
Abstract
Background:
The aim was to investigate the effectiveness of custom-made orthopaedic shoes (derby shoes) along with physiotherapy (twice a week) on a person with Charcot-Marie-Tooth over a period of 10 years.
Case description and methods:
A 66-year-old woman with Charcot-Marie-Tooth disease, who did not have other health conditions, complained of pain and frequent falls. Physical examination, including ankle, knee and hip muscle strength; sensory evaluation of foot and joint range of motion; self-reported assessment of pain, frequency of falls and sprains; and gait analyses, including spatial and temporal parameters and motion analyses, were performed in 2001, 2007 and 2011.
Findings and outcomes:
During the 10 years of follow-up, the physical examination parameters had stabilized since 2001; falls, sprains and walking distance had improved as compared to 2000; pain had alleviated since 2001 and gait parameters had improved up to 2007 and stabilized between 2007 and 2011.
Conclusion:
Bracing with orthopaedic shoes along with physical therapy was effective in treating pain, improving the gait and enhancing the walking distance (>500 m) without assistive device in a person with Charcot-Marie-Tooth disease.
Clinical relevance
Orthopaedic shoes along with physical therapy can be a good option for treating Charcot-Marie-Tooth associated pain, foot drop, falls and sprains, improving the gait abnormalities and also increasing the walking distance.
Background
Charcot-Marie-Tooth (CMT) disease is a hereditary sensorimotor neuropathy, which is the most common form of inherited peripheral neuropathy. The prevalence is estimated to be 1 out of 2500. 1 There are three forms of CMT. CMT 1 is a demyelinating form, which may involve the alteration of various genes and is due to the alteration of the PMP22 gene. Diagnosis is based on clinical features, nerve conduction studies and genetic tests. The main impairment resulting from CMT is progressive distal symmetrical muscle weakness and atrophy affecting the peroneus brevis and longus and the ankle dorsiflexor muscles. The outcome is instability and deformation of the feet 2 and balance disorders involving many features, including proprioceptive deficits, hyperextension of the knees during the stance phase and steppage gait. This may result into frequent falling and sprains. Some persons become wheelchair-bound in the late stages of the disease. No specific therapeutic approaches have been developed to date. 3 Only supportive treatment of CMT persons is currently available, focussing on orthosis, surgical correction of foot and hand deformities and rehabilitation.
Timely rehabilitative treatment of the deformities can result in significant functional improvement and postpone the immediate need for surgery. 4 The preliminary study that we conducted in 2001 5 on the same person with CMT 1A disease showed that after just 1 month of treatment with orthopaedic shoes (OS), the person’s pain and foot drop had decreased, her stability and gait had improved and the quantified gait assessment showed that her walking speed, cadence and step-length had increased, while the area of the foot support base had decreased. OS provide a useful overall approach, since they can be designed taking several parameters, such as pain, deformation, trophic problems and ankle stabilization, into account.
The aim of this study was to assess the efficacy of the OS along with physiotherapy in a person with degenerative CMT disease over a period of 10 years using gait analyses tools and person self-reported assessment of pain, falls and sprains.
Case description and methods
The person was examined in 2000 at the age of 55 years and her neurological, musculoskeletal and physical performances were assessed. The person’s informed consent for the OS procedure was obtained. Ethical approval is not required for retrospective case report studies in France.
Past medical history
The person had undergone surgery for claw toes, once on each side, since the age of 20 years. Her mother and her son also have similar symptoms.
History of the disease
The first symptoms appeared at the age of 35 years, in 1980. CMT was diagnosed at that time in both the foot, based on a nerve biopsy (demyelinating neuropathy), electromyographic tests (sensorimotor neuropathy) and the familial history. The genetic tests conducted in 1999 confirmed the diagnosis of CMT 1A. In 1994, since her steppage symptoms were worsening, an ankle–foot orthosis (AFO) was prescribed. The AFO was custom-made by a certified prosthetist orthotist (CPO). The AFO was not used for long by the person because it only slightly improved the drop foot problem and did not correct the fixed equinus, nor did it improve the frontal instability or reduce the loss of balance and it did not relieve her pain.
Physical and rehabilitation treatment
Two main objectives were defined: to maintain the ankle motion range by prescribing physical therapy (PT) (passive and active motion, muscle reinforcement in the lower limb, stretch posture, gait, balance and proprioceptive training) and to improve the person’s balance and gait by means of OS.
The person underwent regular PT comprising two sessions per week (30 min duration of PT) under a qualified and certified professional physiotherapist experimented during the entire 10-year follow-up period to maintain ankle range of motion, muscle strength, gait and balance capacities. The OS were made after a medical and technical meeting (with a physical and rehabilitation physician and a specialized shoe technician) at which the specifications were defined (therapeutic objectives, description of the upper, the plantar orthosis, the sole, the mode of fastening and so on). The shoes were then made and fitted to the person (Figure 1) by a certified professional having an experience of 20 years.
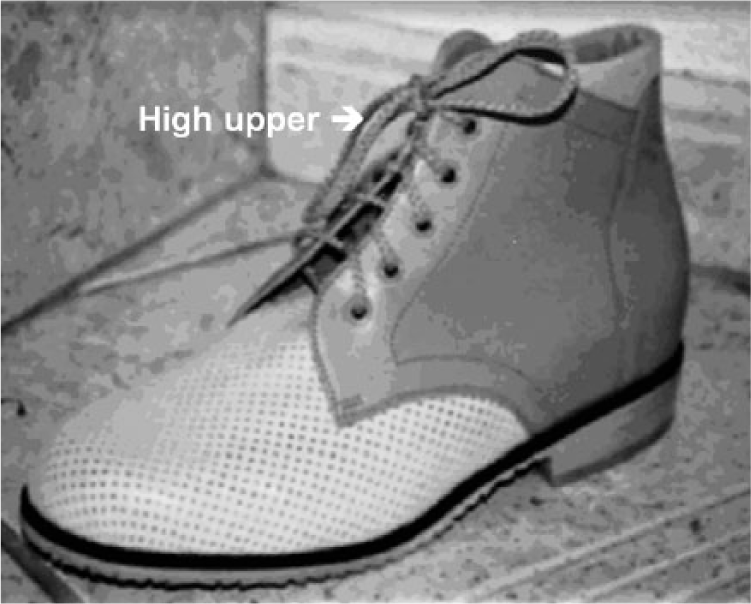
Orthopaedic shoes (2001).
In our case, the OS were designed with a view to
Prevent the foot drop with a high upper (the upper consist of the parts of shoe covering the toes, the top of the foot, the sides of the foot and the back of the heel).
Improve the person’s stability while walking and stabilize the ankle in the frontal plane via the high upper and a wide heel.
Abolish the pain by reducing friction zones and hyper supports.
Improve heel-to-toe foot movements facilitated by the shape of the soles of the shoes.
Compensate for the equinus with the insole.
Make the shoes as light as possible.
In this case, the OS model chosen was a derby shoe. This is a wide model, which is appropriate for feet with deformities, and has a high upper stabilizing the ankle in the frontal and sagittal planes. There was a thick layer of foam under the head of the metatarsus, and the part of the plantar orthosis under the toes was raised to improve the footstep. A backer made of hide or synthetic fibres is generally used inside the upper. The external plantar sole is light and resistant. To obtain a wide shoe, we used a welt and added a double sole (3 mm) and chose ‘black’ for the stitching. A broad heel was chosen to improve the person’s stability. The weight of the shoes was 400 g.
The first pair of shoes was made in 2001 5 and replaced seven times until 2012 because of wear and tear with new pairs, having the same characteristics, and prepared by the same specialized shoe technician.
Methods of assessment
Further physical examination (medical doctor specialist in Physical and Rehabilitation Medicine (PRM), self-reported measures and gait analyses were performed in 2001, 2007 and 2011. These examinations were conducted 1 month after delivery of the OS:
(a) Physical examination Evaluation of ankle, knee and hip muscle strength. Sensory evaluation: proprioception (joint position sense), graphesthesia and touch localization. Joint range of motion.
(b) Self-reported measures Frequency of falls (per week) and sprains (per months). Pain on visual analogue scale (VAS). Walking distance (<500 or >500 m).
(c) Gait analyses Clinical analyses of gait barefoot and with the OS. Assessment of temporal and spatial parameters of gait with the Gaitrite® system.
6
Findings and outcomes
Physical examination
Evaluation of ankle, knee and hip muscle strength: no changes were observed from 2001 to 2011 (Table 1). Sensory evaluation: proprioceptive sensory impairments (arthrokinesia) were observed at the lower limbs. Joint range of motion: no changes were observed for ankle range of motion from 2001 to 2011.
Self-reported measures
Frequency of falls and sprains: falls did not occur after wearing the OS for 2 months and the patient reported significant improvement in stability. Additionally, no sprains were reported. Pain on VAS: the pain completely disappeared since the use of OS (0/100 mm on the VAS score). Walking distance: walking more than 500 m independently without mobility device.
Gait analyses
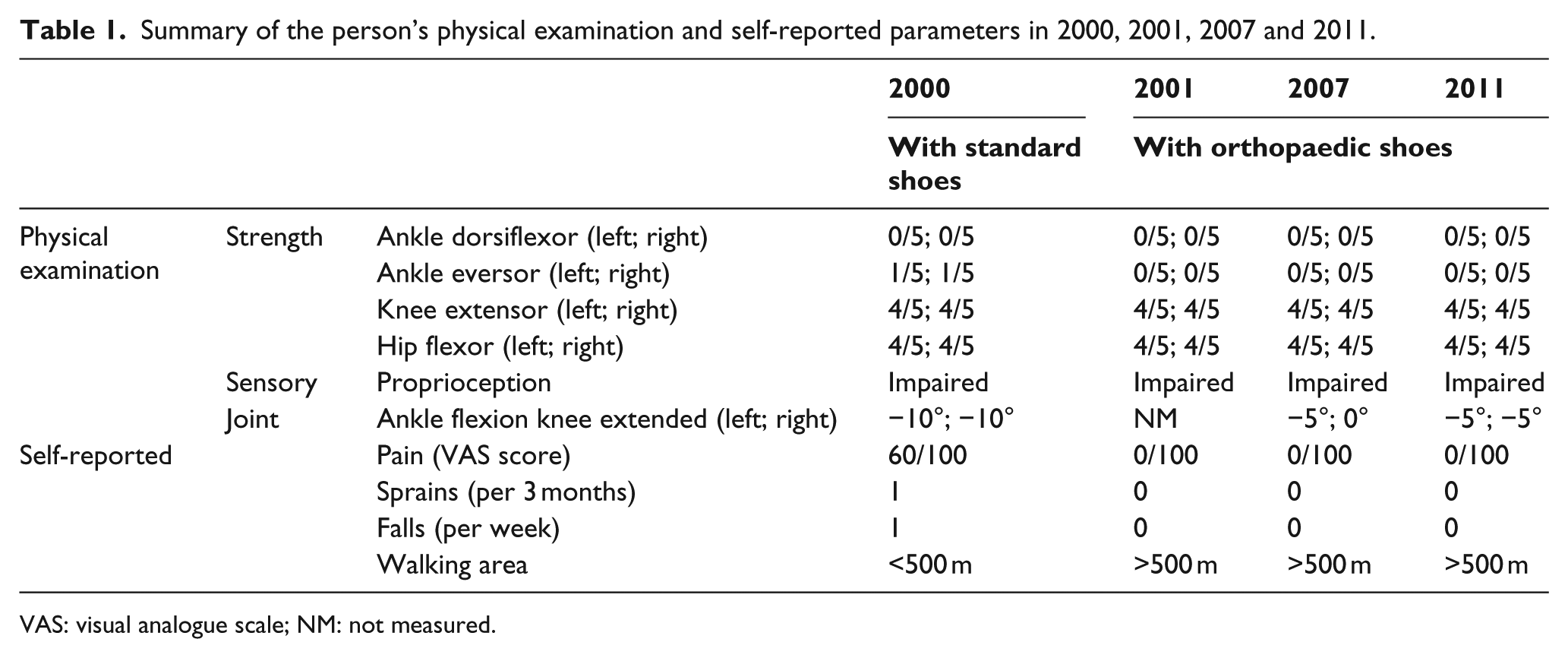
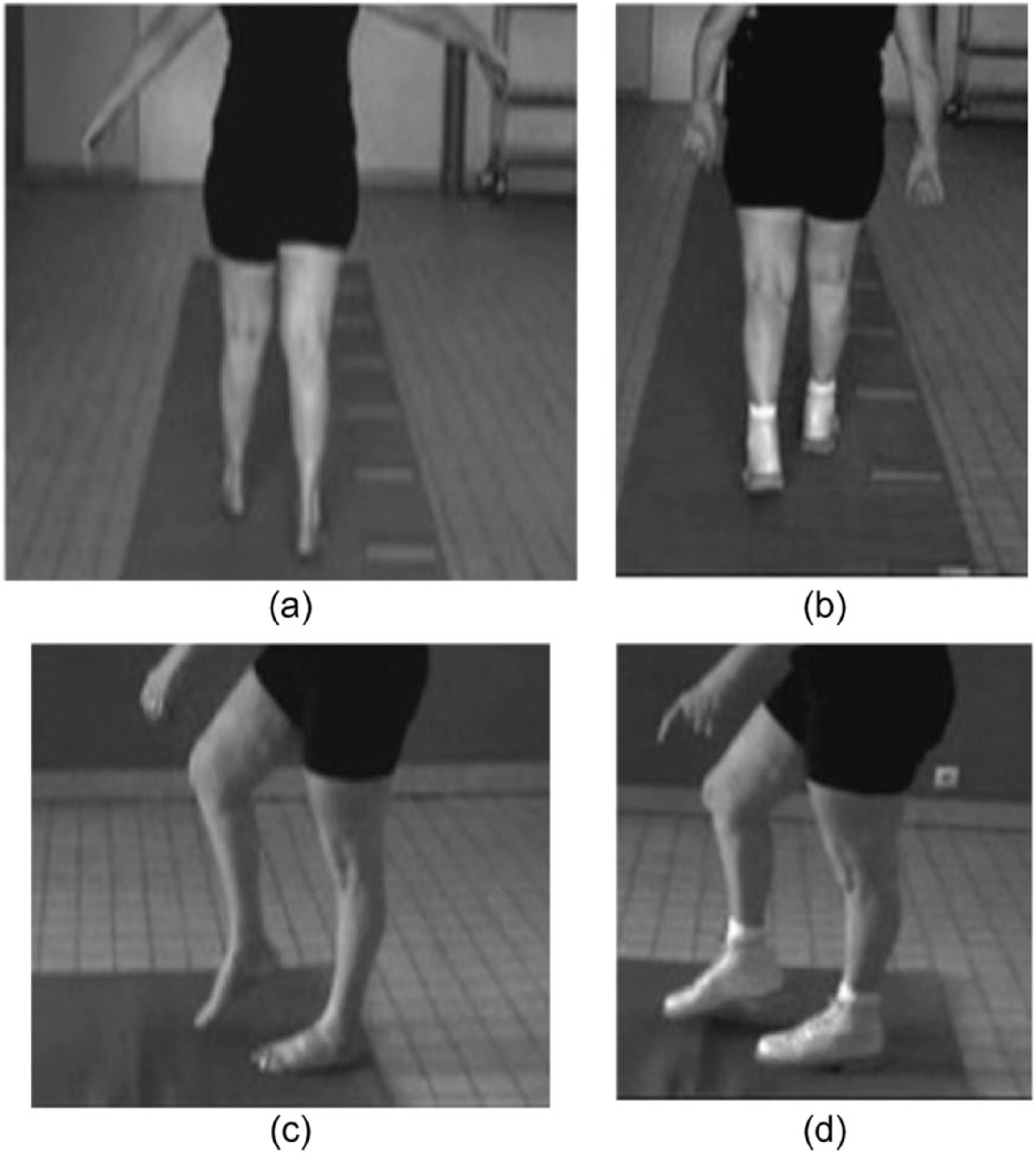
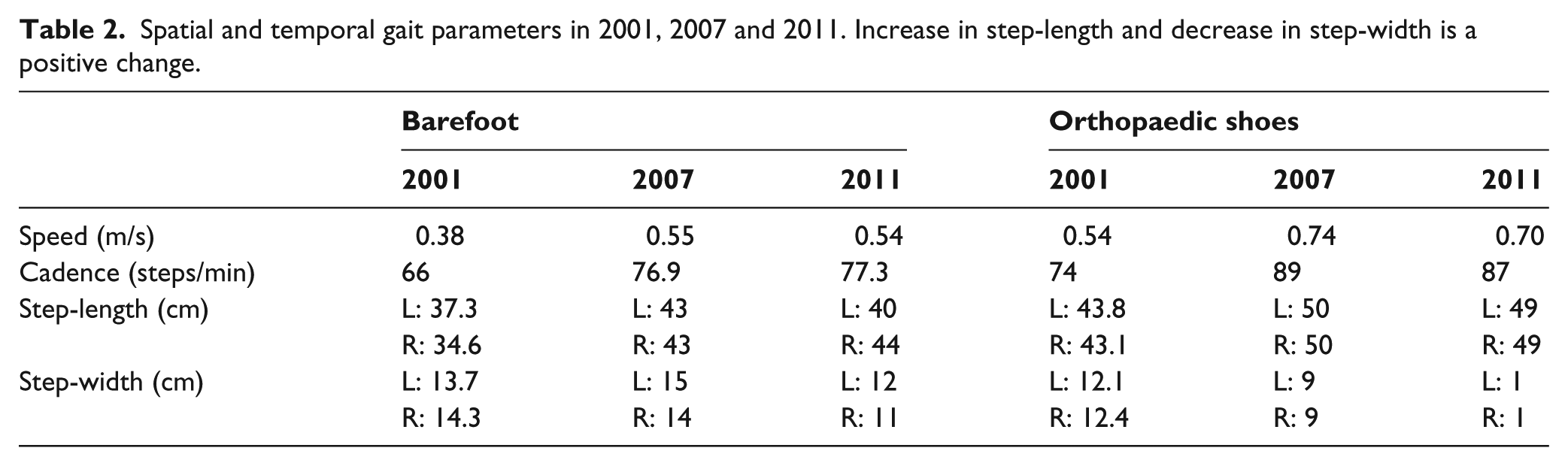
Clinical analyses of gait: the clinical barefoot gait analysis showed the existence of a balance disorder involving compensatory swinging upper limb abduction movements and an enlargement of the foot support base (Figures 2(a) and 3(a)), which decreased with OS (Figures 2(b) and 3(b)). During the swing phase, bilateral steppage was observed (Figures 2(c) and 3(c)), which decreased with OS. During the stance phase, the initial foot contact was made with the outer sides of both feet in the frontal plane and with the forefoot in the sagittal plane. With OS, the initial foot contact was a flatfoot contact (Figures 2(d) and 3(d)). Assessment of temporal and spatial parameters of gait with the Gaitrite system: the results obtained with the Gaitrite system are summarized in Table 2. An improvement in the person’s walking speed, an increase in the step-length and a decrease in the step-width was noticed both barefoot and with the OS.
Summary of the person’s physical examination and self-reported parameters in 2000, 2001, 2007 and 2011.
VAS: visual analogue scale; NM: not measured.
(a) Walking barefoot, frontal view: balance disorder, 2001, (b) walking with OS, frontal view: the abduction of upper limbs has disappeared, 2001, (c) walking barefoot, sagittal view: foot drop, genu recurvatum, high-stepping, 2001 and (d) walking with OS, sagittal view: foot drop no longer present, 2001. Photos of 2007 are not available.
(a) Walking barefoot, frontal view: balance disorder, 2011, (b) walking with OS, frontal view: the abduction of the upper limbs has disappeared, 2011, (c) walking barefoot, sagittal view: foot drop, high-stepping, 2011 and (d) walking with OS, sagittal view: foot drop no longer present, 2011.
Spatial and temporal gait parameters in 2001, 2007 and 2011. Increase in step-length and decrease in step-width is a positive change.
Discussion
OS
OS provide a useful overall approach since they can be designed taking several parameters such as pain, deformation, trophic problems and ankle stabilization into account. Since OS are lighter than standard shoes (the present model weighed only 400 grams), they reduce the muscle effort involved in walking in comparison with normal shoes. AFO can also be used for this purpose but they make no improvement in the person’s deformities and hyper supports. Management of foot deformities usually requires surgical interventions, but the clinical findings obtained after the most common surgical procedure (triple arthrodesis) have shown that it yielded poor long-term results in terms of pain relief and functional improvement. 7 Few studies have been published so far on the physical and rehabilitation treatment of persons with CMT disease. A 24-week strength training programme was found to improve persons’ walking speed. 8 Neither night splinting nor holding the ankle in the maximum dorsiflexion position for 6 weeks resulted in any significant improvement in muscle strength or the passive range of movement around the ankle. 9
To summarize, the improvement observed in the present person’s gait performances and parameters could be definitely attributed to the long-term use of OS and physical treatment, since there are no efficient drugs available, and surgery should be avoided and attempted only in the last resort.
Clinical improvement
As reported here, both the clinical and quantified gait parameters improved in this person to whom OS were prescribed for a long period of time, both with the OS and barefoot.
Since 2001, after she had been wearing OS for only 2 months, the person was no longer having falls and pain. Very few studies have established so far that the use of OS significantly decreases persons’ pain levels, 10 and these studies have dealt with pathologies of other kinds (chronic post-traumatic disabilities, diabetes, rheumatoid arthritis and so on).11,12 Also, no studies were found on the PubMed database regarding the long-term use of OS and with 10 or more years of follow-up. A study was retrieved with follow-up of 1.5 years 12 and included various pathologies (diabetes mellitus, rheumatoid arthritis, muscular disease and another disorders), and the primary outcome of this study was that 87% of participants were wearing their OS at follow-up. However, this study did not present physical examination assessments, evaluation of falls and gait.
Gait improvement
Walking distance had improved with PT and OS. No studies have been published so far in which the Gaitrite system has been used on CMT persons with OS. This is a useful system for quantifying gait parameters in clinical settings. In 2001, the person had been wearing OS for only 2 months 5 and the Gaitrite analysis on the person wearing OS showed that her walking speed, cadence and step-length had already improved. This early assessment was important because we have to make sure that persons accept the need for assistive technology, knowing that it will be helpful in the future. 13 It was reported in 2010 12 that after delivery of OS, persons need about 2 months to become accustomed to them. In addition, long-term use of OS is correlated with positive persons’ short-term (3-month) usability outcomes. 14 In 2007, the present person’s parameters had continued to improve and they had stabilized by 2011. Only one study on stroke persons has shown that an improvement in walking speed was achieved with OS in comparison with normal shoes, 15 but this was a short-term study (conducted 3.6 months after stroke). This study brought to light an unexpected finding: the fact that the person’s gait parameters barefoot parameters also improved. This improvement cannot be attributable to the evolution of the disease, which would have resulted in an aggravation of the symptoms, but may have been attributable to the continuous regular PT including muscle strength training undergone by the person and her self-rehabilitated walking performances with OS.
Limitations
One of the limitations, that is, is a case study. The present findings will therefore have to be confirmed in studies involving more persons. Another limitation is that the efficacy of OS treatment depends on the specialized shoe technician’s skill; however, we have not captured the information regarding person’s satisfaction with the different OS technicians involved in the fitting of OS at different time-points. In addition, it is often difficult to monitor all the external parameters in a long-term study involving 10 years of follow-up, such as other forms of treatment, but in the case of CMT disease, this problem can be ruled out because there exist no drugs or other forms of physical treatment, which has proven to be effective. 3
Conclusion
The current findings suggest that bracing with OS can be a good option for treating gait disabilities in persons with CMT disease.
Also, the use of OS resulted in an appreciable improvement in the person’s gait performances and quantified parameters since the person no longer tended to fall or experience pain. The OS also reduced the person’s foot drop and improved her ankle stability. The person’s barefoot performances were also found to have improved after she had been wearing OS for 6 years.
Footnotes
Acknowledgements
The authors thank Julie Bertolino and José Ramon, the pedorthosists who provided the OS.
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.