable postural control, and develop upper extremity functions by ensuring stability. These systems also provide the regulation of abnormal muscular tonus, inhibition of primitive reflexes, prevention of deformities, and the prophylaxis of muscle contractures.8,9
The use of sitting positions in improving constrained postural control, functional potential, and sitting balance has been investigated previously.2,6 The search for optimal sitting position led researchers to the concept of adaptation for straight sitting. 8 Mhyr et al. conducted a study involving 23 children with various types of CP and evaluated their head control, pathologic movements, postural control, and upper extremity function using the Sitting Assessment Scale (SAS) in six different sitting positions. They reported that there were significant differences in positions with hip abduction, in head control, and extremity function. 10 Adaptive postural supports for children with CP have been recommended in order to develop and maintain the optimum posture. Most of the previous studies in the literature have investigated the effects of adaptive devices in terms of support for neck, trunk, and hip and pelvis in terms of abductor wedge use for hip abduction, support for knee-joints, and foot/ankle. 11 Although there are several studies in the literature on the topic, to the best of our knowledge, there is no study comparing different adaptive seating systems regarding postural control and upper extremity competencies. Therefore, this study was designed to compare commercially available children’s chairs with back support, adjustable seating systems (AdSSs), and custom-made body and pelvis positioning orthoses in terms of postural alignment and related extremity functions observed by the Seated Postural Control Measure (SPCM) and the SAS in a group of children with spastic CP. The effects of these intervention methods were also to be explored by grouping the same study sample by levels of motor functioning.
Materials and methods
Participants
The study included 20 children with spastic CP with an age range of 3–6 years (mean age 3.95 ± 0.82 years). Even though most of the studies on the topic involved children of school age,12,13 there are a few studies involving children below the age of 6 years.14,15 Children of 3–6 years were selected because the effects of seating systems in such age groups were considered to be greater because the nervous system has a higher plasticity at an early age.10,15
The subjects of the study were conveniently selected among the patients who were followed up in a pediatric rehabilitation center in Ankara, Turkey.
Inclusion criteria were as follows:
Children diagnosed with CP by a pediatric neurologist;
Children must have the mental ability to perform basic instructions during tests, as assessed by the researchers by clinical judgment;
Level 3, 4, or 5 in Gross Motor Function Classification System (GMFCS) as assessed by the researchers through observations made in the center;
Able to attain 90° hip flexion.
Exclusion criteria were as follows:
Children who received botulinum toxin or intrathecal baclofen treatment in the previous 6 months;
Children who underwent pelvic, spinal, or upper extremity surgery.
Parents’ permissions, informed consent forms, and local ethical committee approval were obtained.
Methods
Expanded and revised versions of the GMFCS were used to determine the functional level of the candidates and to confirm their conformity with the inclusion criteria.16,17 Children’s age and functional status were evaluated (n = 28). Eight children were rejected: two for being older than 6, four for having sufficient functional status, and two for being mentally incapable.
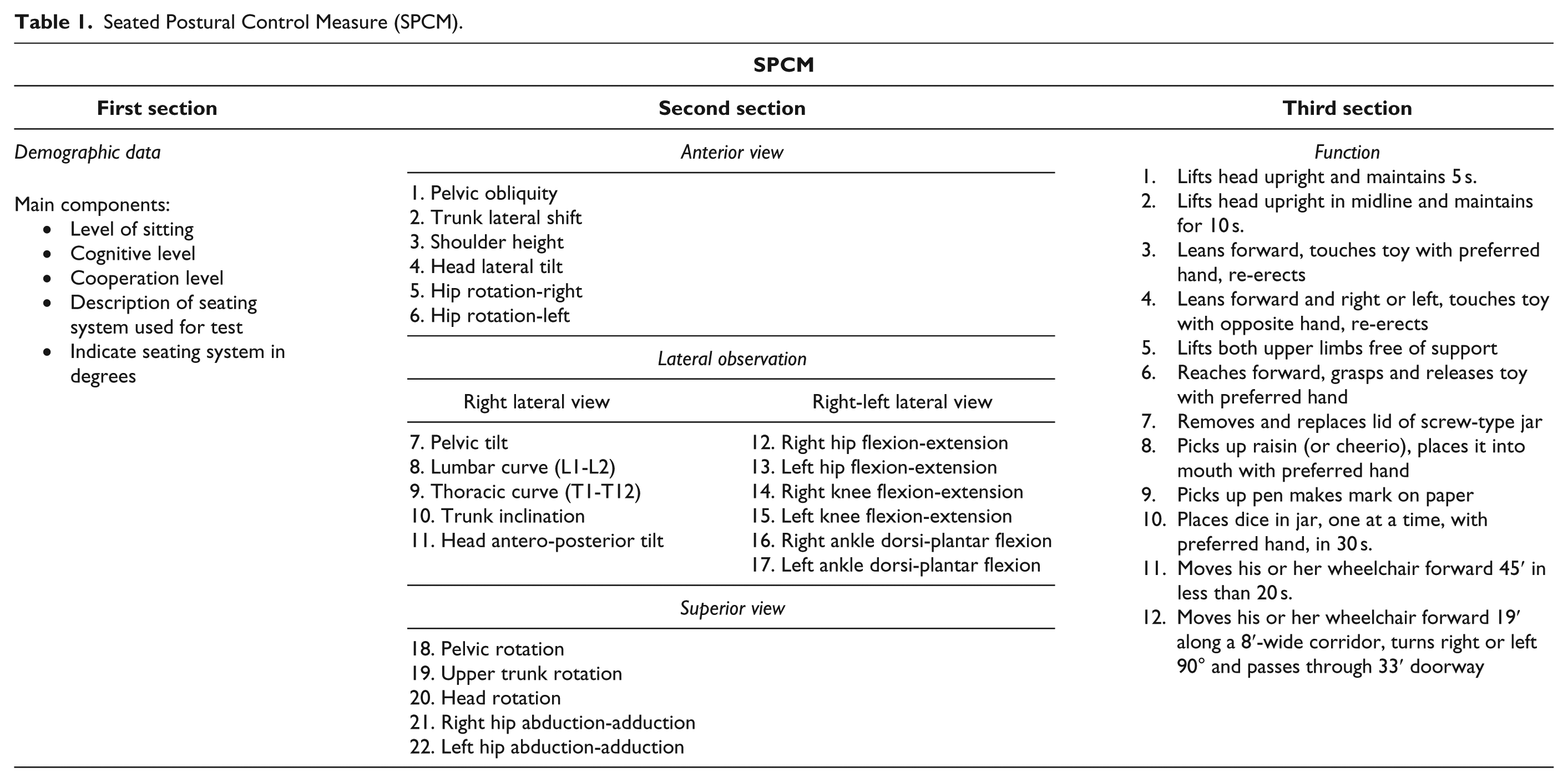
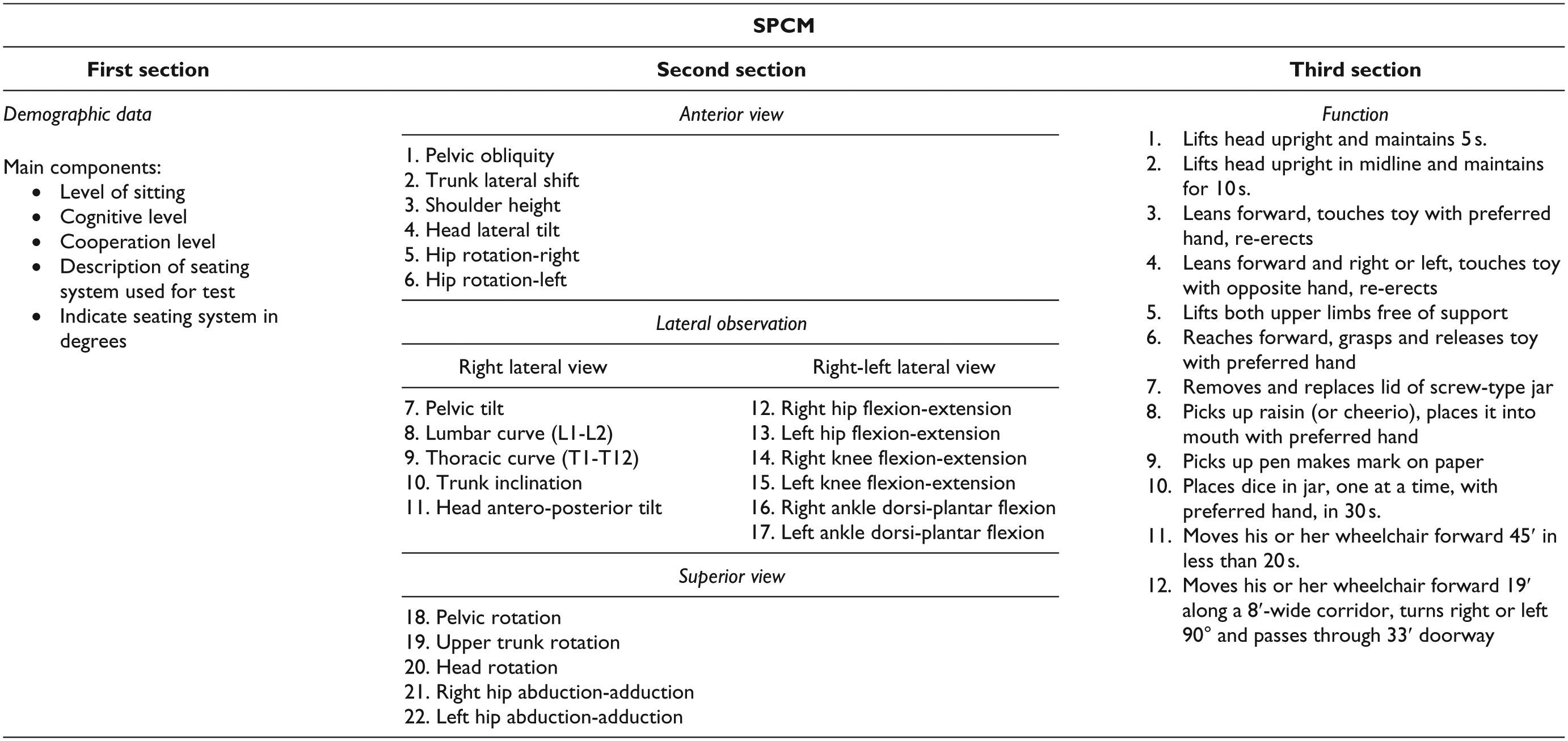
Children’s postural control and functions in sitting position were measured using the SPCM. The test–retest reliability of the SPCM was reported as 0.87. 18 The SPCM measures children’s postural alignment and effects of sitting position on postural control. 18 The SPCM has three sections. The first section is about demographics and the main components of the seating system. The second section includes postural characteristics observed through anterior, lateral, and superior observation. In the third section, upper extremity function in sitting position was assessed by means of the Function Section (Table 1). Each item is evaluated as severe, moderate, mild, and normal with a score between 1 and 4.19,20 The SPCM is administered while the child is sitting with soles touching the floor.
Seated Postural Control Measure (SPCM).
The SAS is used to evaluate head, body, foot, arm, and hand function of children with CP in sitting position on a scale from 1 (none) to 4 (good) using video recordings or direct observations.10,21 The overall intra-rater reliability of the scale was reported as adequate.10,22,23 Before the test, a desk was placed in front of the children on which there was a toy that makes noise when touched, an empty box, 6 dice, a jar with a lid, and a few small toys. During the test, the children were asked to look at a different point in the room and then back to the center of the desk. Next, they were asked to touch the toy that makes noise when touched, to open the jar and put the dice in it, to place the small toys into the box, and to raise the box above their heads. The test takes 5 min to complete. The testing environment was quiet, acclimatized, and well-lit.
All children were evaluated by the same physiotherapist who is experienced in sitting adaptations and CP. The physiotherapist piloted the evaluation measures before the study. Using both SPCM and SAS, each child was evaluated once in each of the following seating systems: in a commercially available Standard Chair (SC), in an AdSS, and in a Custom-Made Orthosis (CMO). The order of seating was random. The children were kept in each seating system for 10–15 min to complete. Tests were started after a 15-min relaxation and adaptation to the seating systems. SPCM and SAS were administered to all children in all groups.
Features of SC
A commercially available children’s chair was used (Sundvik, Ikea®) (Figure 1). The dimensions of the SC were height 55 cm, depth 29 cm, width 28 cm, seat height 29 cm, seat depth 26 cm, and seat width 28 cm. The chair had a back support providing a 90°-hip flexion and a 4-cm polyurethane cushion on the seating surface. During all observations in SC and CMO, the children were instructed to sit with their soles touching the ground. In AdSS, they were instructed to sit with their soles touching the foot plate. During evaluations in SC, the same chair was used for all children.

Standard chair.
Features and fabrication of CMO
The custom-made sitting orthosis was fabricated by an orthotist who had experience fabricating such orthoses for children with neuromuscular problems (Figure 2). Before fabricating the orthosis, bony processes and sensitive areas were marked. Then, the children were asked to put on a tight-knit body stockinette. First, the trunk was wrapped with a 15-cm plaster bandage up to the axillary line. Then, the children laid back with knees in flexion and soles on a supporting surface and slight spinal tractions were administered at the axilla and knees. Before the drying phase of the plaster cast, the crest of the ilium was determined. After the plaster cast was half-dry, pelvic obliquity caused by adductor spasticity was corrected and they were placed in prone position with 30° femoral abduction in both legs and a 90° hip flexion. In this position, the pelvis, hip, and femur were again covered with plaster casting with the proximal boundary being the axilla and distal boundary being the popliteal region (Figure 3). The children were kept in the same position until the cast was hardened, which was used as a negative model from which a positive model was obtained. The positive cast was molded using 3.2 mm polyethylene material. The inside of the orthosis was covered with 6 mm Polyform. To prevent unwanted hip motion and for pelvic stabilization, a band and a pad were utilized. To avoid the windswept position caused by adductor spasticity and related pelvic obliquity, pelvic bands, which kept both hip joints within the orthosis, were used. For some cases, based on the children’s specific needs, additional pads and bands were also used. Children were placed in custom-molded orthoses with 30° hip abduction, 90° hip flexion, and 0° tilt to the sitting surface. The orthoses did not have a headrest.

Custom-made orthosis.

Fabrication of the orthosis.
Features of AdSS
A Mygo Seating System (Leckey Brand, UK) was used (Figure 4). We used the same size for each child since the study was carried out in a limited age and body structure group; however, height and width adjustments were made. To correct postural malalignment, the children’s hip, body, and head positions were supported using suspension straps and pads attached to the seating system.

Adjustable seating.
Statistical analysis
For measured variables, minimum and maximum values were calculated, and for non-numeric data, distribution percentages were calculated. Considering the possible effects of GMFCS levels on the results, results are presented for all cases as well as classified per GMFCS levels. The analyses of the differences among the three conditions were carried out via Friedman’s test. In cases where the result is meaningful, Wilcoxon paired two-sample test with Bonferroni adjustment was used to find out the variable which differed. SPSS 15 was used for analyses.
Results
Children’s demographic data, GMFCS (Level 3, 4, 5) distribution, and percentages are presented in Table 2.
Demographic data and GMFCS distribution.
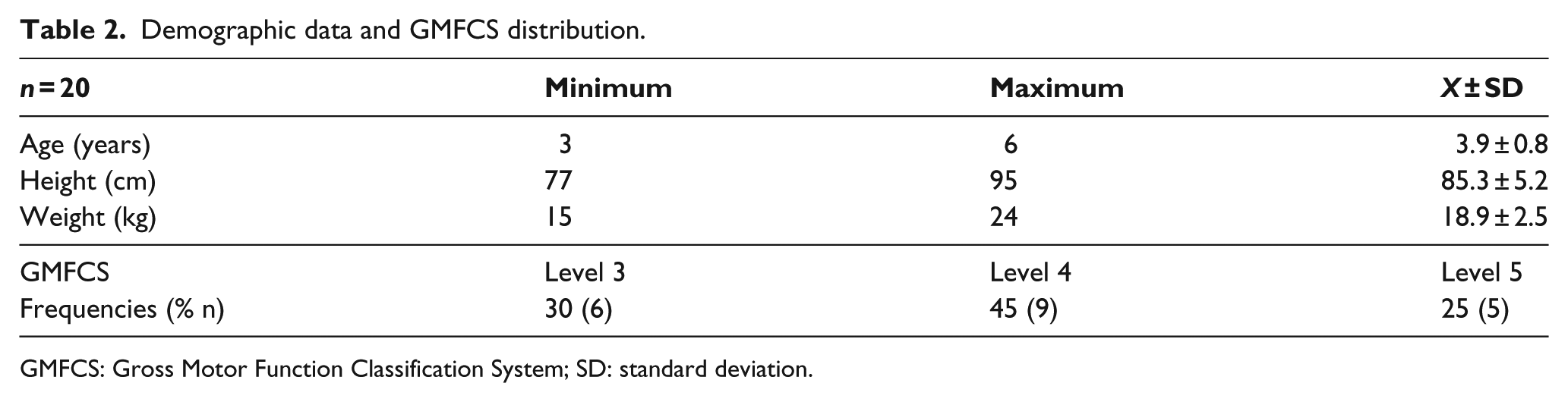
GMFCS: Gross Motor Function Classification System; SD: standard deviation.
Sample size calculation could not be performed because not sufficient literature could be accessed prior to the commencement of the study. The power calculation performed at the end of the study showed that SAS and SPCM results were different in all seating systems, and the power of attaining these differences was 95% in a sample size of n = 20 with 0.05 type I error.
SPCM values from all seating options and differences between children are presented in Table 3.
SPCM results and differences obtained in three seating options and paired comparison of groups in terms of SPCM results.
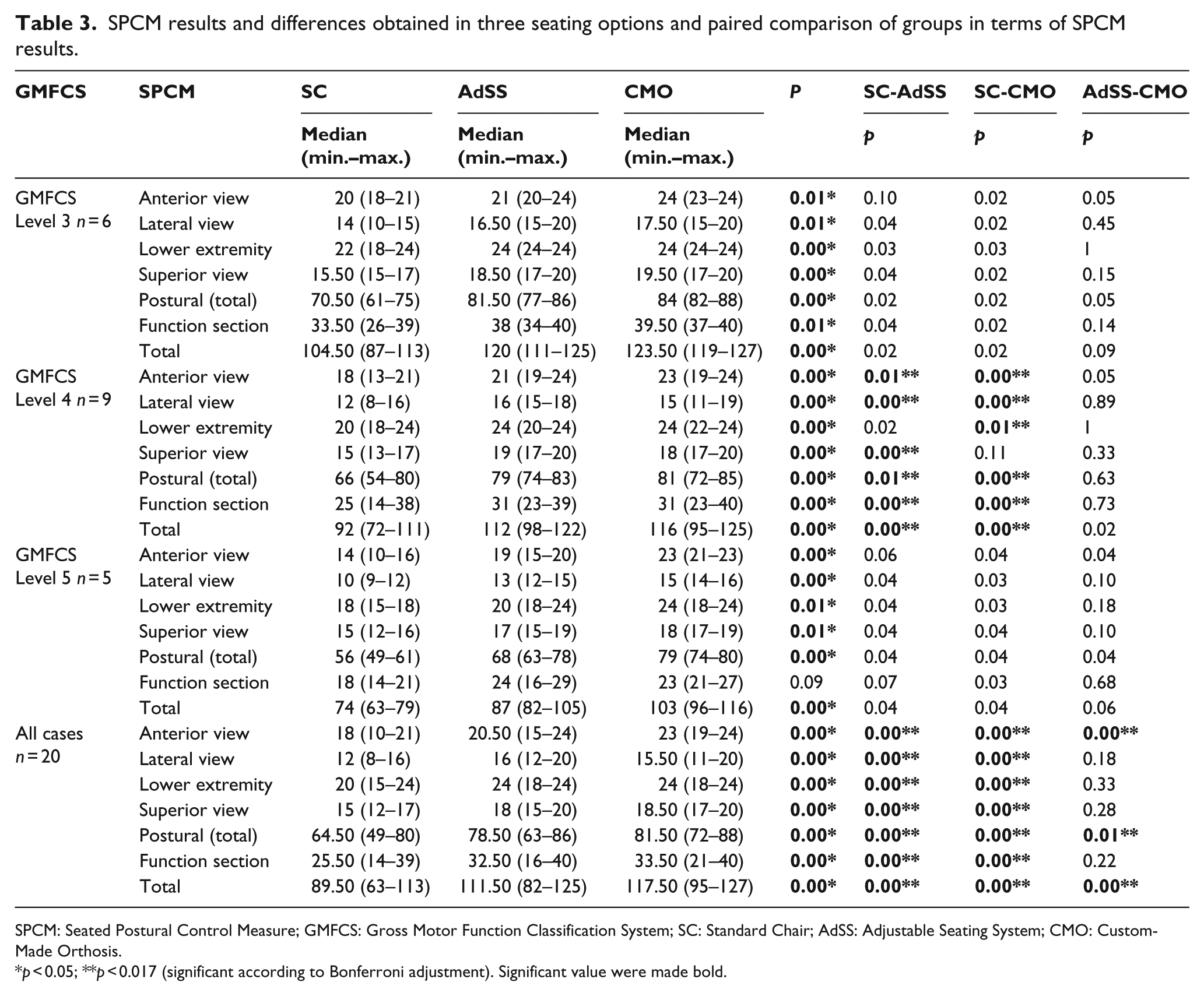
SPCM: Seated Postural Control Measure; GMFCS: Gross Motor Function Classification System; SC: Standard Chair; AdSS: Adjustable Seating System; CMO: Custom-Made Orthosis.
p < 0.05; **p < 0.017 (significant according to Bonferroni adjustment). Significant value were made bold.
Based on the SPCM results of all cases with no GMFCS grouping, there was a difference among groups. Paired comparisons of the groups showed a difference between SC and AdSS and between SC and CMO in terms of all sub-dimensions of SPCM; however, there was a difference between AdSS and CMO only in terms of anterior view, postural, and total scores (Table 3). However, the results grouped according to levels in GMFCS showed that there was a difference among all intervention groups, except the upper extremity function part of the function section in Level 5.
Results grouped in GMFCS levels showed that differences occurred most between SC and the other two intervention groups only in Level 4 children in anterior and lateral view, postural, function sections, and the total score in SPCM. The data obtained in Level 4 children also showed a difference between SC and CMO in terms of lower extremity, and between SC and AdSS in terms of superior view. For all of the SPCM parameters, no difference was observed between SC-AdSS, SC-CMO, and AdSS-CMO in Levels 3 and 5 (Table 3).
Table 4 presents SAS results of the children in all groups and the differences.
SAS test scores and differences among the treatment groups and paired comparisons of the groups in terms of SAS scores.
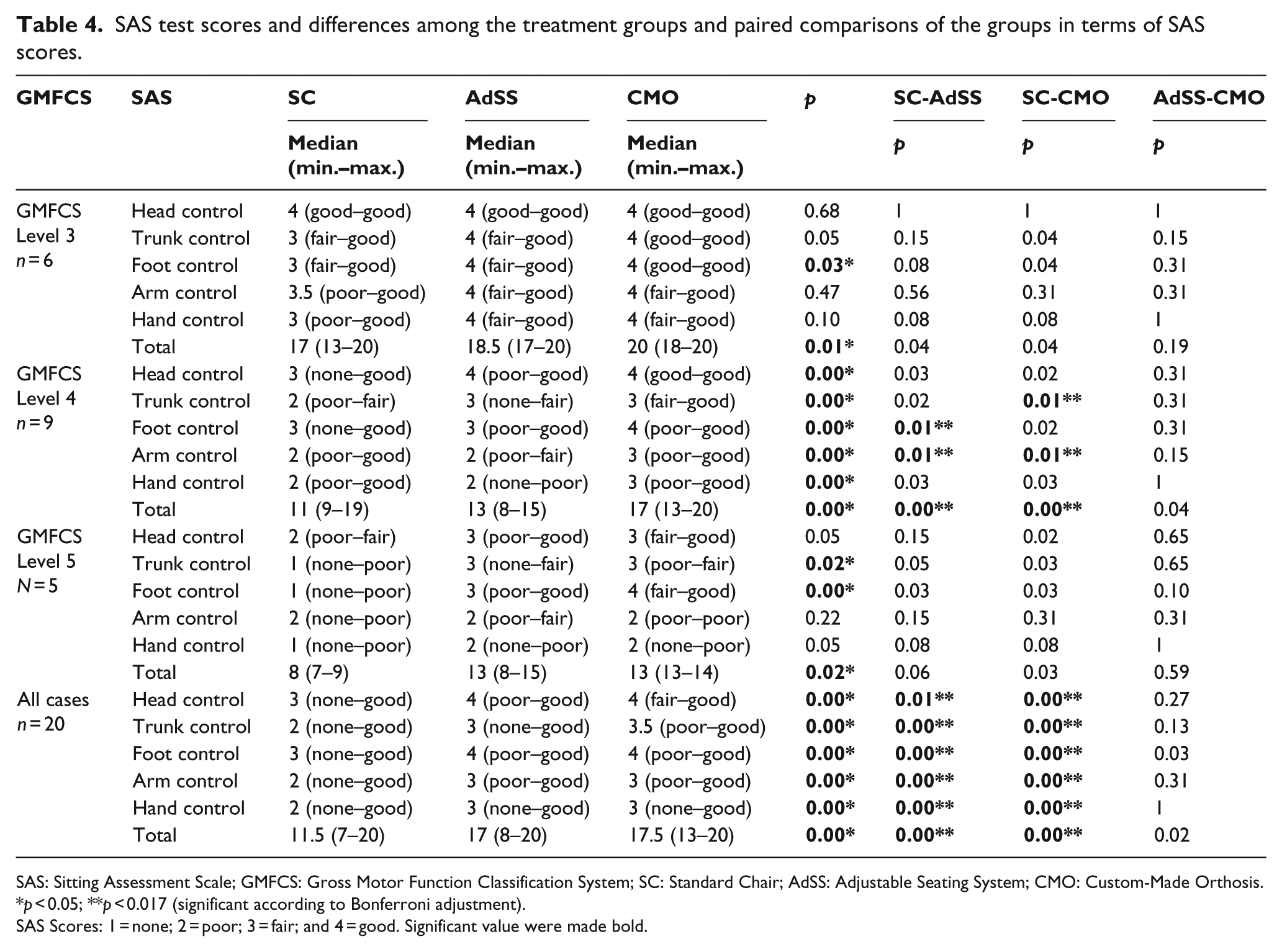
SAS: Sitting Assessment Scale; GMFCS: Gross Motor Function Classification System; SC: Standard Chair; AdSS: Adjustable Seating System; CMO: Custom-Made Orthosis.
p < 0.05; **p < 0.017 (significant according to Bonferroni adjustment).
SAS Scores: 1 = none; 2 = poor; 3 = fair; and 4 = good. Significant value were made bold.
The data belonging to all children when not grouped showed a difference among all interventions in terms of all five sub-dimensions of SAS and the total score. In all SAS items in all cases, the SC group differed from the remaining groups. However, no difference was observed between CMO and AdSS in all SAS items (Table 4).
When the children were grouped, a statistically significant difference was found among all SAS values obtained in all seating systems in Level 3 and Level 5 children; however, no difference was observed in paired comparisons.
In Level 4 SAS items, such as arm control and total scores, significant differences were shown between SC-AdSS and SC-CMO. The differences were found in trunk control item between SC-CMO and foot control item between SC-AdSS in Level 4 children. In Level 4, socio-economic status (SES) sub-domain scores were similar, except the total score, in AdSS and CMO measurements (Table 4).
Discussion
Children with CP may temporarily maintain normal posture, but they cannot perform upper extremity movement and keep their positions in the long term.5,7,23,24 Adaptive seating systems for the treatment of children with CP have been utilized for the improvement of positioning and functioning and for the prevention of various secondary complications. 11 With additional accessories, adaptive seating equipment is used to activate functionality. Researchers have been working to improve limited postural control, functional potential, and poor sitting balance using appropriate sitting positions.2,6
Our primary motivation in this study was to investigate whether different seating systems affect postural control in terms of both trunk stability and upper extremity functionality. Our secondary aim was to investigate the effects of these seating adaptations on different motor levels.
In studies investigating upper extremity functionality, during the administration of test batteries, timing, speed, and quality of upper extremity movements are monitored using 3D imaging systems, and there are some parent-reported test batteries that rely only on family observation.1,25 We chose to use the SPCM and SAS because there are validity and reliability studies for these assessment tools, and they have face validity.10,18,26 The results of this study showed that there is a very obvious need for postural support for seating in children with CP, since there was a significant difference in most sections of SPCM and SAS in favor of CMO and AdSS when compared with SC especially in GMFCS Level 4 children.
In the present study, GMFCS Level 3, 4, and 5 children were included because the children in these levels require seating systems more, and it has been reported numerous times that as the level increases, their need for seating systems also increases.11,17 It was surprising (because it contradicts with the literature) to see that there were differences among groups in terms of all SPCM values in both all children ungrouped as well as grouped, and paired comparisons showed no difference between seating groups except in Level 4 children. An analysis of these results showed that the differences in most items of SPCM were between SC and the other applications, and AdSS and CMO yielded similar results. Our results mean that Level 4 children may benefit more from such seating systems, and AdSS and CMO may better address the needs of children in this level. When the CMO and AdSS were compared, there were differences in terms of anterior view, total postural score, and total score of SPCM in favor of CMO in all cases ungrouped. In the SPCM, this difference is caused by differences from the anterior which comprises pelvic obliquity, head lateral shift, shoulder height, head lateral tilt, and hip rotation. Anterior evaluation assesses the frontal asymmetry of the body, shoulder, and pelvis. The significant difference observed in CMO, compared to AdSS, may have occurred because CMO stabilized the pelvis and the lower extremities, and thereby stabilized the body and the shoulder better than AdSS.
There was also a difference in favor of CMO in the total score and arm control item scores of SAS in GMFCS Level 4 children. The results showed that the total score was affected by the arm control score. This result was attained because shoulder straps, which are part of the CMO designed for each child, provide proximal stabilization required for the upper extremity movement. Although height and width adjustment were made according to the needs of each child and malalignment was remedied by means of suspension straps and pads in AdSS, these were not as effective as correcting the malalignment during casting. It may be argued that casting is more time-consuming and requires an experienced orthotist, which causes it to be more expensive. However, this is not the case in our country where importing AdSS is quite expensive and wages are low.
A thorough literature research revealed a lack of studies assessing postural control in these children by means of scales and functional tests, as well as exploring postural control during daily functional activities. The assessment of postural control in these children by means of scales and functional tests may provide a better insight into functional constraints in CP. Moreover, exploring postural control during functional activities allows the identification of the mainly affected activities in this population and its repercussion on the level of activity and participation of the children. Thus, the research addressing these issues can be a promising field for further research on postural control.25,27
During physiotherapy sessions for muscle training, muscle strengthening, and voluntary motor movements, an upright posture is required. 2 Gavin-Dreschnack 28 stated that the support provided for the posterior wall of the seating systems maintains the lumbar lordosis. In this study, we retained the lumbar curve and also, using a pelvic belt, we supported the pelvis at 90° hip flexion position when children were sitting with CMO and AdSS.
Nwaobi et al. 29 studied upper extremity activities at various hip flexion angles in children and adolescents with CP. They reported that voluntary control and shoulder movements with high endurance were best obtained at 90° hip flexion. In most studies, the clinical type of CP, or its severity, has been ignored. For the evaluation of postural control and upper extremity functionality, we evaluated the data for the whole group as well as in groups classified per GMFCS levels. In our study, 90° hip flexion position was used in order to control the trunk, pelvis, and extremity, and to maintain the upright position of the body. Postural control and functional skills were examined using the SPCM and SAS. An analysis of the function section of the SPCM showed significant differences among the three seating systems. In all cases ungrouped and in Level 4 patients, there was a difference between CMO and SC. Statistically significant differences were observed between AdSS and SC in all cases ungrouped and in Level 4 patients. No difference was observed between CMO and AdSS.
Both functionality in sitting position and head, trunk, and lower extremity control during hand and arm functions were evaluated using the SAS. Statistically significant differences were observed among SC, AdSS, and CMO in only foot control; total score of the SAS in Level 3 patients, in only trunk and foot control; and the total score of the SAS in Level 5 patients. There was no difference between CMO and AdSS.
Another topic of discussion in the literature is the forward or backward inclination of the seats. Theoretically, forward inclination of the seat provides a more upright and stable posture and controls the abnormal kyphosis. With this kind of sitting position, the center of gravity shifts forward, lumbar extension time increases, the backward rotation of pelvis is prevented, and hypertonus of hamstring and hip extensor muscle group is inhibited. Forward tilted seat activates hip flexors and abdominal muscles and positions the body more upright with respect to the hip.7,30,31 McClenaghan et al. 6 studied 20 children with CP with an age range of 4–10 years, and examined their upper extremity functionality by placing them in seats with varying inclinations while they were performing their daily activities. They reported no significant difference among groups (straight, tilted forward, tilted backward) regarding upper extremity functionality. 6 Some studies support forward tilting, while some support backward tilting. Therefore, before designing adaptive seating systems, children’s clinical type of CP, extremity involvement, severity of involvement, and individual differences should be considered.6,9,30,32–34
In the present study, we decided to use the horizontal plane to perform all evaluations. There was a significant difference between SC and the other seating systems when head control was evaluated in a horizontal position. There was no difference between CMO and AdSS regarding improvement in head control. This was a result of correct positioning of the proximal segments of the trunk as well as due to the maintenance of trunk stabilization in both seating adaptation systems.
Limitations
Because all children were subjected to all seating systems, the physiotherapist was not blinded to the study objectives. The children were assessed once in each seating system for each measurement scale. Instead of more robust and reliable measurement methods, such as computerized motion analysis systems, less objective measurement scales were used. The effect of front and back sitting surface inclinations were not measured. Further studies in which inclination is measured via objective techniques are required.
Conclusion
The results of the tests showed that there was a significant difference in favor of CMO and AdSS when compared to SC. Although there were some differences in favor of CMO in some items of SPCM and SAS when compared with AdSS, they can be neglected. Although CMO fabrication is a long process, it was recommended in the present study because its fabrication is low-cost compared to AdSS in our country where AdSSs are imported, which makes them more expensive. This may not be the case for all countries. In addition, CMO is custom made for the child, and it is light and portable compared to AdSS. On the other hand, AdSS can be modified according to the child’s height and weight, but it is difficult to carry. This study allowed us to gain insight into two important aspects: seating systems influence body posture and also postural control due to seating system fixations, which in turn affects their static and dynamic control, upper extremity function, and other functions in this population. On the other hand, the best seating choice for each child should be selected individually.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.