
Abstract
Background:
Input from target respondents in the development of patient-reported outcome measures is necessary to ensure that the instrument is meaningful.
Objectives:
To solicit perspectives of prosthetic limb users about their mobility experiences and to inform development of the Prosthetic Limb Users Survey of Mobility.
Study design:
Qualitative study.
Methods:
Four focus groups of lower limb prosthesis users were held in different regions of the United States. Focus group transcripts were coded, and themes were identified. Feedback from participants was used to develop a framework for measuring mobility with a lower limb prosthesis.
Results:
Focus group participants (N = 37) described mobility as a confluence of factors that included characteristics of the individual, activity, and environment. Identified themes were defined as individual characteristics, forms of movement, and environmental situations. Prosthetic mobility was conceptualized as movement activities performed in an environmental or situational context.
Conclusion:
Respondent feedback used to guide development of Prosthetic Limb Users Survey of Mobility established a foundation for a new person-centered measure of mobility with a prosthetic limb.
Clinical relevance
Perspectives of target respondents are needed to guide development of instruments intended to measure health outcomes. Focus groups of prosthetic limb users were conducted to solicit experiences related to mobility with a lower limb prosthesis. Results were used to inform development of a clinically meaningful, person-centered instrument.
Background
Development of person-centered, clinically meaningful health instruments requires input from the individuals being measured.1–4 For example, prosthetic limb users are uniquely positioned to provide meaningful information about how the interventions they receive affect important health-related outcomes, such as home or community mobility. 5 Although prosthetic limb users’ perceptions of their health are often discussed with providers, routine measurement of patient-reported outcomes (PROs) is uncommon. 6 Standardized evaluation of prosthetic outcomes is likely challenged, at least in part, by limited access to instruments suited to measuring outcomes of importance to patients in a clinical setting.
Patient-reported outcome measures (PROMs) are standardized instruments designed to measure patients’ perceptions of their health and are well suited to measurement of complex outcomes such as prosthetic mobility. 7 Consistent with current methodological standards, PROMs must be created with input from representatives of the target population to ensure they address issues of importance and meaning to end users. 8 PROM developers conduct focus groups of target respondents (e.g. people with lower limb loss) in order to solicit their attitudes, experiences, perceptions, and opinions related to outcomes of interest. In the context of instrument development, focus group facilitators use open-ended questions (e.g. “What mobility challenges do you face on a regular basis because you use a prosthesis?”) and peer-to-peer discussions to elicit examples of shared experiences and common vocabulary that can inform development of new instrument questions. 9 Focus group discussions are also used to develop, refine, and confirm conceptual models of the outcome of interest.1,2
The purpose of this study was to explore how prosthetic limb users conceptualize mobility with a prosthetic limb, construct a conceptual model of prosthetic mobility meaningful to people with lower limb loss, confirm key definitions, and inform development of items for the Prosthetic Limb Users Survey of Mobility (PLUS-M), a PROM intended to assess prosthetic mobility in people with lower limb loss. PROMs currently available for measuring mobility of prosthetic users are often limited by a variety of psychometric issues, including poor reliability, floor and ceiling effects, and a lack of responsiveness. 10 PLUS-M has been developed using a mixture of qualitative and quantitative methods recognized to maximize a PROM’s psychometric qualities. Here, focus groups of target respondents were convened to provide initial evidence of the target concept and measurement model, in accordance with established instrument development standards. 11
Methods
Focus groups in this study were modeled after those conducted during development of the National Institutes of Health’s Patient-Reported Outcomes Measurement Information System (PROMIS).11,12 Focus groups were conducted in different geographic areas in order to solicit experiences from individuals who live in different climates. All study procedures were conducted in accordance with institutional review board (IRB) approved methods.
Participants
Focus group participants were recruited from hospitals, clinics, or research centers in the area where each group convened. Participants in each of the focus groups met the following inclusion criteria: (1) 18 years or older; (2) amputation of the lower limb between the hip and ankle; (3) use of a lower limb prosthesis; (4) able to read, write, and understand English; and (5) agree to have the focus group discussion recorded and transcribed. Participants also had to travel to one of the focus group locations. Candidates were excluded from participation if, in the opinions of the investigators, they had a medical, psychiatric, or a cognitive condition that would interfere with completing a self-administered questionnaire or participating in a group discussion.
The participants were purposively sampled to reflect a range of characteristics deemed relevant to mobility with lower limb prostheses. 9 To ensure diverse perspectives, enrollment targeted participants with different limbs, levels, and etiologies of amputation as well as those of different genders, races, ethnicities, and ages. Specifically, at least two participants with the following characteristics were recruited for participation across all focus groups: (1) transfemoral (i.e. above-knee) amputation, (2) bilateral lower limb amputation, (3) female, (4) age over 50 years old, (5) amputation within the previous year, and (6) amputation due to military service. No more than 12 people were recruited for each focus group to facilitate input from all participants. 9
Procedures
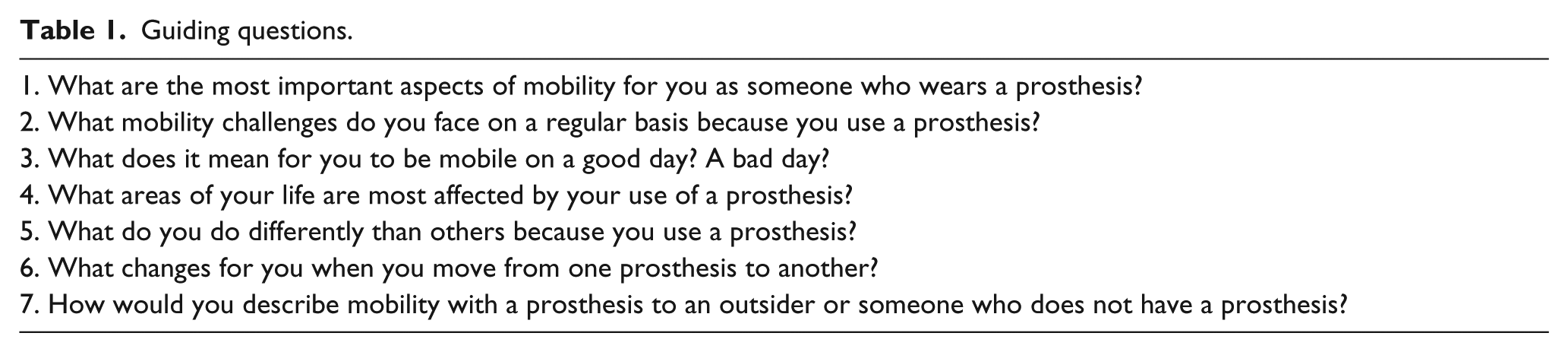
Focus group discussions were approximately 2 h in length. Participants were first asked to complete a brief health and demographic survey. A trained facilitator started each focus group by describing the study purpose and reviewing guidelines developed to facilitate productive and respectful discussions. 9 The facilitator then used a semi-structured approach to encourage discussion of mobility using lower limb prostheses among participants. 13 Guiding questions (Table 1) were used to promote discourse pertinent to specific aspects of mobility with a prosthesis. The facilitator was otherwise nondirective, nonevaluative, and supportive. Toward the end of each focus group, participants were provided a written copy of the investigators’ proposed definition of mobility (i.e. “the ability to move intentionally and independently from one place to another”) for review and comment. The definition of mobility provided to participants was developed through a review of existing definitions (i.e. literature review) and consensus discussions with an advisory panel of researchers, clinicians, end users, and other stakeholders. Focus group sessions were audiotaped and transcribed by a Communication Access Real-time Translation (CART) reporter to facilitate analysis. 14 At least two investigators were present at each focus group to observe and take notes.
Guiding questions.
Analysis
Focus group transcripts were coded, and codes were grouped to identify discussion themes. First, investigators reviewed transcripts from all focus groups to familiarize themselves with the data. They then identified portions of the transcripts related to the proposed definition of mobility. Discussions unrelated to mobility, but related to the experience of living with amputation, were also noted, included in the analysis, and will be published in a separate article. Next, two investigators independently indexed the transcripts using initial codes selected by the study team to describe different aspects of mobility (e.g. uneven terrain and distance). Transcripts were coded using ATLAS.ti (Cleverbridge AG, Chicago, IL) qualitative data analysis software. ATLAS.ti was developed to locate, code, and annotate findings in primary data material, evaluate their importance, and visualize the relations between them. Codes were updated and restructured based on discussions with the research team. Finally, two investigators (D.C.A. and S.J.M.) independently reviewed the coded transcripts to identify themes. Themes were used to evaluate the proposed definition of mobility, create a conceptual model, and inform new survey question content related to the mobility experiences described by focus group participants.
Results
One focus group was held in each of the four cities (i.e. Seattle, WA; Puyallup, WA; Chicago, IL; and Miami, FL). Between 6 and 12 people with lower limb amputation participated in each group. A total of 37 participants with a diverse range of characteristics were included in the study (Tables 2 to 4).
Participant characteristics (N = 37).
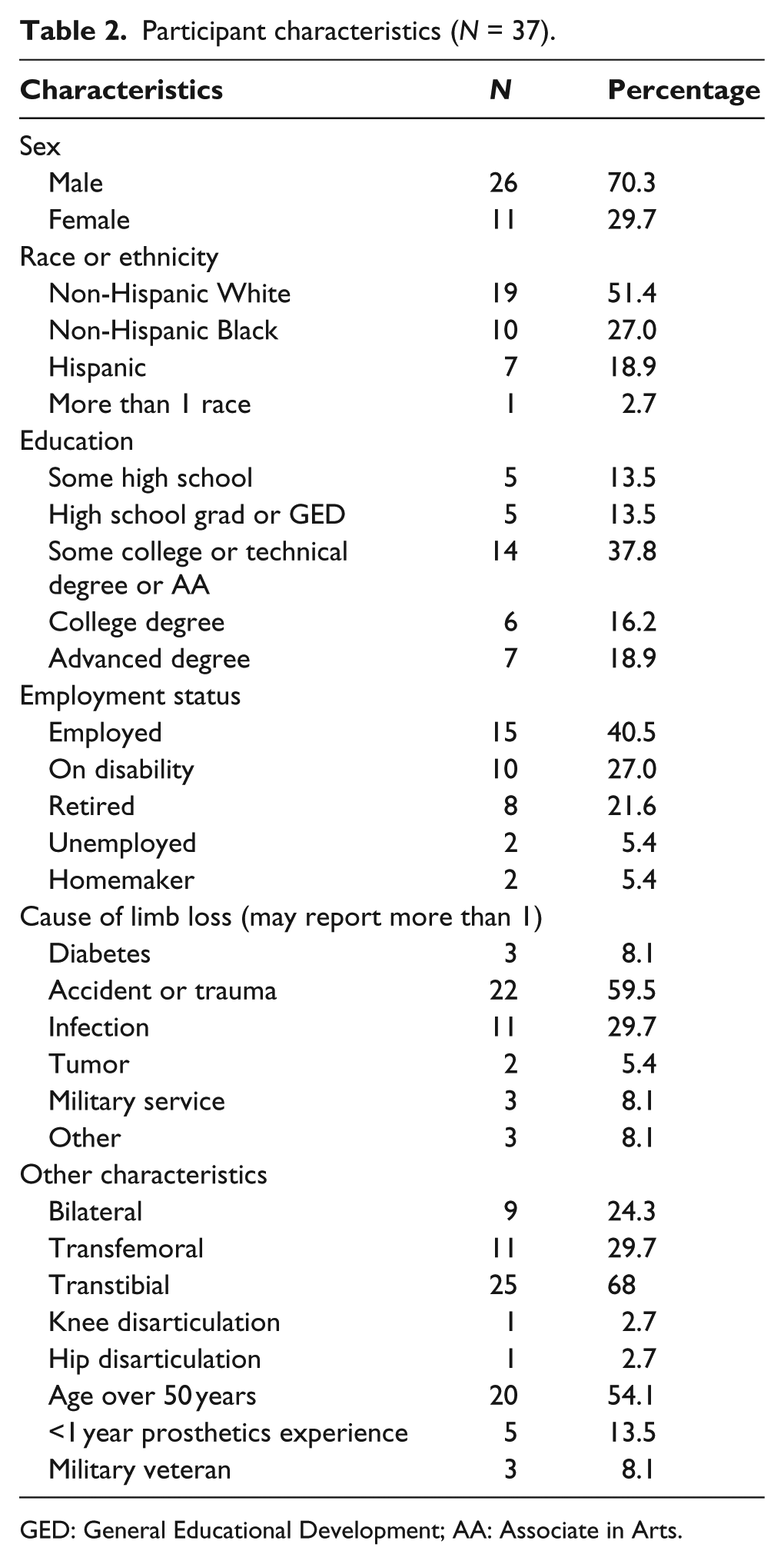
GED: General Educational Development; AA: Associate in Arts.
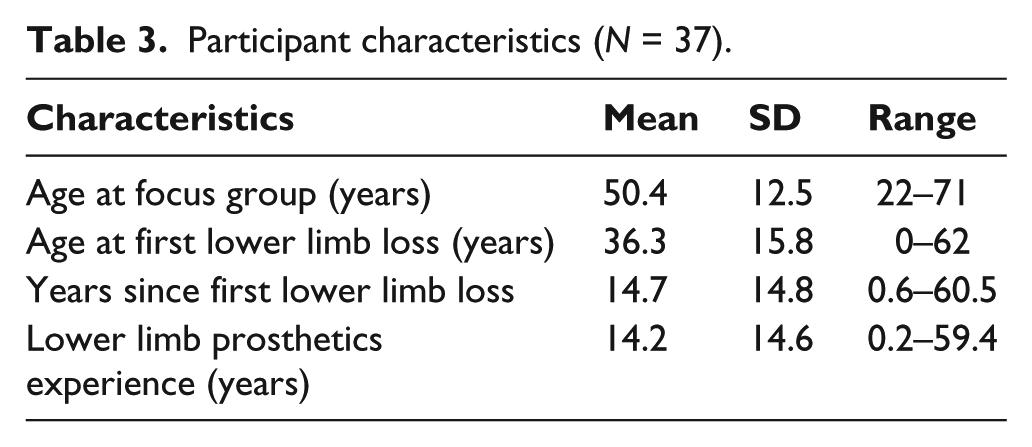
Participant characteristics (N = 37).
Demographic and clinical details for focus group participants.
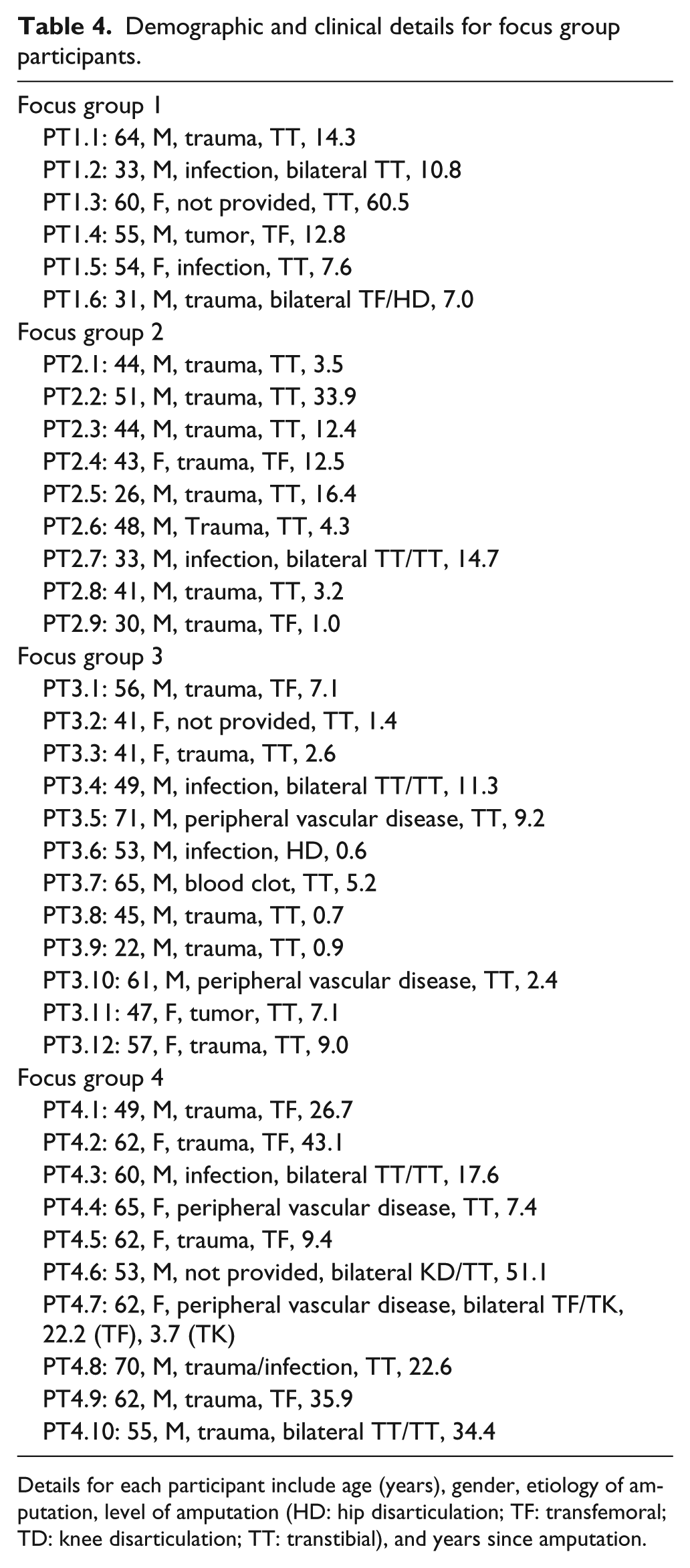
Details for each participant include age (years), gender, etiology of amputation, level of amputation (HD: hip disarticulation; TF: transfemoral; TD: knee disarticulation; TT: transtibial), and years since amputation.
Focus group participants described a wide range of subjects they felt were related to their prosthetic mobility. Upon review and analysis of the transcripts, the investigators identified three primary themes that summarized the focus group discussions: (1) individual characteristics, (2) forms of movement, and (3) environmental situations (Table 5). Descriptions of themes and supportive quotes from the focus group discussions are presented in Table 5.
Themes and categories.
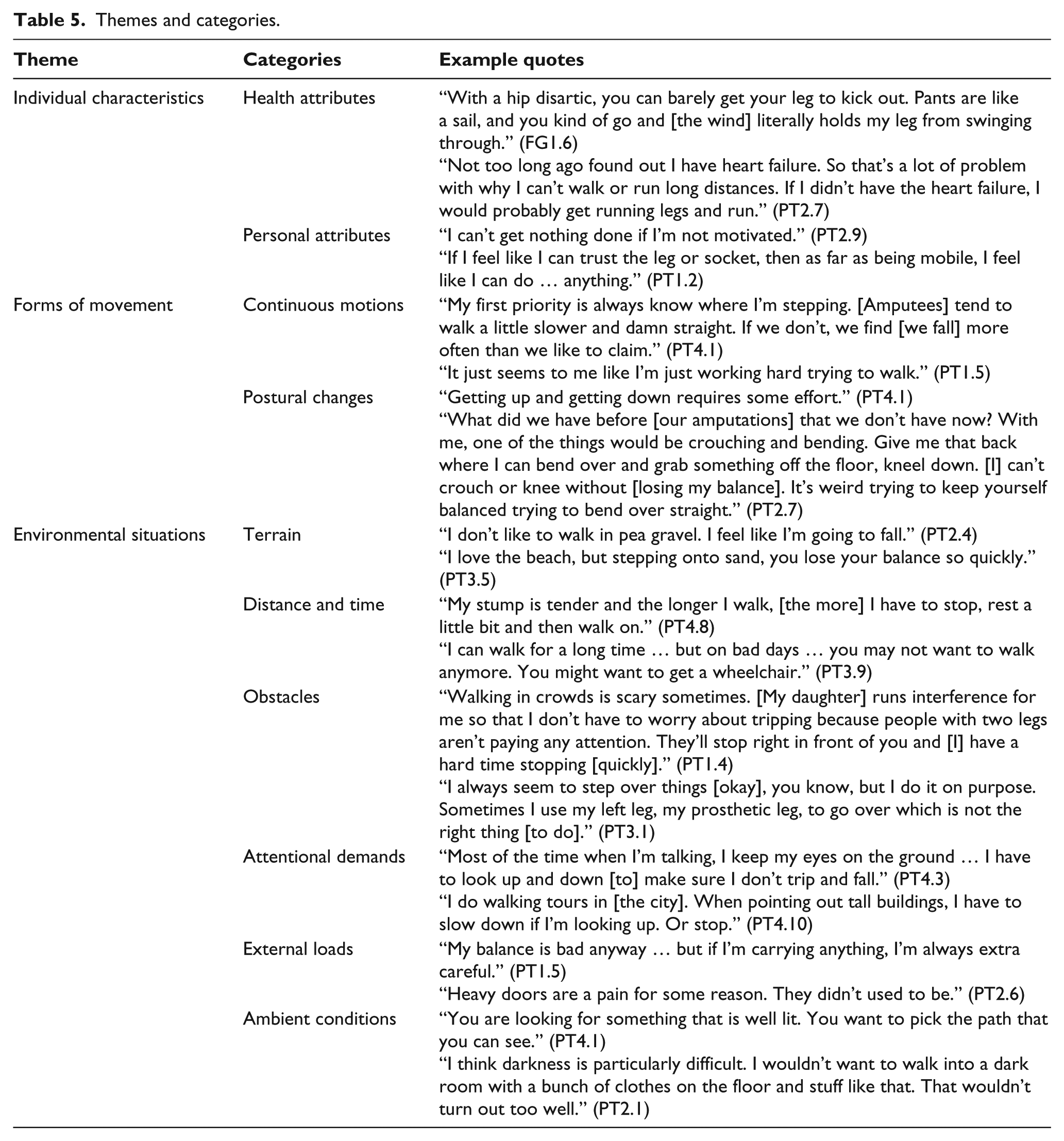
Individual characteristics
The theme of individual characteristics included personal characteristics of people with lower limb loss and aspects of their health that affected their ability to move. Individual characteristics fell into two primary categories: health attributes and personal attributes.
Health attributes
The influence of each individual’s limb amputation and comorbid impairments on prosthetic mobility was a common topic in all focus groups. Participants with multiple or high-level (i.e. proximal) amputations noted that they faced mobility challenges they believed were directly related to their type of physical impairment(s): For one thing, I can’t go upstairs because I have [an] above the knee [amputation]. (PT3.1) I’m a double amputee. It is difficult for me to sit in certain places. I always have to look down before I can get up so I could see my feet. (PT4.3)
In addition, focus group participants often expressed that pain or discomfort negatively affected mobility with a prosthesis: First of all, you [do] less activities than you would normally because, say like you planned to go to the mall or you planned to go to the beach or something and you are having a bad day or in pain with your stump. Of course you wouldn’t do it that day and you would be a little grouchy, you know, because the pain is irritating and you would be less active in your normal day. (PT3.11) I find when my prosthetic is very comfortable, I can go out and run, I can do everything I need to do. As soon as I start getting a sore or rubbing somewhere, I’m not as apt to get up and do what I need to do. (PT3.2)
Personal attributes
Individual qualities such as motivation to be active or trust in one’s prosthesis were often considered to have an effect on mobility. Some focus group participants attributed mobility to their ability to self-motivate: If you complain, [the prosthesis is] not going to move. Just like if you don’t put gas in a car, it’s not going to go anywhere. But if you work hard at it and just think of what you want [and believe] that nothing is going to stop me, that’s the determination that I have. (PT3.12) The time I first got my prosthesis, in seven days I was walking because I motivated myself to move. (PT2.9)
Trust in the prosthesis or a particular component was also linked to changes in participants’ perception of mobility. Conversely, when the prosthesis behaved or moved unpredictably, participants reported limiting their mobility in order to bolster their feelings of safety and security: I didn’t trust the first prosthesis that I had because I didn’t know [how to use it] … It took a while for me to trust it, and the more I began to do activities, the more relaxed I became. (PT3.8) I had a first leg my first knee was a hydraulic knee, and that had certain limitations … Then, I got a C-Leg which is [an] electronic [knee] and that’s a lot more mobile. I mean, I can do almost anything that I choose to do. (PT1.4)
Forms of movement
Forms of movement were defined as mobility-related tasks or activities described by focus group participants. Two primary forms of movement, continuous motions and postural changes, were identified.
Continuous motions
Many participants described challenges with activities that involved constant or continuous motion, such as walking or running: Sometimes I have to really concentrate on the ability to walk because [I’m] sore or the terrain is bad. I’m concentrating on walking rather than what’s going on around me. My sole focus is the ability to get one step in front of the other. (PT1.3) My biggest problem was teaching my daughters about riding a bike and running alongside them for a long distance … I could run a few feet, but wasn’t running a block or anything like that. (PT4.6)
Postural changes
Participants also described challenges with changing posture or position such as sitting down in a confined space or squatting: Getting out of a back seat of a car is very difficult. I have to put one foot in and then I have to put my [other] foot under the front seat and lift [my prosthesis into the car]. When I’m getting out, I’m stuck. (PT4.3) Being in a booth at a restaurant and having to slide in or slide out of the booth is a pain. (PT1.1)
Environmental situations
Environmental situations were defined as qualities of the setting in which the described tasks or activities were performed by focus group participants. Six categories of environmental situations were identified and were coded as terrain, attentional demands, obstacles, distance or time, external loads, and ambient conditions.
Terrain
When asked about mobility challenges, participants frequently noted that ground or surface conditions affected their ability to walk: You have to be a lot more careful, especially if you’re not walking on any kind of level ground. It’s a lot more difficult. (PT1.4) Slippery surfaces scare me into immobility. [I] just stay in the house until [the ice] goes away. (PT4.4)
Participants also discussed how terrain had the potential to limit their involvement in recreational activities: I haven’t been to the beach in eight years and I love the beach. But stepping onto sand, you lose your balance quickly. [So], I just stopped going to the beach. (PT3.5)
Attentional demands
Participants discussed how attending to another activity while walking was a challenge because their focus could be drawn away. A common example was walking and talking on a cell phone: If I’m walking and the phone rings, I have to stop. Lots of people pick up the phone and keep walking. I’m not going to keep walking and talk at the same time. (PT4.3)
Participants also described how walking and conversing with friends was challenging because they could not look at another person while walking: For amputees, we’re not talking back and forth when we are walking … there is not a lot of eye-to-eye contact. (PT4.1)
Other environmental situations
Other situations that were found to limit mobility included obstacles on the ground, having to walk quickly, walking long distances, carrying objects while moving, and challenging ambient conditions. Examples are provided in Table 5.
Mobility definition
Most participants agreed that the investigators’ developed definition was meaningful and comprehensive. Questions and comments about the provided definition primarily focused on two key terms, intentionally and independently.
Intentional movements
Participants generally understood that the term “intentional” was meant to reflect purposeful or volitional movements and to avoid unwanted events, such as falls: Does [“intentional”] leave the aspect of falling out of the definition [of mobility]? (PT1.6)
Others endorsed the concept of intentional movements by stating that mobility is goal oriented: I would be tempted to add something to [a definition of mobility] about the ability to accomplish wanted or needed tasks. (PT2.6)
Independence
Participants confirmed the investigators’ intention of independence by illustrating that mobility tasks performed with the help of others differed from when they did them alone: If I’m by myself, I’m probably a little more cautious. I would probably wait [to cross the street]. If I was with someone else, I would either take their arms or they kind of inspire me to walk faster because they’re a little bit in front of me, which is common. (PT1.5)
Discussion
The purpose of this study was to better understand mobility with a prosthetic limb from the users’ perspectives and to guide development of PLUS-M, a PROM intended to measure prosthetic mobility. Qualitative methods similar to those used in this study (e.g. thematic analyses of participants with limb loss) have been used previously to examine the psychosocial experience of coping or living with amputation. Qualitative researchers typically employed one-on-one interviews with prosthetic limb users, rather than group discussions. 15 Relatively few studies across the body of qualitative research (in prosthetics) have specifically applied focus groups to study the experiences and perceptions of prosthesis users. However, the use of focus groups has grown more common in the last decade.
Focus groups of people with limb loss have been used recently to examine the benefits of prosthetic prescription, 5 revise a satisfaction questionnaire, 16 and study the effects of back 17 and phantom limb 18 pain after amputation. People with limb loss have also been included in focus groups with nonamputees to study psychosocial adjustment and coping strategies across a range of medical conditions19–21 and to discuss the prosthetic needs of veterans. 22 However, application of focus groups to the formal development of outcome instruments specific to people with limb loss remains uncommon. To the authors’ knowledge, only one other effort to develop a PROM specific to people with limb loss involved use of focus groups to inform development of the conceptual model. Gallagher and MacLachlan23,24 used thematic analysis of focus group discussions to develop the conceptual model for the Trinity Amputation and Prosthesis Experience Scales (TAPES). Here, we applied focus groups in a similar manner to inform development of a conceptual measurement model, key definitions, and survey items for PLUS-M.
Discussions among focus group participants demonstrated clearly the complexity of mobility with a prosthetic limb. Participants’ discussions of mobility were categorized into three themes: individual characteristics (i.e. the physical and psychological attributes of the prosthetic limb user), forms of movement (i.e. the type of mobility task or activity being performed), and environmental situations (i.e. the setting or context in which the activity was performed). Of these, forms of movement and environmental situations were the most relevant to development of standardized PROM items for measuring prosthetic mobility across a range of individuals. Individual characteristics, such as motivation, confidence, comorbid conditions, and symptoms (e.g. pain), clearly influence mobility and are important to measure along with mobility.
The focus group themes, forms of movement and environmental situations, were, therefore, used to establish an initial PLUS-M measurement model (Figure 1) and define inclusion criteria for instrument items. PLUS-M items would need to possess two fundamental characteristics: a specific activity (e.g. “walking”) and a specific setting or context (e.g. “a parking lot” or “when you are bumped into”). These criteria were subsequently used to guide the search for existing mobility items and to create new items that could potentially be included in the PLUS-M instrument. As an example, questions such as “are you able to walk?” were not included in the candidate PLUS-M item bank, but questions such as “are you able to walk a short distance in your home?” were included in the candidate bank.
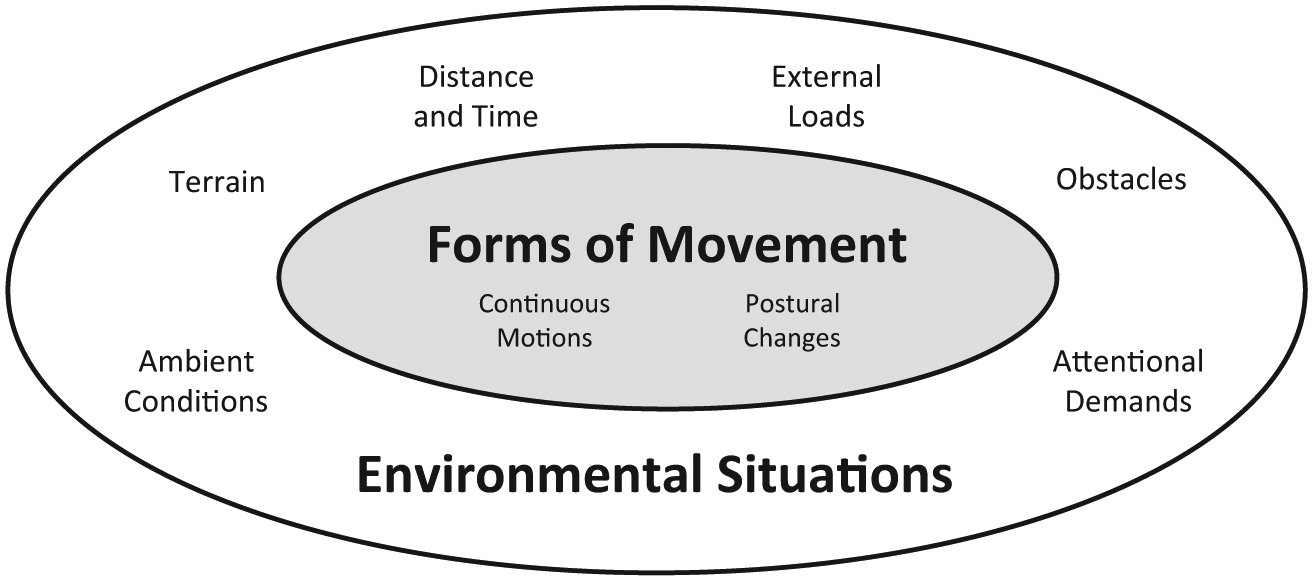
Initial PLUS-M measurement model. Mobility is conceptualized in this model as a form of movement (i.e. task or activity) performed within an environmental situation (i.e. setting or context).
Characterizing mobility as an activity performed within a situational or environmental context is in alignment with existing mobility frameworks; 25 the International Classification of Functioning, Disability, and Health (ICF); 26 and the classification system27,28 used by the US Centers for Medicare & Medicaid Services (CMS) to determine prosthetic users’ eligibility for prosthetic componentry. The environmental situations described by focus group participants in this study (Table 5) were notably similar to dimensions of community mobility (i.e. minimum walking distance, time constraints, ambient conditions, terrain characteristics, external physical loads, attentional demands, postural transitions, and traffic level) described by Patla and Shumway-Cook. 25 A key difference between these dimensions and the categories derived in this study is how postural changes are classified. Patla and Shumway-Cook categorized postural transitions and other environmental conditions, such as terrain and time constraints, as dimensions. Here, the authors elected to classify postural changes (and continuous motions) as forms of movement, distinct from environmental situations. “Walking and moving” and “changing basic body position” are similarly classified together as mobility activities in the ICF framework. 26 The CMS classification system also describes activities in an environmental context, as evidenced by terminology such as “ambulation on level surfaces” and “ability to traverse low level environmental barriers such as curbs, stairs, or uneven surfaces.”27,28 General agreement among prosthetic users’ views on mobility and descriptions included in established classification systems may indicate that prosthetic mobility can be characterized in this manner.
The investigators considered the individual characteristics to be separate from the construct of mobility. However, focus group participants had a notably holistic view of mobility. This comprehensive view of health outcomes is consistent with perspectives reported by both prosthetic users 5 and nonamputees 29 in similar studies. These common, holistic perceptions of health suggest that measurement of mobility, as conceptualized here, should be complemented by measurement of related health outcomes (e.g. balance confidence and pain) in order to fully understand experiences of prosthetic limb users in a way that is consistent with how they perceive their own mobility. The use of other valid and reliable instruments (e.g. PROMIS) that span a range of domains may also be useful for evaluating and documenting patients’ perceptions of their health. 30
Limitations
It is recognized that individuals with strong personalities may disproportionately contribute to discussions in a focus group.4,31 The investigators attempted to address this potential limitation by encouraging all participants to voice their experiences 2 and by following up on gestures, such as nodding or changes in facial expression. Additionally, short responses that indicated agreement, such as “yeah,” or “me too,” were captured in transcripts and included in the analysis of focus group discussions.
Discussions may also be limited by the perspectives of those selected to participate. 32 As with any nonrandom small sample, caution is recommended when generalizing these results to the overall population of prosthetic limb users. Here, purposive sampling was used to obtain a broad spectrum of participant characteristics and to solicit a range of experiences in each focus group. In such cases, it is methodologically appropriate to recruit individuals who possess traits of interest to the goals of the research, rather than to recruit participants who reflect the exact characteristics of the target population. 9
The presence of health-care providers or others of authority may affect focus group discussions.9,33 Three of the four focus groups in this study included investigators or observers who provided prosthetic care for select participants. Participants may have been more conscious of the tone or content of their comments due to the presence of these providers. Alternatively, provider attendance may have enhanced participants’ comfort and allowed them to share their experiences more openly. Investigators attempted to mitigate this potential limitation by hosting the focus groups at neutral locations and encouraging open, honest dialogue. 2
Conclusion
The results of this study were used to establish a preliminary framework for the PLUS-M instrument. Based on the identified themes and potential for standardization of experiences across persons with lower limb loss, the investigators described mobility as activities performed within a situational or environmental context. Future efforts will be directed toward identifying existing PROM items that may be suitable for inclusion in the instrument or to developing new PLUS-M items, based on experiences described by participants in this study.
Footnotes
Acknowledgements
The authors would like to thank Kurt Johnson, PhD, for serving as a focus group facilitator. The authors would also like to thank Greg Davidson, CPO; Stefania Fatone, PhD; Robert Gailey, PhD, PT; and Ignacio Gaurnaurd, PhD, PT, for their help in identifying candidate focus group participants at each of the study locations.
Author contribution
The authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interest
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child and Human Development of the National Institutes of Health under award number HD065340.