
Abstract
Background:
Individuals with leg amputations who use passive prostheses have greater metabolic demands than non-amputees likely due to limited net positive work compared to a biological ankle. New powered ankle–foot prostheses can perform net positive mechanical work to aid push-off capabilities, which may reduce metabolic demands.
Objectives:
Compare step-to-step transition work and metabolic demand during level and inclined walking using passive and powered ankle-foot prostheses.
Study Design:
Repeated measures.
Methods:
Six individuals with transtibial amputation and six able-bodied controls walked at a standardized speed across level ground and up a 5° incline. Calculated measures included mechanical work during step-to-step transitions from the trailing prosthetic to leading intact limb, steady state metabolic rate, and ankle joint kinetics and kinematics.
Results:
The powered prosthesis generated 63% greater trailing limb step-to-step transition work than the passive during level walking only (p = 0.004). Metabolic rate was lower with the powered prosthesis during level (p = 0.006) but not inclined walking (p = 0.281). The powered prosthesis increased ankle power compared to the passive, to the extent that power was normalized to controls during inclined walking and greater than controls during level walking.
Conclusion:
The powered prosthesis improved ankle power, metabolic rate, and step-to-step transition work on level ground, with few negative consequences on inclines. These results may be used to guide the development and use of actively powered prosthetic devices in high-functioning individuals.
Clinical relevance
Overall, powered devices offer biomechanical and metabolic benefits over passive energy storage and return designs on level ground and perform as well as a passive model on inclines. The lower metabolic demand when using the powered device may delay fatigue for individuals with transtibial amputation when walking over level ground.
Background
Active ankle plantarflexion is an important contributor to forward propulsion during walking. To propel the center of mass (COM) upward and forward during walking, the trailing limb’s ankle plantarflexors contract and the Achilles tendon returns stored energy to generate positive ankle joint work during push-off (up to 80% of the total work).1–3 This positive work performed by the trailing limb is required to overcome the mechanical energy losses that occur during the collision of the leading limb as it accepts the weight of the body and dissipates energy during step-to-step transitions. Leading limb energy losses are an important determinant of, and are correlated with, the metabolic cost of transport during walking, 4 as they determine how much positive work must be generated from the trailing limb. The trailing limb push-off power, particularly the ankle joint, can help reduce these collisional losses and maintain a relatively low metabolic demand.5,6
However, when trailing limb push-off capabilities are compromised (i.e. reduced positive work), energy losses occur through energy dissipation (i.e. negative work) of the leading limb. For example, the absence of ankle joint musculature and the use of a prosthetic device, as occurs following lower limb transtibial amputation (TTA), decrease the positive work performed by the prosthetic trailing limb during push-off.5,7 This compromised push-off may lead to compensations at other joints and greater energy loss during the collision of the contralateral limb relative to able-bodied individuals.3,8,9 Walking economy is thus affected and individuals with amputations require 10%–30% more gross metabolic energy than able-bodied individuals at the same walking velocity.10–12
Energy storage and return (ESR) prostheses are worn by a majority of ambulatory individuals with TTA and are designed to provide some of the functions of a biological ankle. Although prosthetic technology has improved over the years to provide greater energy return capabilities3,13 than traditional models (e.g. solid ankle cushion heel (SACH) foot), ESR prostheses are still inferior to the biological limb during the push-off phase of walking.14–16 One of their drawbacks is that they produce less than half the ankle joint work of an intact ankle,17,18 which evokes greater leading leg collision cost. 5
Compared to passive ESR prostheses, novel powered prostheses are designed to better emulate biological ankle function as they supply active push-off power and can generate net positive trailing limb work. 7 In general, an increase in ankle power at push-off has the potential to increase self-selected walking velocity7,16 and decrease metabolic cost.5,7 However, it remains inconclusive if powered prostheses can restore normative walking kinematics and energetics over level ground.7,16
In contrast to level walking, walking up an incline requires more overall positive work from the trailing limb during push-off 19 to increase the potential energy of the body and thus more metabolic energy. 20 While several groups have investigated inclined walking using ESR prostheses,21–23 biomechanical and metabolic parameters of inclined walking with powered prostheses are relatively unexplored. Ankle power generation from an actively powered ankle–foot prosthesis may be particularly useful during inclined walking when greater push-off power is desired compared to level walking.
The purpose of this study was to compare both mechanical work on the body’s COM during step-to step transitions from the prosthetic to intact limb and metabolic demand between ESR and powered ankle–foot prostheses during level and inclined walking. A second purpose of this study was to determine whether a powered prosthesis normalizes walking mechanics and metabolic demand to able-bodied individuals. We hypothesized that, compared to the ESR prosthesis, the powered prosthesis would result in greater positive trailing limb work during step-to-step transitions and lower negative leading limb work and a lower metabolic demand over level and inclined walking. Furthermore, we hypothesized that the use of a powered prosthesis would normalize peak ankle power, step-to-step transition work, and metabolic demand to able-bodied individuals.
Methods
Subjects
A repeated measures study design was used to compare ESR and powered prosthetic device. A total of 12 subjects with traumatic unilateral TTA who were ambulatory for at least 2 months were initially enrolled in the study, but half had step lengths that were either too long or too short to fully contact each of the force platforms on the inclined walkway without adjustments. Therefore, six subjects were necessarily excluded from this analysis (Table 1). TTA was matched on gender and body mass index to six able-bodied control subjects. All subjects provided written informed consent to participate, and study investigations were approved by and in accordance with the policies set forth by the Institutional Review Board.
Subject characteristics.
TTA: transtibial amputation; ESR: energy storage and return; SD: standard deviation.
Experimental setup
The experimental setup for level ground walking consisted of a 26-camera motion capture system (120 Hz; Motion Analysis Corp, Santa Rosa, CA) with five centrally located force platforms in tandem (1200 Hz; Advanced Mechanical Technology, Inc. (AMTI), Gothenburg, Sweden). Inclined walking was assessed using a 5-m long incline of 5°, with two force platforms in tandem (1200 Hz; AMTI, Watertown, MA). Metabolic demand was assessed as the steady state rate of oxygen consumption (V̇O2). As subjects breathed into a plastic mask that sealed around the nose and mouth, a portable metabolic unit recorded V̇O2 using indirect calorimetry and 30-s averaging (model K4B2; COSMED, Inc., Rome, Italy).
Experimental device
Patients were initially assessed using their prescribed ESR device. Subjects were then fit with the powered prosthesis (Figure 1) (BiOM; iWalk, Cambridge, MA) by a certified prosthetist. BiOM ankle parameters, including ankle joint power production, timing of push-off power, toe-off ankle angle, net non-conservative work, and foot stiffness, were tuned by an iWalk representative to patient preference within normative reference ranges. Comprehensive details of the BiOM can be found in the literature.7,24,25 Subjects were instructed to wear the device integrated with an ESR foot for 3 weeks to allow for acclimatization prior to returning to the laboratory for assessment.

A bionic powered ankle–foot prosthesis (BiOM).
Protocol
During data collection, 57 spherical, retro-reflective markers were secured to anatomical landmarks and segments of the limbs, pelvis, torso, and head. 26 A digitization pointer (Visual3D; C-Motion, Inc., Germantown, MD) identified the medial and lateral malleoli and femoral epicondyles to calculate intact joint centers. The ankle joint center of the BiOM was calculated from digitized points on the medial and lateral aspect of the BiOM’s axis of rotation. For the ESR device, the position of the ankle joint center in the intact foot coordinate system was mirrored into the foot coordinate system of the prosthetic limb.
Subjects walked at a standardized velocity (±5%) based on leg length and a dimensionless Froude number of 0.16 (1.24 ± 0.05 m/s for TTA and 1.21 ± 0.03 m/s for controls), over level ground and up the inclined walkway. 27 The Froude number of 0.16 was chosen because it approximates an average self-selected walking velocity for able-bodied individuals and is attainable for individuals with amputations. 16 Three successful trials in which the prosthetic limb and then the intact limb contacted consecutive force platforms were recorded. Additionally, subjects walked at the standardized velocity on a treadmill for at least 6 min or until steady state metabolic rate was achieved for both level and inclined walking.
Data analysis
Biomechanical data were analyzed in Visual3D (version 4.96.7; C-Motion, Inc., Germantown, MD). Raw marker data and analog data were filtered using a fourth-order, low-pass Butterworth filter with cutoff frequencies of 6 and 50 Hz, respectively. Ankle joint angles were calculated and internal joint moments and powers were calculated using an inverse dynamics approach. Segmental inertial parameters were obtained from Dempster, 28 and the prosthetic foot and leg were each modeled using the properties of a biological limb. 29 Step-to-step transition work during the entire period of double support was calculated for the leading (intact) and trailing (prosthetic) limbs independently according to the individual limbs method. 4 Integration constants for overground walking were chosen such that the average vertical velocity over a step was zero, the average fore–aft velocity was equal to the forward velocity of the kinematic COM, and the medio-lateral velocities at the beginning and end of a step were equal in magnitude and opposite in sign. Integration constants were adjusted for inclined locomotion 30 such that the fore–aft and vertical COM velocities were equal to the whole-body COM velocities calculated from the kinematic model. Calculations on biomechanical measures were performed on individual trials, and resultant values were averaged within a subject. V̇O2 data were averaged over the final 2 min of each trial and scaled to biological body mass.
Statistical analysis
Effect sizes (d) were calculated as per Cohen, 31 and large effect sizes (d > 0.80) will be regarded as a meaningful difference between two groups. A one-way analysis of variance (ANOVA) with Tukey’s post hoc tests compared the BiOM and ESR to the able-bodied control group (p < 0.05) (SPSS version 19; IBM, Sommers, NY). Paired t-tests compared between the ESR and BiOM. The p-values were included to supplement effect sizes.
Results
Step-to-step transition work
During level walking, the net step-to-step transition work done by the trailing prosthetic limb was 63% greater for the BiOM (0.275 ± 0.068 J/kg) versus ESR (0.168 ± 0.025 J/kg) prosthesis (p = 0.004, d = 2.094) (Figures 2 and 3). The BiOM trailing limb step-to-step transition work was also 28% greater than controls (p = 0.186, d = 1.231), while the ESR was 22% less than controls (p = 0.327, d = 0.982). Net leading limb work (sum of both positive and negative work) during step-to-step transitions was not different between prosthetic devices or between TTA and controls.
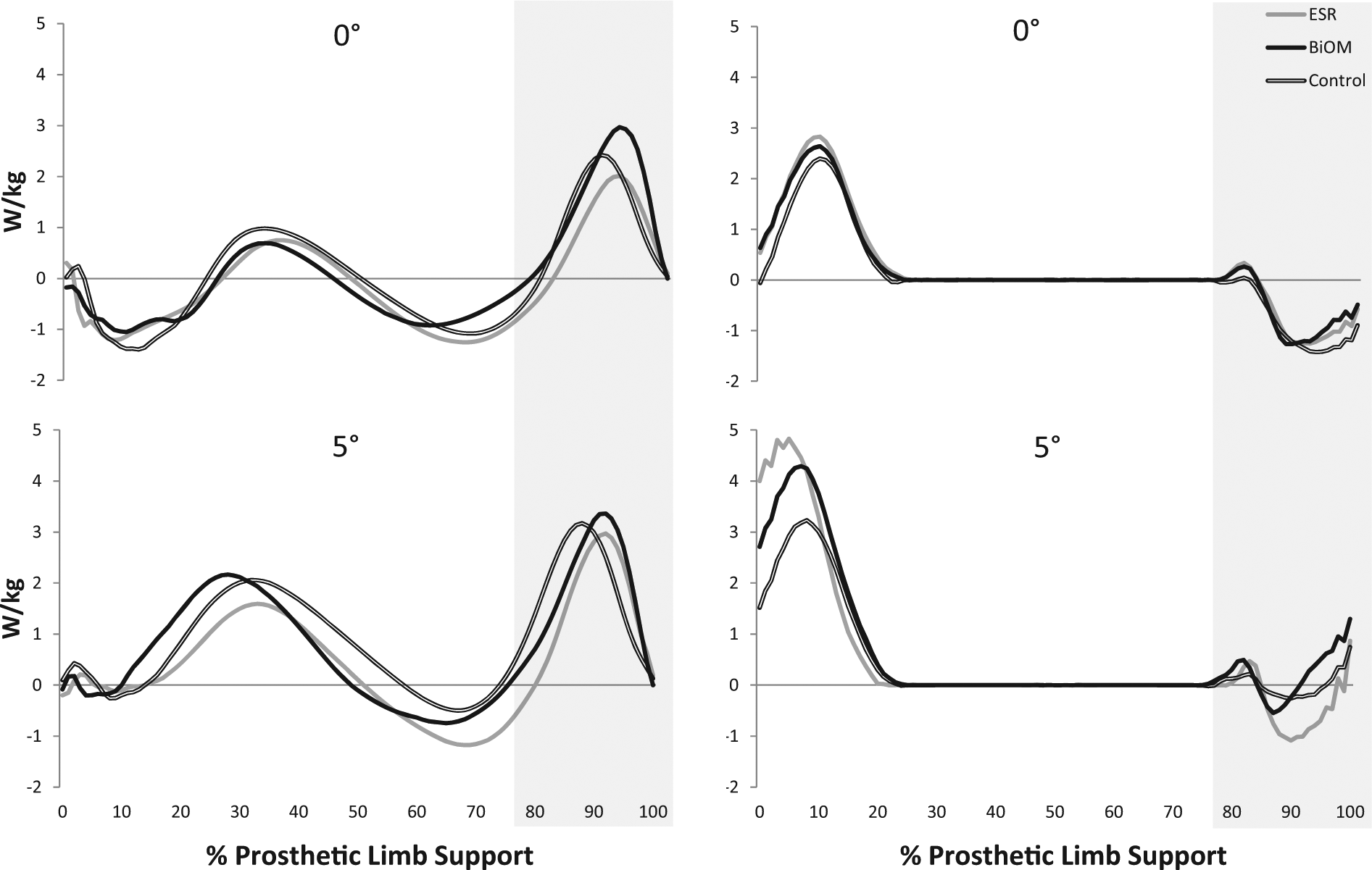
Prosthetic trailing limb and intact leading limb power during the single-limb support phase of the prosthetic limb.
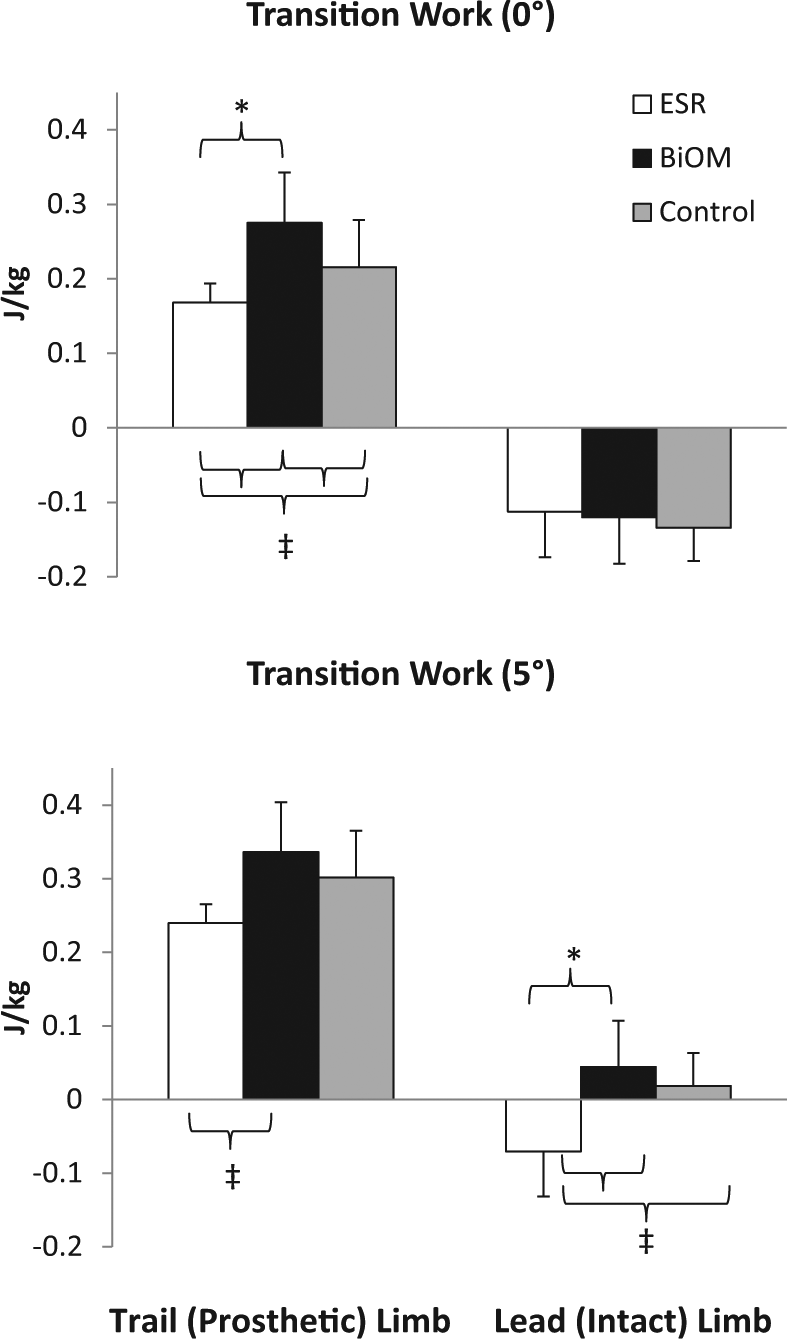
Average step-to-step transition work of the leading (intact) and trailing (prosthetic) limbs when using the powered prosthesis (BiOM), the energy storage and return (ESR) prosthesis, and for control subjects.
During inclined walking, the net trailing prosthetic limb step-to-step transition work was, on average, 53% greater for the BiOM relative to the ESR (ESR: 0.240 ± 0.106 J/kg, BiOM: 0.336 ± 0.118 J/kg, p = 0.144, d = 0.858). Net trailing limb step-to-step transition work did not differ between control subjects and TTA in either device during inclined walking.
Metabolic rate
During level walking, V̇O2 was 16% lower with the BiOM versus the ESR prosthesis (p = 0.006, d = 2.213) (Figure 4). ESR users experienced 9% greater metabolic rates than able-bodied individuals (p = 0.107, d = 1.213), but the BiOM normalized metabolic rates (p = 0.384, d = 0.763). On the incline, metabolic rates were not different between BiOM users and controls or between the BiOM and ESR. However, two TTA subjects experienced an increase in V̇O2 during inclined walking with the BiOM relative to the ESR (15% and 6% increases). ESR use increased V̇O2 by 6% relative to controls on the incline (p = 0.139, d = 0.927).
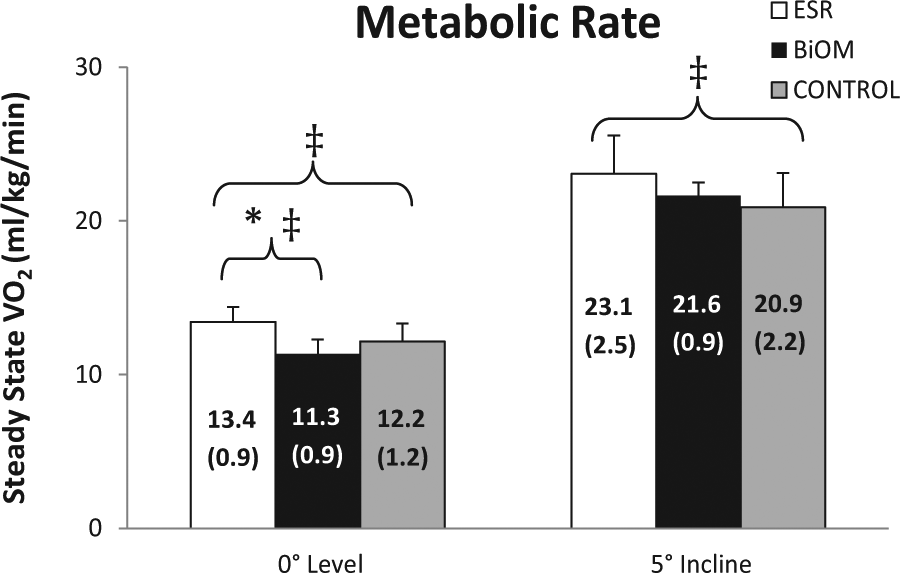
Average (standard deviation) steady state metabolic rate during walking using the powered prosthesis (BiOM) and energy storage and return (ESR) prosthesis during level (0°) and inclined (5°) walking.
Kinetics and kinematics
During level ground walking, the BiOM increased peak ankle plantarflexion angles (p < 0.001, d = 4.603), and powers (p = 0.001, d = 2.948) at push-off relative to the ESR (Figure 5) and decreased peak internal plantarflexor moments (p = 0.064, d = 1.411). During inclined walking, peak angles (p < 0.001, d = 3.481) and powers (p = 0.003, d = 2.432) were greater in the BiOM. Peak ankle plantarflexion angles (p < 0.001, d = 3.037) and powers (p = 0.044, d = 2.197) were lower in the ESR than controls over level ground, and angles (p < 0.001, d = 3.678), moments (p = 0.260, d = 0.839), and powers (p = 0.043, d = 1.904) were lower on the incline. The BiOM normalized the peak ankle plantarflexion angles on level ground (p = 0.487, d = 0.592), but moments remained lower (level: p = 0.269, d = 0.802; incline: p = 0.385, d = 1.343) and powers higher (level: p = 0.030, d = 1.436; incline: p = 0.181, d = 0.998) than controls during both level ground and inclined walking.
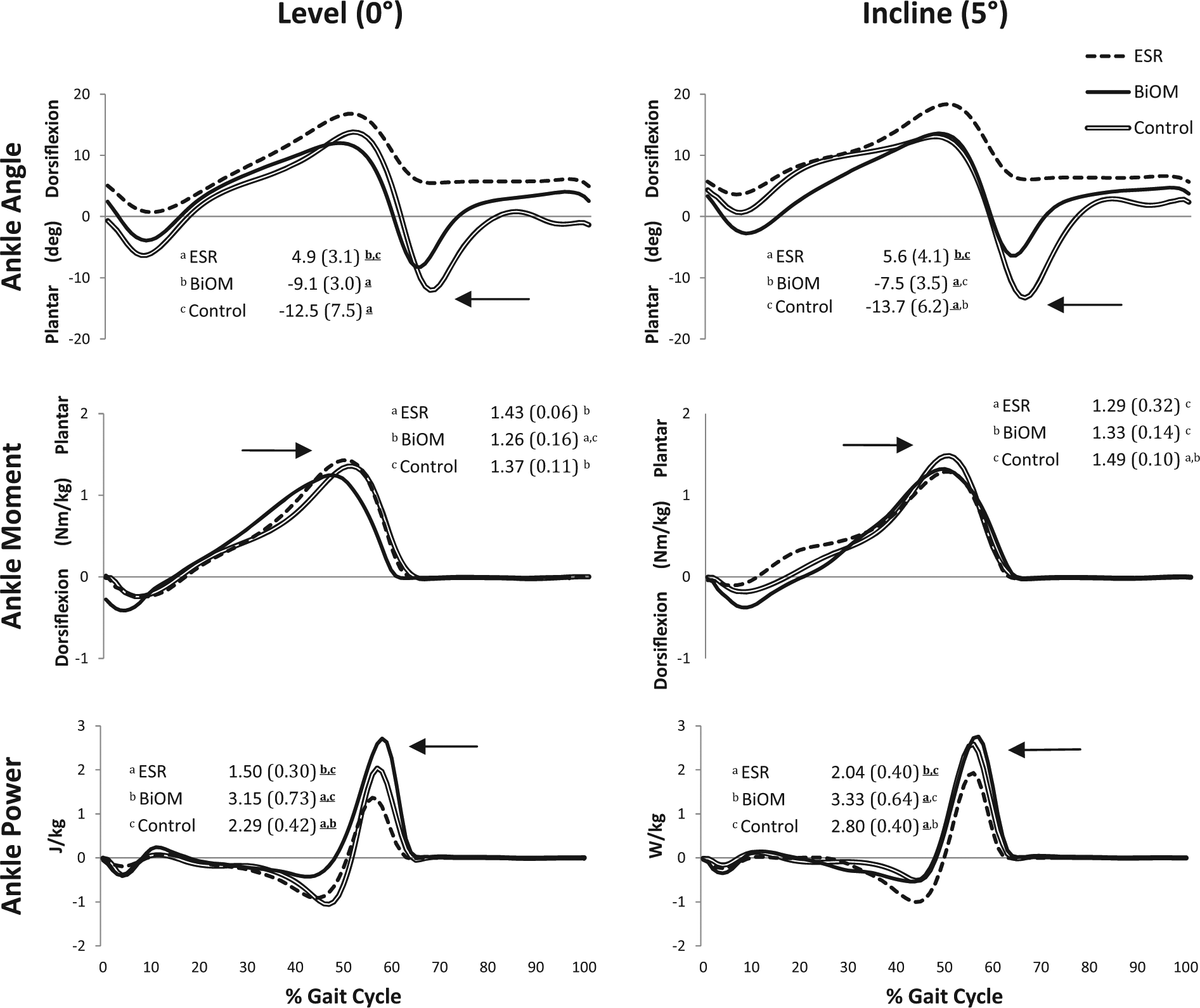
Average (standard deviation) sagittal plane joint angles, internal moments, and powers for the powered prosthesis (BiOM), the energy storage and return (ESR) limb, and the able-bodied subjects.
Discussion
The purpose of this study was to compare biomechanical and metabolic parameters between passive and powered ankle–foot prostheses during both level and inclined walking. In partial support of our first hypothesis, and in agreement with Herr and Grabowski, 7 the powered BiOM prostheses improved ankle power, net trailing limb mechanical work during the double support phase of the step-to-step transitions, and V̇O2 compared to a passive ESR prosthesis on level ground. These data are consistent with Winter 1 in that the ankle is largely involved in trailing limb push-off work during step-to-step transitions and provides support for use of powered prostheses. The battery-powered assistance provided by the BiOM supplied the necessary means of increasing ankle push-off power without incurring an associated metabolic cost. However, metabolic advantages of the BiOM compared to the ESR were only found over level ground walking, not inclined.
On the incline, although there was a large effect size for increased trailing limb push-off work and ankle joint power, combined with reduced leading limb energy dissipation in the BiOM compared to the ESR, V̇O2 did not decrease. Segal et al. 32 also found that prosthetic feet capable of restoring push-off energy and reducing leading limb energy dissipation during collisions did not produce significant reductions in metabolic rate. In addition, compensations at the hip throughout the gait cycle likely contributed to the elevated V̇O2. Of the two subjects in this study who experienced greater V̇O2 in the BiOM relative to the ESR during inclined walking, one experienced no change in trailing limb push-off work between devices, while the other experienced a large increase and had the greatest calculated value of all subjects. It is likely that insufficient tuning for powered plantarflexion assistance on the incline resulted in the low BiOM work during step-to-step transitions in the first subject and over-powering of the device affected the excessive work during transitions in the second subject. Thus, optimal or near-optimal tuning of the BiOM is crucial to obtain a positive effect on V̇O2.
Push-off from the trailing limb during double support can best regenerate the energy lost during collision of the leading limb.5,17 As expected, powered push-off from the BiOM reduced mechanical energy losses of the leading intact limb on the incline, but the additional push-off did not affect the leading limb on level ground. These results are contradictory to the hypothesis that an increase in trailing limb step-to-step transition work decreases the energy dissipation by the leading limb. However, Herr and Grabowski 7 found similar results at two of their walking velocities (0.75 and 1.75 m/s) where the increase in trailing limb work provided by the BiOM did not reduce intact leading limb negative work. Therefore, compensation strategies, such as the BiOM replacing the positive work of the ankle muscles, may occur to reduce V̇O2 despite no reduction in leading limb negative work for the collision. It has often been proposed that insufficient push-off power and trailing limb work following TTA increase the energy dissipated by the leading limb during step-to-step transitions. This greater energy dissipation of the leading limb to compensate for deficiencies in the trailing limb push-off increases the metabolic demand during walking. 5 In this study, this was particularly apparent during step-to-step transitions on the incline when the leading limb of the control and BiOM groups generated net positive mechanical energy, while the ESR group dissipated mechanical energy. This result likely contributed to greater V̇O2 of the ESR group relative to the controls. Positive leading limb work is important during inclined walking because it contributes to the upward movement of the COM. 19 The ankle and hip joints primarily contribute to its positive work during uphill walking. 33 TTA was limited in its ability to generate this positive leading limb step-to-step transition work in the ESR, but not BiOM.
In partial support of the second hypothesis, the BiOM normalized level ground step-to-step transition work to able-bodied individuals. Herr and Grabowski 7 also found that the BiOM provided the ankle plantarflexion and power generation necessary to normalize gait to able-bodied subjects over level ground. In this study, although the BiOM provided even greater peak ankle joint power than control subjects and there were large differences between BiOM and control groups for trailing limb step-to-step transition work, metabolic rate was not different between groups. These results may be due to the fact that, although the ankle is primarily responsible for trailing limb work, the BiOM cannot supplement all the functions of a biological lower limb and is fundamentally different. It is monoarticular in nature and can only mimic the activity of the soleus, not biarticular gastrocnemius musculature. This inherent limitation in the device may not allow it to sufficiently replicate intact ankle capabilities and fully restore function. In addition, the timing of push-off power, its magnitude, or a combination of the two may not have been optimal for each user. Despite these limitations, the added push-off power may have been sufficient enough to limit some of the compensatory strategies that incur an added metabolic cost when walking with a prosthesis.
While the BiOM was expected to normalize mechanics and V̇O2 to controls, the ESR was expected to differ from controls across all dependent measures. However, this was not the case during level or inclined walking. Although the ESR contributed less ankle power than an intact ankle, it did not result in significantly less trailing limb step-to-step work and V̇O2 was not significantly greater. This result was contradictory to previous studies that have found greater V̇O2 and lower step-to-step transition work with ESR prostheses.5,7 However, effect sizes were large when comparing between ESR and controls, and the patients in this study were relatively young, healthy, and highly active compared to a general amputee population commonly reported. The authors acknowledge that the sample size may have affected these particular statistical outcomes.
There were several other limitations in this study. First, the independent active and passive contributions of the BiOM were not recorded as part of this study but can be found elsewhere. 7 Next, it is unknown how device tuning specifically affected the results for inclined walking. During the accommodation period, the BiOM was tuned for level walking; however, tuning adjustments are a normal part of the clinical process and occurred during the study, and therefore tuning parameters between the level and inclined walking data collections may have differed slightly. Another limitation is that mechanical work during single-limb support and transitions from the intact to prosthetic limb both affect V̇O2, but only the transitions from the prosthetic limb to the intact limb were considered in this study. Finally, the calculations performed in this study emphasized double support as the entire period of step-to-step transitions. However, Adamczyk and Kuo 34 presented data supporting that the redirection of COM velocity occurs just before and ends just after the period of double support. Future work could compare step-to-step transitions during the period of COM velocity redirection in an amputee population.
Conclusion
In conclusion, the powered BiOM prosthesis increased ankle power and trailing limb push-off work during step-to-step transitions on both level ground and inclines. The improvement in trailing limb push-off may partly account for the reduction in metabolic rate over level ground, but it had little effect on reducing the energy lost during step-to-step transitions. On inclines, the ESR trailing limb did not display deficiencies in push-off work relative to able-bodied individuals; the slightly lower values still resulted in leading limb compensations and net energy dissipation. Although leading and trailing limb mechanical work during step-to-step transitions do not account for total metabolic demand, they do contribute substantially to a portion of it. The powered BiOM ankle–foot prosthesis reduced metabolic rate on level ground but not on inclines, but resulting values were equivalent to able-bodied individuals. Overall, there were limited negative biomechanical or metabolic consequences to wearing a powered ankle–foot prosthesis. The results of this study may be used to guide the development and use of actively powered prosthetic devices in high-functioning individuals. Future work may examine how different inclines and velocities affect V̇O2 and individual limb work in individuals with amputations who are using new prosthetic technology.
Footnotes
Author contribution
The study concept and design was contributed by E Russell Esposito and JM Wilken. Acquisition of data was done by JM Whitehead. Analysis and interpretation of data were carried out by E Russell Esposito. Statistical analysis was performed by JM Whitehead. Drafting of the article was done by E Russell Esposito. Critical revision of the article for intellectual content was carried out by E Russell Esposito, JM Whitehead, and JM Wilken. Funding was obtained by JM Wilken.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
Support was provided by the Center for Rehabilitation Sciences Research (CRSR), Department of Physical Medicine and Rehabilitation, Uniformed Services University of Health Sciences, Bethesda, MD, and US Army Telemedicine & Advanced Technology Research Center (TATRC).