
Abstract
Background:
Knee osteoarthritis is a prevalent disease. Unloading the affected compartment using a brace is a treatment option.
Objectives:
To determine whether a decompressive knee brace alters loading in medial knee osteoarthritis following 2 and 8 weeks of use.
Study design:
Within subjects; pre- and post-testing.
Methods:
A total of 15 individuals with medial knee osteoarthritis attended four sessions: baseline, fitting, 2 weeks after fitting (post), and 8 weeks after fitting (final). A gait analysis was performed at baseline (without knee brace), post and final. Knee adduction impulse, first and second peak knee adduction moment, knee motion, and walking velocity were calculated. Participants also recorded hours and steps taken while wearing the brace.
Results:
On average, the brace was worn for more than 6 h/day. Through use of repeated-measures analysis of variance, it was determined that the knee adduction impulse and second peak knee adduction moment were reduced (p < 0.05) at post and final compared to baseline (36% and 34% reduction in knee adduction impulse, 26% reduction in second peak knee adduction moment for post and final, respectively). Furthermore, participants walked faster with increased knee motion during stance.
Conclusion:
The studied decompressive brace was effective in reducing potentially detrimental forces at the knee—knee adduction impulse and second peak knee adduction moment during the stance phase of gait.
Clinical relevance
The data from this study suggest that use of a medial unloading brace can reduce potentially detrimental adduction moments at the knee. Clinicians should use this evidence to advocate for use of this noninvasive treatment for people presenting with medial knee osteoarthritis.
Background
Knee osteoarthritis (OA) is a chronic joint disease most commonly involving degeneration of the medial compartment of the knee. Symptomatic knee OA occurs in greater than 6% of the population older than 30 years. 1 As the general population ages, the prevalence of knee OA is expected to increase. 2 The presence of knee OA is characterized by knee pain, loss of motion, and gait alterations,3–5 commonly reducing an individual’s activity, participation in society, and impairing quality of life.6,7
The standard practice when treating knee OA involves use of analgesic and anti-inflammatory agents, physical therapy intervention, progressing to joint injections and surgery when warranted. 8 Evidence is amassing suggesting that other less invasive strategies should be attempted prior to surgery. 8 Therefore, investigation of alternative, more conservative options is necessary. 9
One nonoperative, nonpharmacological method used to treat individuals with knee OA is to provide a knee brace designed to decompress or unload the medial compartment of the knee. During the midstance phase of gait, an individual’s center of mass is positioned medial to the knee joint center creating an external knee adduction moment (KAM). It is believed that as the KAM increases, so does the compressive load between the femur and tibia within the medial compartment 10 which can be theorized as contributing to increased pain and symptoms, decreased activity, and limited participation. Typically, peak KAM is used as a surrogate to investigate the amount of compression within the medial compartment. While peak KAM is informative, it may not represent the point in the range of motion where individuals are symptomatic. Thus, as a way to consider the load being applied to the medial compartment throughout the stance phase of gait, we derived the knee adduction impulse (KAI) from the area under the KAM curve. 11 Various knee braces have been designed to decompress the arthritic compartment attempting to reduce these undesirable forces.12–16 However, most commercially available braces have not been independently evaluated to determine their effectiveness. 17
Unloading types of knee braces are utilized for the management of medial knee OA much less frequently than higher risk alternatives like nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroid injections. 18 As stated in the literature review completed by Brooks, “Hutchins and Jones in 2007 reported that less than 1% of all patients with knee OA are fitted with a knee brace”. 17 Reasons for underutilization of decompressive braces are multifactorial but likely include unclear and limited evidence about the efficacy of available braces.5,19 Support for use of decompressive braces, while limited and in some cases conflicting, 18 suggests that bracing reduces the KAM during stance.20–28 The primary aim of this study is to determine whether the Rebel Reliever decompressive knee brace (Townsend Design, Bakersfield, CA) can alter compressive loading on the medial compartment of the knee following 2 and 8 weeks of use.
Methods
Participants with diagnosed knee OA between the ages of 35 and 70 years were recruited to participate. Inclusion criteria were unilateral, medial compartment OA of the knee diagnosed by an orthopedic physician and classified on the Kellgren–Lawrence scale. Specific exclusion criteria included cardiac or pulmonary disease that limits ability to walk; presence of hip, ankle, foot, or contralateral knee OA; surgical procedure in either leg within the past 6 months; or the presence of other lower limb pathology that limits the ability to walk. All participants received a prescription for the brace and provided informed written consent. This study was approved by the Institutional Review Board of Stony Brook University. The trial was registered as “Effects of Bracing on Knee Osteoarthritis” with ClincalTrials.gov identifier no. NCT01886144.
Study design
Participants were assessed at baseline and subsequently fit with the Rebel Reliever (Townsend Design, Bakersfield, CA) decompressive knee brace to be worn for 2 months. Participants attended four sessions: baseline, brace fitting, 2 weeks after brace fitting (post), and 8 weeks after brace fitting (final). At baseline, participants were measured for the knee brace according to manufacturer specifications and underwent testing as indicated below; 1 week following baseline participants returned and were fitted with the knee brace by a certified orthotist. The Rebel Reliever (Figure 1) consists of a thigh shell and a calf shell that are attached by medial and lateral uprights and hinges. The medial and lateral uprights are adjustable allowing alteration of the frontal plane angulation of the brace. The degree of valgus angulation (to decompress the medial compartment) was determined by the orthotist in part with the participant’s report of reduced symptoms during various weight bearing activities. This method was utilized to mimic procedures used during clinical application of decompressive braces employed by orthotists. The orthotist taught the participants how to don and doff the brace and instructed them to wear the brace a minimum of 3 h per day, emphasizing use when engaged in weight bearing activities. In addition, a Yamax SW-200 Step Digi-Walker (Yamax International, Tokyo, Japan) pedometer was secured to the thigh support of the knee brace to record the number of steps taken per day while wearing the brace. This pedometer has been demonstrated to be accurate and suitable for research purposes in a healthy population29,30 and found to be accurate in those who present with normal weight, overweight, and moderately obese. 31 Participants completed a daily log recording the number of hours and steps taken while wearing the brace.

Picture of the Townsend Rebel Reliever brace.
Gait analysis
We evaluated gait at baseline, without use of the knee brace, and at post and final while participants were wearing the knee brace. Instrumented gait analysis was performed using a 12-camera motion capture system (Vicon; Oxford Metrics Ltd, Oxford, UK), floor mounted force plates (Kistler Group, Winterhur, Switzerland), and the Plug-In-Gait lower body reflective marker set (Vicon; Oxford Metrics Ltd, Oxford, UK). Trials recorded when wearing the knee brace required the knee marker be placed on the lateral side of the brace at the level of the joint axis. An offset was subsequently calculated for each subject to determine knee joint center. Subjects walked at a self-selected pace across the force plates allowing for collection of kinematic (100 Hz) and kinetic (1000 Hz) data. Trials during which the foot of the affected limb did not land completely on the force plate were discarded and repeated. Kinematics and kinetics were computed using Vicon Plug-In-Gait. Custom scripts were written in Visual 3D (C-Motion, Inc., Rockville, MD) to extract sagittal angles (knee flexion/extension), gait velocity, ground reaction force (GrF), and frontal plane knee external moments during the stance phase to quantify medial compartment compression. KAM was defined as positive values and normalized to bodyweight. KAI was determined as the area under the KAM curve and provides an overall indication of the KAM during the stance phase, not just at any particular point. The two peaks in KAM that occurred during early (first peak) and late stance (second peak), the overall KAI, the peak vertical GrF, peak knee extension range of motion during stance, peak knee flexion range of motion during swing, and walking velocity were calculated.
Statistical analysis
Separate repeated-measures analyses of variance (ANOVAs) were employed to detect differences in kinematic and kinetic variables at baseline, post, and final. When significant, Bonferroni post hoc tests were performed to compare baseline to post and final. Significance was considered at p < 0.05. In a study of 12 normal subjects, 27 the variability of paired differences in repeated measures of KAM indicated that we could expect to detect a decrease of 13% in peak KAM (p < 0.05, 80% power) with 15 subjects.
Results
A total of 55 individuals were screened for eligibility. Of them, 21 individuals presented with medial compartment OA, participated in baseline assessment, and received the knee brace. A total of 6 participants were removed from the study; 3 participants reported an injury unrelated to brace wear but as a result became limited in their ability to walk; 3 participants reported difficulty putting the brace on and, although remediation was offered, chose not to wear it. Characteristics, average daily brace time wear, and average daily number of steps taken for the 15 participants that completed the testing protocol are included in Table 1.
Participant characteristics (n = 15); displayed as mean (range) unless indicated.
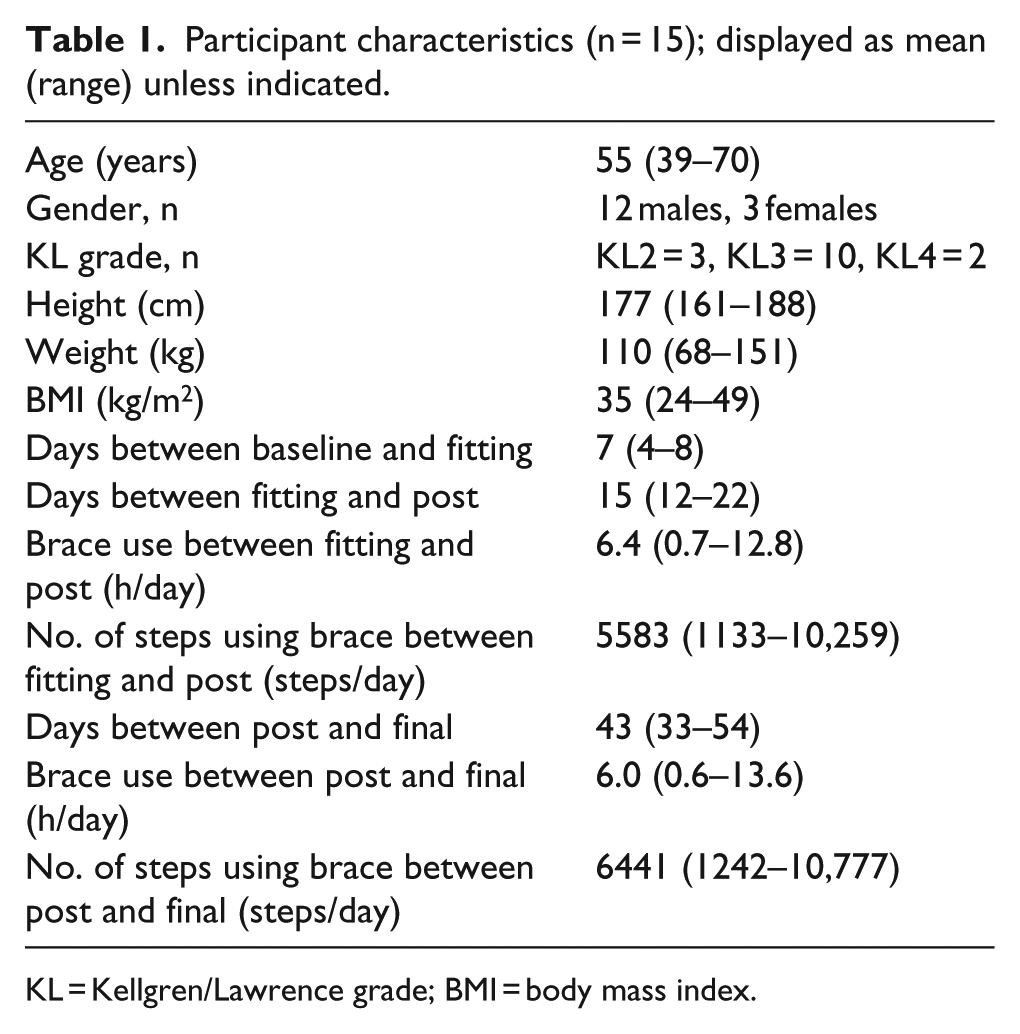
KL = Kellgren/Lawrence grade; BMI = body mass index.
Figure 2 shows the mean KAM throughout the stance phase. The KAI is visualized as the area under each curve for baseline, post, and final. Table 2 presents the mean values for the measures. Overall, the KAI (p = 0.01) and the peak KAM that occurred in the second half of the stance phase (p = 0.02) differed significantly throughout the study. Post hoc analysis revealed that the difference in KAI and peak KAM in the second half of the stance phase was significantly decreased (p < 0.05) when comparing post or final to baseline (36% and 34% reduction in KAI, 26% reduction in second peak KAM for post and final, respectively). The peak KAM that occurred during early stance phase was also lower at post and final but did not reach statistical significance (p = 0.13). Overall, gait velocity (p < 0.001) and GrF (p = 0.03) significantly increased throughout the study. Furthermore, peak knee extension during the stance phase (p = 0.006) decreased with brace wear, while peak knee flexion during the swing phase did not (p = 0.11), implying that the brace did not hinder knee motion.
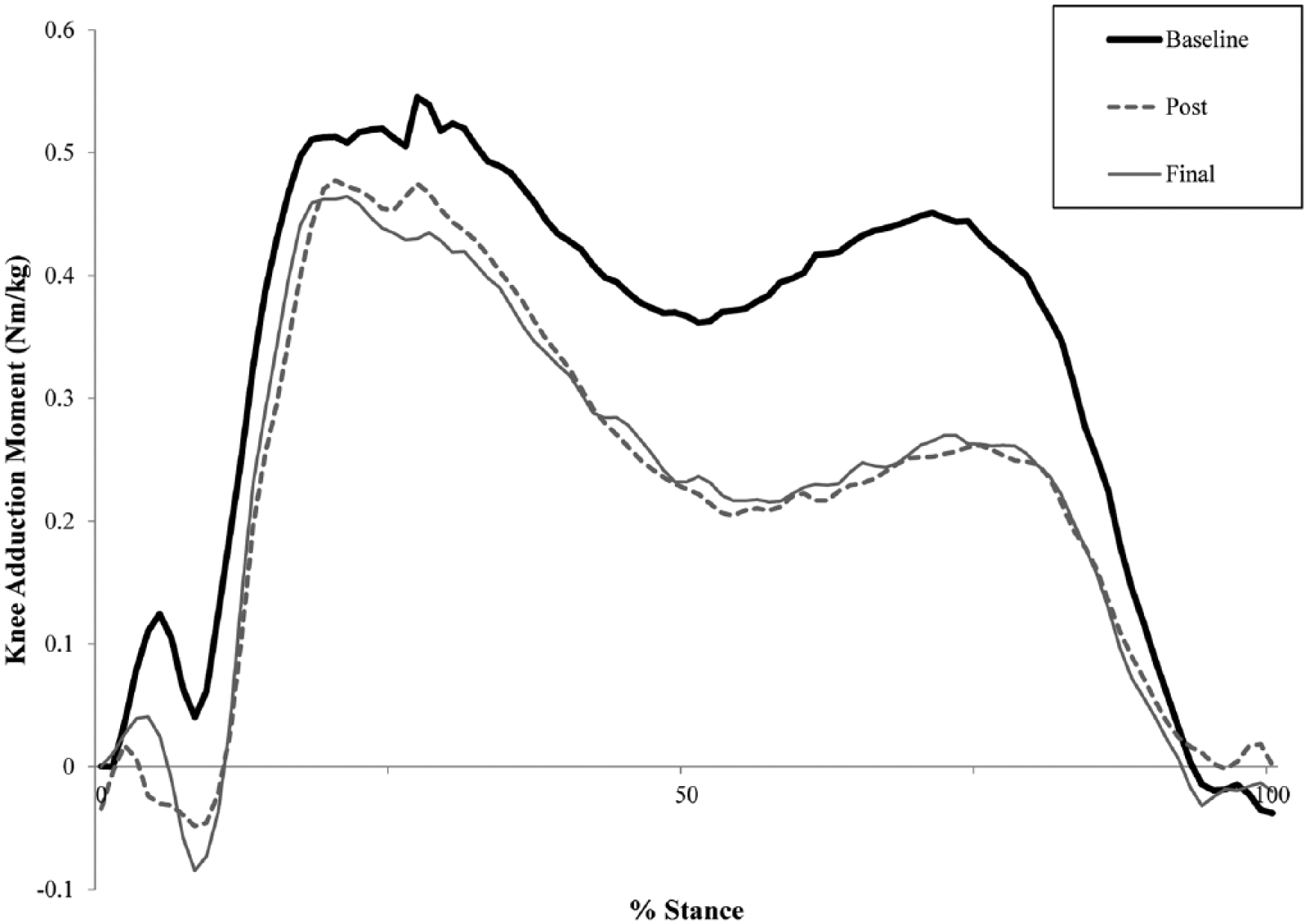
Plot of the average knee adduction moment throughout stance at baseline (solid black line), post (dotted gray line), and final (solid gray line). The knee adduction impulse is visualized as the area under each curve.
Data for various measures at baseline, post, and final.
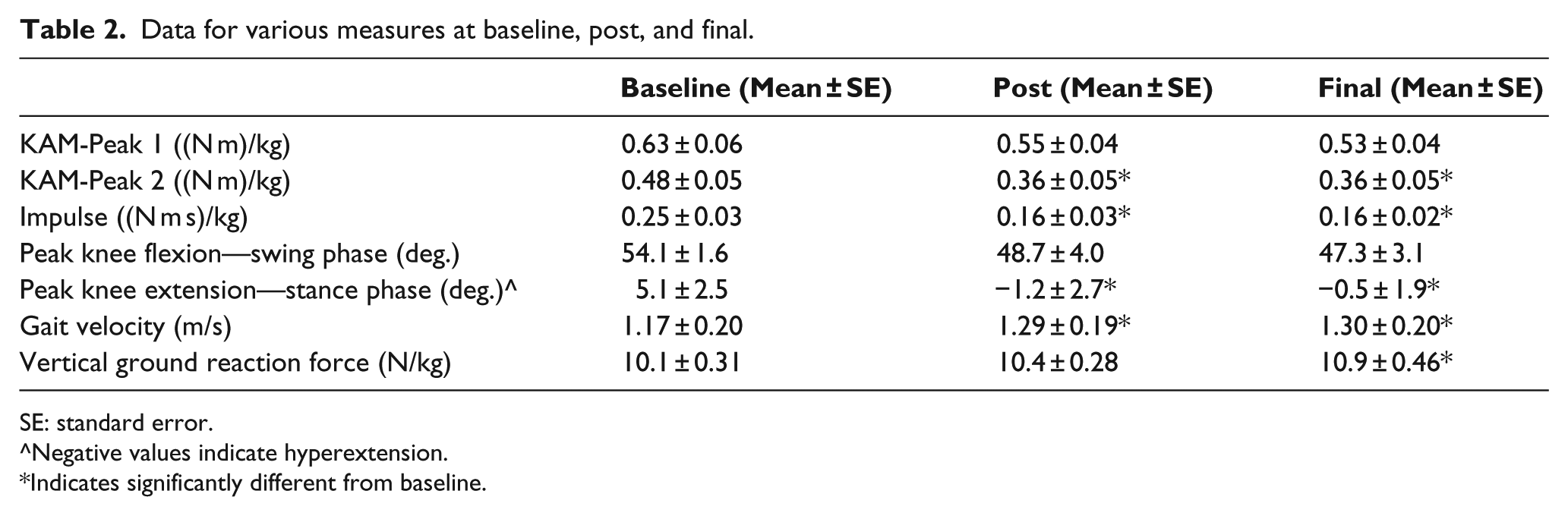
SE: standard error.
Negative values indicate hyperextension.
Indicates significantly different from baseline.
Discussion
This study evaluated the kinetic and kinematic effects of a decompressive knee brace for individuals with medial compartment OA of the knee. The results support the concept that use of a decompressive knee brace reduces the external adduction force imposed on the knee during stance. Specifically, we identified that use of the brace significantly reduces the KAI and the second peak of KAM.
High-level compressive forces in the medial compartment of the knee are considered an undesirable driving force in the progression of medial knee OA. 32 Direct measurement of these forces in vivo is difficult and invasive. The KAM is commonly used as a proxy measurement to identify the medial compartment compressive forces occurring during the stance phase of gait. 10 Results of clinical trials investigating the effectiveness of decompressive knee braces in reducing KAM are inconsistent; some show decreases of KAM while others do not. The peak KAM represents a single peak load at a moment in time. While peak KAM is informative, it may not represent the point in the range where individuals are symptomatic. In an effort to consider the load imposed on the medial compartment throughout the stance phase of gait by the adduction moment, we investigated the KAI. 11 Kean et al. 33 have suggested that KAI is sensitive and comprehensive when identifying mechanical joint loading in medial OA.
In this study, we found that KAI was significantly reduced on average by 35% as a result of wearing the knee brace. These findings are consistent with reductions in KAI (35%) found when a decompressive knee brace is worn by healthy subjects. 27 The magnitude of KAI reduction in the current study is greater than previously reported (8.6% to 18%) when decompressive knee braces are used for individuals with medial knee OA.21,34–36 The larger reduction in KAI identified in this study may be attributable to brace design. The Rebel Reliever is a rigid double upright brace which may have allowed for better attenuation of forces than braces used in other studies that were mostly single upright. In addition, we used the compression/suspension (C/S) package for all participants which encompasses semi-malleable sub-shells mounted into the thigh section of the brace that compress into soft tissue when anterior and posterior distal thigh straps are tightened which may have helped with reduced slippage.
In addition to considering the KAI, we determined two KAM peaks. The first peak KAM occurs during early stance phase and is widely analyzed and reported as it typically has the greatest magnitude, although the point in time when this occurs varies on an individual basis.
There is no consensus in the literature on efficacy of a decompressive bracing on first peak KAM reduction, which in part may explain underutilization of bracing in management of knee OA. Some studies have demonstrated significantly reduced first peak KAM26,27,35,37 while others have not.21,34,36 Participants in this study experienced a decrease in first peak KAM while wearing the decompressive brace but it did not reach statistical significance at 2 weeks (13%) or 8 weeks (16%) when compared to baseline. While our a priori power analysis indicated that we should have been able to determine this to be a statistically significant decrease, our data did not demonstrate such. This could be because the power analysis was based on data from normal subjects, whereas this study examined subjects with OA. Post hoc analysis indicated that we only obtained 24% power for this comparison. In contrast, we found a greater difference in the second peak KAM with reductions around 26%, which is in accordance with values (11%–32%) reported in other studies investigating use of decompressive knee braces.21,27,34–36
A concern about decompressive knee brace use is the potential for restricting or negatively altering functional movements. The Rebel Reliever knee brace used in this study did not negatively affect lower limb motion during gait. Participants achieved more knee extension during stance, did not reduce knee flexion during swing, and increased gait velocity. The maintenance of peak swing phase knee flexion differs from that reported by Jones et al. 35
Measurement of KAI and KAM potentially explains how the brace influences forces in an arthritic knee. An additional factor in its efficacy as an intervention is frequency of use. This study measured this in two ways; hours per day the brace was worn and the number of steps taken while wearing the brace. In this study, we recommended the brace to be worn at least 3 h per day; our participants documented brace use averaging greater than 6 h per day. This value is similar to the reported daily usage found in the few studies that have documented this variable, ranging from less than 4 h/day 35 to between 5 and 9 h/day.23,38 Furthermore, through use of a pedometer attached to the knee brace, we were able to determine that the number of steps participants took while wearing the knee brace increased, which offers insight into the fact that the participants were not sedentary during the time they wore the brace.
Several limitations of this study warrant mentioning. Our sample was predominantly male, and the greater degree of lower extremity valgus alignment typically seen in females compared to males may influence the effectiveness of the valgus unloader brace in shifting the knee to a more abducted position.39,40 Additionally, further work is necessary to demonstrate the relationship of decreased KAM and KAI with symptom relief and increased function.
Conclusion
The Rebel Reliever knee brace used in this study was effective in reducing KAI and second peak KAM during the stance phase of gait with a concurrent increase in stance phase knee extension and overall walking velocity. Furthermore, the magnitude in reduction of external knee adduction forces may be directly attributable to the design of the studied brace, the Rebel Reliever, which incorporates rigid double upright supports and an enhanced suspension system.
Footnotes
Acknowledgements
The authors would like to thank Chuancai Zou and Mayank Seth for their help with data collection.
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author’s declare that there is no conflict of interest.
Funding
This study was financially supported by Townsend Design, Bakersfield, CA, a Thuasne Company. The funding source did not have any role in collection, analysis, interpretation of the data or writing of the article.