
Abstract
The aim of this study was to assess the extent to which orthopaedic shoes improved gait in a patient with Charcot-Marie-Tooth (CMT) disease and to show how the latest gait analysis tools available can help to assess and quantify the efficacy of this treatment. The case of a 55-year-old woman with CMT disease is described. She complained mainly of pain and frequent falling. The physical examination and the clinical gait analysis showed the presence of bilateral foot drop, high-stepping and varus. Treatment based on physical therapy and orthopaedic shoes was prescribed. In order to assess the clinical efficacy of the treatment, a complete physical examination was carried out after the patient had been wearing the orthopaedic shoes for one month. The quantified assessment was performed with a Gaitrite® system, which can be used to record the spatio-temporal parameters of gait. It was concluded that orthopaedic shoes provide specialists in physical and rehabilitation medicine with an excellent means of treating gait disabilities in patients with CMT disease. With the made-to-measure orthopaedic shoes used, the falling and pain disappeared; the patient's walking speed increased and the foot support base decreased in size. Both the clinical and quantified data confirmed the subjective improvement perceived by the patient. The latest tools available for performing quantified gait analysis in clinical practice provide useful means of objectively assessing the success of treatment.
Introduction
Charcot-Marie-Tooth (CMT) disease is a hereditary sensory motor neuropathy with a prevalence of 1 in 2500. Several forms of the disease have been distinguished, based mainly on nerve conduction velocity studies: The demyelinating form (CMT 1), the axonal form (CMT 2), the intermediate form and the spinal form. There are three hereditary patterns: Autosomal dominant CMT disease, autosomal recessive CMT disease and X linked CMT disease. Several genes have been identified, especially that encoding PMP 22 (peripheral myelin protein-22), which is the most frequent defective gene (CMT 1). Diagnosis is based on clinical features, nerve conduction studies and genetic tests. The penetrance is incomplete and the clinical expression is variable. The main impairment resulting from CMT is a progressive upward muscular amyotrophy that begins with the foot and peroneal muscles, instability and deformation of the feet (Sabir and Lyttle 1984; Young and Suter 2001; Planté-Bordeneuve and Said 2004). These disabilities have negative effects on gait and standing posture. The authors of gait analyses on CMT patients, (Sabir and Lyttle 1984; Vinci and Perelli 2002) have reported the presence of balance disorders involving many features: Proprioceptive deficits, hyperextension of the knees during the stance phase, hyperflexion of both knees and hips, raising of the pelvis to keep the toes from the ground during the swing phase, foot drop and incapacity to make initial contact with the heel. Walking barefoot is difficult. No specific therapeutic approaches have been developed so far. However, a great deal of research has been carried out on animal models with a view to finding means of developing genetic treatment, preventing axonal degeneration and inducing immune modulation (Young and Suter 2001; Carter et al. 2004). Rehabilitation treatment is essential (Vinci and Perelli 2002). This treatment consists of physical therapy, bracing, and sometimes surgery (Alexander and Johnson 1989; Delarque et al. 1989; Oganesian and Istomina 1991; Holmes and Hansen 1993; Delagoutte and Mainard 1996; Njegovan et al. 1997; Vinci et al. 2003). Quantifying the efficacy of these forms of treatment turns out to be much more difficult than with drug therapy. Very few quantitative studies have been carried out on gait in CMT disease, as far as the authors know. One noteworthy exception is the dynamic pedobarography study by Metaxiotis et al. (2000), in which the plantar contact areas were measured in CMT patients with cavovarus feet.
The case of a patient with CMT disease is described here. The outcome of treatment with orthopaedic shoes was assessed using a video recording system and a Gaitrite® system (Cutlip et al. 2000; Bilney et al. 2003) to record quantified spatial and temporal gait parameters.
The aim of this study was three-fold:
Describing the treatment of gait disorders in a CMT patient wearing orthopaedic shoes;
Assessing the efficacy of this treatment at the clinical level; and
Quantifying the efficacy with the latest gait analysis tools available in clinical settings.
Methods
Case report
This study deals with a patient with CMT disease, who first attended the physical medicine and rehabilitation ward at the age of 55, where she was referred from the neurology ward.
The patient's complaints, the history of the disease, and details of the neurological lesions were recorded at the first examination, and the neurological and musculoskeletal impairments were assessed, as were her physical disabilities and handicap. Therapeutic objectives were then established and orthopaedic shoes prescribed. The patient was subsequently re-examined after she had been wearing the orthopaedic shoes for one month, in order to assess their efficacy and the patient's tolerance.
Past medical history
Since the age of 20, this patient had undergone surgery many times for claw toes and left sciatica. Her mother and her son also have similar disorders.
Disease history
The first symptoms appeared at the age of 35, in 1980. The diagnosis of CMT was made at that time, based on a muscle biopsy and electromyographic and genetic tests. The patient began to undergo physical therapy. In 1994, since her high-stepping was worsening, an ankle-foot orthosis (AFO) was prescribed. The AFO was not used for long by the patient, because it did not seem to improve her gait sufficiently. It only slightly improved the drop foot problem and did not solve the patient's other complaints and problems. The AFO did not correct the fixed equinus, nor did it improve the frontal and sagittal instability or reduce the loss of balance. In addition, the AFO did nothing to alleviate the pain resulting from the claw toes. In fact, since it took up more space in the patient's standard shoes, it increased the pain resulting from the claw toes.
Main complaints
The patient first attended consultations at the physical medicine and rehabilitation ward because of the foot pains from which she suffered when walking with standard shoes (pain rating: 60 – 100 mm on the visual analogue pain scale [Huskinson 1974]) and the frequent falls she was having (1 fall per week on average).
Impairment
The clinical examination of the joints during passive movements (Muller and Boitzy 1971) showed the presence of a 10° bilateral ankle equinus (−10° of flexion). Active ankle flexion was impossible because of the complete lack of bilateral ankle flexor muscle activity. The maximum extension of the ankle was 50°. The normal values of the articular range of ankle motion were 20° in flexion and 50° in extension. The muscle strength assessment (Medical Research Council 1976) showed a complete bilateral ankle dorsiflexor deficit (0/5), a peroneal muscle deficit (2/5), a similar triceps deficit (2/5), a partial bilateral plantar flexor deficit (2/5), whereas the quadriceps (4/5) and hip flexors showed almost normal strength (4/5). Proprioceptive sensory (arthrokinesia) and graphesthesia impairments were observed in the extremities of the lower limbs whereas the superficial sensations were intact. Some areflexia was also noted.
Disabilities
The patient was unable to stand on one foot. When she was standing on both feet, there was a varus of the two subtalar joints. The patient was almost unable to walk barefoot. The barefoot gait analysis showed the existence of a balance disorder involving swinging compensatory upper limb abduction movements and an enlargement of the foot support base (Figure 1a). In the frontal plane, an ankle varus was noted. During the swing phase, bilateral foot drop and bilateral high-stepping were observed in the sagittal plane (Figure 1b). During the stance phase, in the frontal plane, the initial contact of the foot was made with the lateral side of the foot. In the sagittal plane, we could see the initial contact with the forefoot and a bilateral genu recurvatum. The patient had difficulty in going upstairs or downstairs with normal shoes. She tended to catch her drop foot on the steps and needed to hold onto the banisters to go up or down stairs.
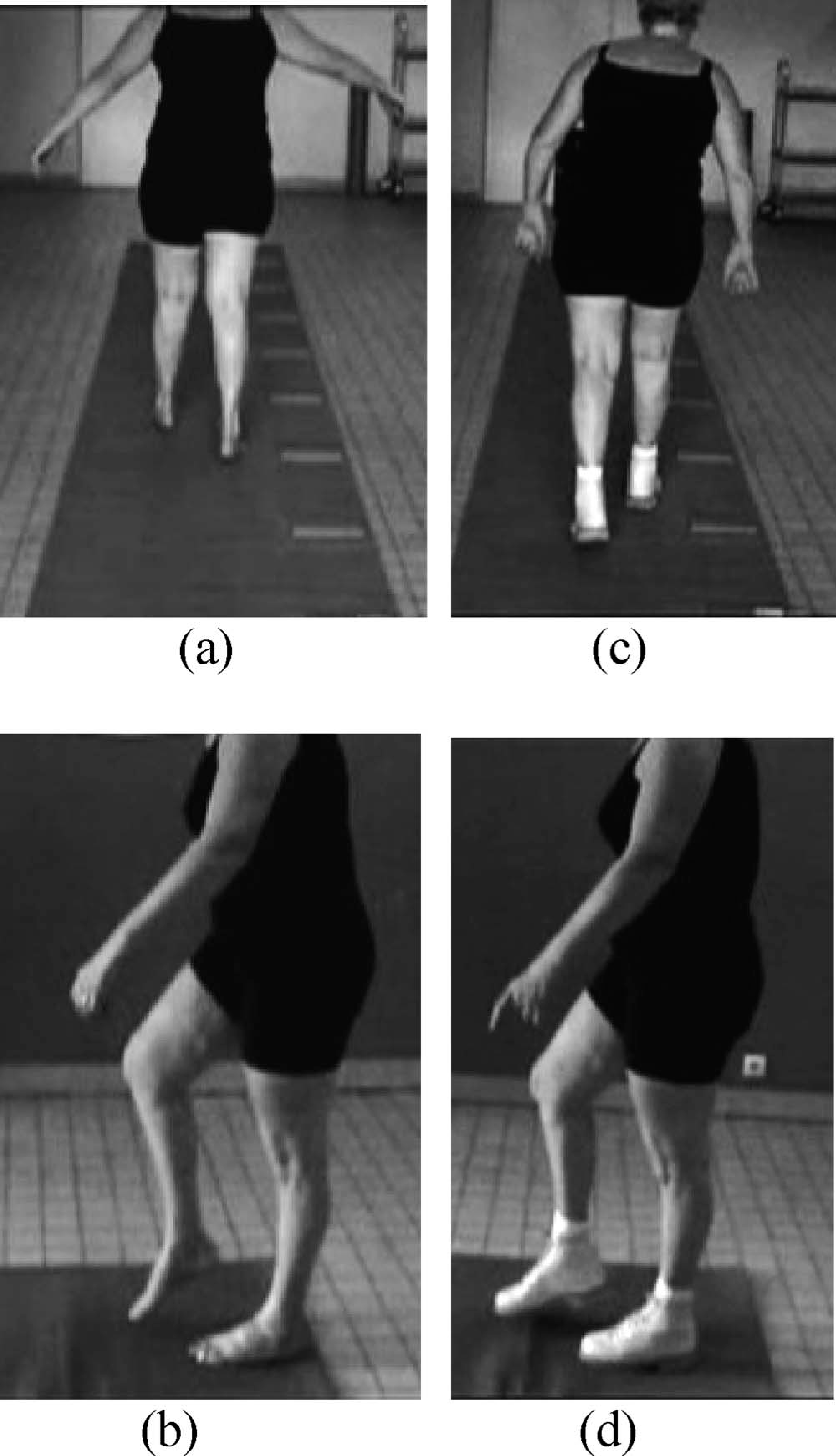
(a) Walking barefoot, frontal view, balance disorder. (b) Walking barefoot, sagittal view, foot-drop, genu recurvatum, high-stepping. (c) Walking with orthopaedic shoes, frontal view. The abduction of the upper limbs has disappeared. (d) Walking with orthopaedic shoes, sagittal view; no more foot-drop.
Handicap situation
The patient liked to take a walk. She had difficulty, however, in walking on uneven ground such as that encountered when walking in the woods or on rough country roads.
Physical and rehabilitation treatment
Based on the physical examination and gait analysis, two main objectives were defined: To maintain the range of ankle motion by prescribing physical therapy, and to improve the patient's balance and gait by means of orthopaedic shoes.
The orthopaedic shoes (Delarque et al. 1995; 1996) were made to measure after a medical and technical meeting (with a Physical and Rehabilitation physician and a specialized shoe technician) at which the specifications were defined (therapeutic objectives, description of the upper, the plantar orthosis, the sole, the mode of fastening, etc.). In the second stage, the patient had a moulding appointment with the shoe technician who then produced a positive from the moulding and corrected it if necessary. The first shoe was a transparent plastic one specially made for the trials. The trials were designed to check three main criteria: Whether the objectives defined were achieved; whether the plantar orthosis fitted; and whether there were any conflict zones.
The shoes were then made and given to the patient (Figure 2) and were designed with a view to:
Prevent the foot drop by means of a high upper;
Improve the stability when walking and stabilize the ankle in the frontal plane thanks to a high upper and a wide heel;
Abolish the pain by avoiding friction zones and pressure points;
Improve heel-to-toe foot movements by means of the shape of the soles of the shoes;
Compensate for the equinus by means of the insole; and
Make the shoes lighter than standard shoes.

The shoes have a high upper and a broad forefoot. The upper is high in order to stabilize the ankle in both the frontal and sagittal planes. The shoes are moulded to the patient's feet. The upper has a broad forepart to reduce the pain resulting from deformities and claw toes.
In this case, the orthopaedic shoe model chosen was a Derby shoe. This is a large model which is appropriate for feet with deformities, with a high upper stabilizing the ankle in the frontal and sagittal planes. The plantar orthosis can be made with thermoforming foam of various densities (Podialène® foam). There was a thick layer of foam under the head of the metatarsus, and the part of the plantar orthosis under the toes was raised to improve the footstep. The height of the heel was determined with the patient during the trial with the plastic shoes. For the upper, a backer made of hide or synthetic fibres is generally used. The external plantar sole is light and resistant. To obtain a large shoe, a welt was used with the addition of a double sole (3 mm) and ‘black’ stitching was chosen. The heel of the shoe was broad to improve the patient's stability.
Means of assessment
Clinical analysis
The authors met the patient for the second time after she had been wearing the orthopaedic shoes for one month. A further clinical examination and gait analysis were carried out. The patient was asked about falls, pain, instability and functional signs.
Video
A Sony® digital video camera was used to perform the gait analysis. The recording was transferred to a computer with a video acquisition card. Video editing was performed and the film was recorded on a CD-ROM. The film showed the patient walking in the sagittal and frontal planes (viewed from the back and front). The patient was wearing a swimsuit. A large room is necessary to record the 3 planes. The pre-treatment and post-treatment movies were then compared. Viewing them in slow motion made it easier to obtain a qualitative gait assessment.
Gaitrite®
The Gaitrite® system measures temporal and spatial gait parameters via an electronic walkway connected to the serial port of a PC. The Gaitrite® electronic walkway contains 7 sensor pads encapsulated in a roll-up carpet, giving an active area 427 cm long and 61 cm wide. Acquisition frequency is 32.2 – 38.4 Hz. As the patient is walking across the walkway, the system records the geometry and the relative pattern of each footfall as a function of time. It records the following spatial and temporal parameters: Step length, stride length, step width, angle between feet and line of progression, step time, gait cycle, velocity, cadence, stance time and swing time. The patient was asked to stand 1 m from the walkway. When told by the physiatrist to begin, she walked along the walkway at a self-paced speed (no speed recommendations were given). The task was performed barefoot before treatment and subsequently, with the orthopaedic shoes which had been worn for a month. The patient walked twice along the walkway at each recording session.
Results
Self-assessment
After one month with the orthopaedic shoes, the pain had completely disappeared (0/100 in mm on the VAS score). The patient felt a significant improvement in her stability. She no longer tended to fall, which was her main complaint previously. While wearing the orthopaedic shoes, she was able to go up and down stairs and walk on uneven ground.
Gait analysis
In the frontal plane, a decrease in the varus was noted during the swing phase. The balance improved because there was no longer any need for the upper limbs to make compensatory stabilizing movements (Figure 1c). In the sagittal plane, the clinical gait analysis showed that the steppage had decreased, that there was no longer any foot drop, and that the initial contact with the ground was a flatfoot contact (Figure 1d).
The patient's walking performances barefoot and wearing orthopaedic shoes were compared by looking at the two video films.
The film shot in the frontal plane showed that the sweeping compensatory movements of the upper limbs had decreased, the patient's stability had improved, the high-stepping was less pronounced, and the initial foot contact pattern had changed. The video film also showed that the patient's walking speed had increased and the area of the foot support base had decreased. By watching the film in slow motion, it was possible to analyse these parameters in detail.
Gaitrite®
The results obtained with the Gaitrite® system are summarized in Table I. After the treatment, an increase in the walking speed and a faster cadence were observed. The length of the steps increased, whereas their width decreased.
Spatial and temporal gait parameters.
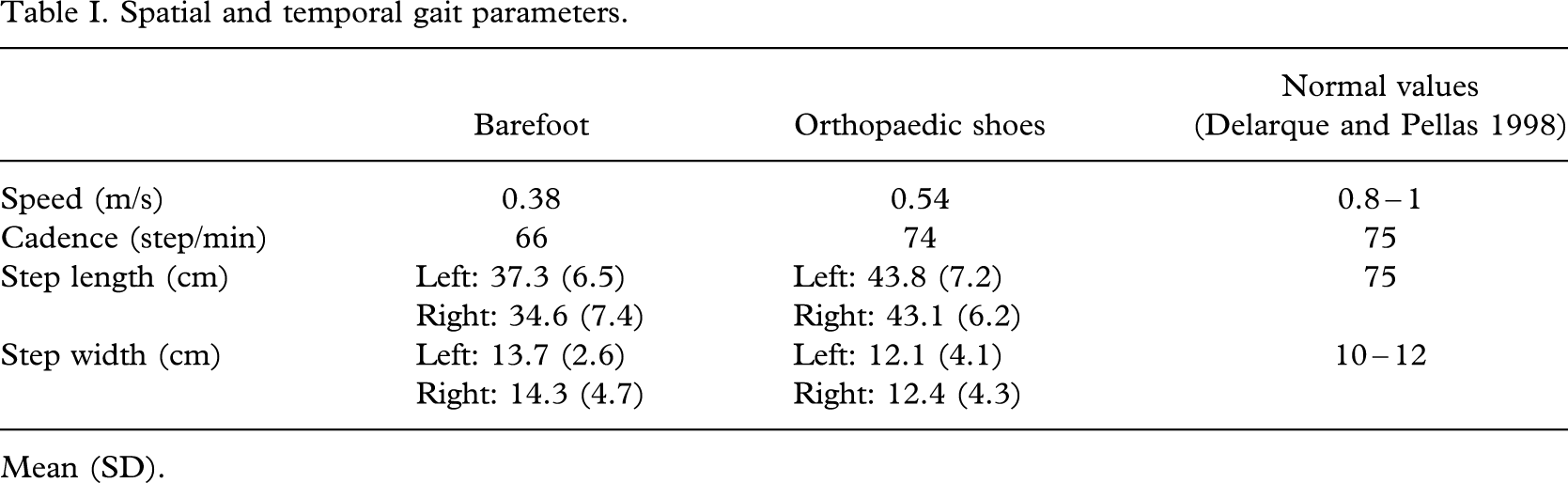
Mean (SD).
Discussion
The aim of this study was to describe a case where a patient with CMT disease was treated at a physical medicine and rehabilitation ward and to present the methods used to assess the clinical efficacy of this treatment and to quantify the spatial and temporal parameters of the patient's gait before and after treatment.
Physical and rehabilitation medical treatment
To the authors' knowledge, no studies have been published so far where quantified assessments have been made on patients with CMT disease treated mainly by prescribing orthopaedic shoes. CMT disease is a progressive pathology which tends to worsen with time. Physical medicine and rehabilitation treatment always require follow-up. One of the main advantages of bracing is that braces can be adapted to the clinical evolution. However, orthopaedic shoes provide a useful overall approach, since they can be designed taking many parameters such as pain, deformation and trophic problems into account. When wearing standard shoes, the patient complained of pain in the feet, frequent falling, and difficulty in going up and down stairs and walking on uneven ground. All these problems disappeared when the patient started wearing the orthopaedic shoes.
Standard shoes raised major problems due to the pain they caused and the lack of ankle stabilization they provided. Since these shoes were not moulded to allow for the foot deformities, there were painful contacts at the toe level. The low uppers of standard women's shoes do not help to stabilize the ankle. In addition, the patient could not find any shoes on the market corresponding better to her foot deformities.
It is also important to recall that standard shoes are heavier than orthopaedic ones. As orthopaedic shoes are light (the present model weighed only 400 g), they require less muscular effort. However, it has turned out to be difficult to assess the outcome of treatment of this kind. There is also an aesthetic problem, especially for female patients: Orthopaedic shoes are not available in many styles, as standard shoes are.
To the authors' knowledge, no studies have been performed so far in which orthopaedic shoes and AFOs have been compared in patients with neurological disorders. In this case, the choice of treatment was based on the patient's characteristics and previous treatment, the results of the clinical examination and those of clinical gait analysis. The AFO failed to improve the patient's condition. Unlike the AFO, orthopaedic shoes improved the ankle stabilization in the frontal plane and helped to compensate for the equinus. Since these shoes were moulded taking the foot deformities into account, they also prevented the pain resulting from a mismatch between the shoes and the shape of the feet. This is not the case with the AFO worn in standard shoes. One of the advantages of orthoses is that they can be used with standard shoes, but they make no allowance for the patients' deformities and pressure points.
Lastly, bracing strategies are more successful than the surgical treatment of deformations for the following reasons: Braces are less invasive and can be adapted to the evolution of the disease, whereas surgery is permanent. In addition, bracing does not entail the risks inherent to surgery, such as the possible effects of anaesthesia and the risk of post-operative infections. Cases where surgery has failed have been reported in the literature, in the study on triple arthrodesis by Wetmore and Drennan (1989), for instance, which was carried out on 16 patients with a mean age of 15 years suffering from CMT disease and foot deformations. This retrospective study showed the poor long-term results obtained in terms of pain and the functional improvement obtained. The authors concluded that this form of surgery should be performed only in the last resort.
To summarize, fitting orthopaedic shoes is the first strategy which should be used to treat the gait problems of CMT patients, to improve their gait and alleviate their pain. Surgery should be attempted only in the last resort when orthopaedic shoes cannot be fitted or when these are no longer effective.
Clinical efficacy
The final clinical assessment made at the follow-up consultation was based partly on the pre- and post-treatment video recordings. The case history is used here to give an idea of the patients' subjective feelings and helps to make sure that the objectives set correspond to the patients' hopes in terms of reducing their complaints. The patient complained mainly about the unsuitability of standard shoes, foot pains (60/100 on the visual analogue pain rating scale), frequent falling (1 fall/week on average), and the problems involved in walking on uneven ground and going up and down stairs. With the orthopaedic shoes, the pain had completely disappeared within one month (pain rating: 0/100). The patient felt that her stability had significantly improved. She no longer had any falls, which was her main problem prior to the treatment. With orthopaedic shoes, the patient was able to go up and down stairs and to walk on uneven ground.
Video provides a useful reproducible gait assessment tool. The authors used this tool here to complete the clinical studies on the patient's actual gait. The physician must first see the patient walking before watching the video film; otherwise the film would be pointless. As far as is known there are few reports in the literature on the use of video techniques in clinical practice. Lemaire (2004) measured spatial parameters (joint angles, distance and speed) based on a video recording. Harlaar et al. (2000) used the SYBAR® system, in which integrated video recording and display, an electromyogram and force plate data are combined. The use of films has many advantages: Films can be used to make comparisons as well as to readily assess the persistence, improvement or aggravation of an ankle varus or a balance disorder in the frontal plane, and the evolution of foot drop, hip hyper flexion, genu recurvatum and initial foot contact patterns in the sagittal plane. Comparisons between the results obtained at two medical consultations are crucial, since medical consultations sometimes take place only every 3 months. Moreover, the use of a video camera requires no special technical knowledge and the equipment is not expensive. Lastly, video films can provide an excellent practical, interactive student teaching aid.
Quantitative assessment of spatial and temporal parameters
Among the parameters recorded with the Gaitrite® system, the authors have kept only those most relevant to this particular case: Step width, speed, cadence and step length. These parameters made it possible to quantify the efficacy of the treatment. The gait parameter which showed the greatest improvement was the walking speed. The increase in speed may have been due to the increase in the cadence and the step length. However, this patient was walking very slowly prior to treatment (0.38 m/s). She had a conspicuous gait and locomotor disabilities. The aim of the orthopaedic shoes was to reduce these disabilities but it was not really expected for this patient to recover normal gait values. The gait parameters such as speed, cadence and step length improved significantly with the orthopaedic shoes, thus confirming the functional improvement obtained. However, the results obtained naturally did not reach normal values. The decrease in the foot support base was also quantified; the quantified assessment reflected the improvement subjectively perceived by the patient and was in line with the findings made with the video camera. This method is a useful means of following up the parameters of interest. Gaitrite®, the validity of which was previously established (Cutlip et al. 2000; Bilney et al. 2003) has been used to analyse gait in a few neurological pathologies such as Parkinson's disease (Nelson et al. 2002); no studies seem to have been carried out with Gaitrite® on gait in CMT patients with bracing, although Metaxiotis et al. (2000) have performed a dynamic pedobarography study on cavovarus foot deformity in CMT, in which they recorded the pre- and post-operative pressure parameters and foot contact areas. This study made it possible to assess and classify cavovarus feet and to objectively quantify the components of equino-cavo-varus foot.
The Gaitrite® system is much simpler to use in daily clinical practice than most other gait analysis tools such as opto-electronic systems. One of the only drawbacks of the Gaitrite® system is its cost.
Conclusion
CMT disease is a progressive disease which results in pain and especially gait disabilities for which no causal treatment is available to date. In the case of the patient under study, the orthopaedic shoes made to measure reduced the pain and foot drop and improved the patient's stability and gait. There was an appreciable improvement in the patient's quality of life, since she no longer tended to fall and no longer felt any pain. The Gaitrite® system actually showed that an increase in speed, cadence and step length and a decrease in the area of the foot support base occurred thanks to the orthopaedic shoes. It can therefore be said to be advisable to combine both clinical and instrumental gait assessments when assessing the efficacy of treatment in patients with gait disabilities.