
Abstract
Background:
Functional hallux limitus (FHL) has been implicated in the development of metatarsophalangeal joint osteoarthritis.
Objectives:
To determine whether cut-out orthosis treatment increases plantarflexion of the first metatarsal by increasing its declination angle.
Study design:
Cross-sectional study.
Methods:
A total of 46 female volunteers with an average age of 25.66 ± 5.70 years (range: 19–42 years) and FHL participated in the study. We assessed the degrees of movement of the first metatarsal and proximal phalanx bones at the first metatarsophalangeal joint without and while wearing the cut-out orthosis using the 3Space Fastrak® via sensors.
Results:
The movement of the plantarflexión declination angle of the first metatarsal bone was higher using the orthosis 29.84° ± 5.98° versus without orthosis 27.69° ± 5.91° (p < 0.031°). Use of sandals may have minimized the magnitude of movement changes associated with orthosis versus non-orthosis use.
Conclusion:
The cut-out orthosis demonstrated a beneficial effect on non-fixed first metatarsophalangeal and metatarsal cuneiform joints affected by FHL, significantly increasing the declination of the metatarsal angle. Furthermore, use of the cut-out orthosis significantly reduced adduction movement of the first metatarsal bone in the transverse plane.
Clinical relevance
The cut-out orthosis demonstrated a beneficial effect on non-fixed first metatarsophalangeal and metatarsal cuneiform joints affected by FHL, significantly increasing the declination of the metatarsal angle. Furthermore, use of the cut-out orthosis significantly reduced adduction movement of the first metatarsal bone in the transverse plane.
Background
Movement of the first metatarsophalangeal (MTP) joint in the sagittal plane is an essential component of normal function of the human foot during gait. Dorsiflexion at this joint during gait is mandated by heel off. Functional impairment of the MTP joint occurs when there is a reduced range of motion during walking in a joint that has no structural limitations. This presentation is referred to as functional hallux limitus (FHL). 1 FHL has been described as the inability of the first MTP joint to dorsiflex sufficiently during gait when normal motion is present on nonweight-bearing examination 1 and has been implicated in the development of MTP joint osteoarthritis. 2 The hallux must continue to dorsiflex to accommodate the concomitant heel off. Forced dorsiflexion of the hallux during continued heel off, in the presence of FHL, produces abnormal and pathologic forces within the first MTPjoint.
Although numerous causes have been attributed to contributing to this malady, we contend that a pathomechanical event occurs with abnormal dorsiflexion of the first ray that limits first MTP joint motion, when full range of motion is available. This concept is not new, as the dorsiflexion position of the first metatarsal bone has been inferred to affect the motion of the first MTP joint.3,4 Excessive dorsiflexion of the first metatarsal bone performed in a repetitive manner may cause degenerative joint disease at the first MTP joint. The patient may complain of pain during push off which is usually due to localized tenderness, swelling, and decreased dorsiflexion of the involved toe. Plain radiographs demonstrate narrowing of the MTP joint and subchondral sclerosis. Treatment is geared toward symptomatic management and may include icing and taping the toe. Surgical treatment includes debridement of the MTP joint and, occasionally, arthrodesis of the MTP joint in 15°–20° of dorsiflexion.5,6
Both custom and prefabricated orthoses have been reported to increase hallux dorsiflexion, as determined by a reduction in symptoms in 30 patients with hallux limitus. 7 However, neither the customized nor the prefabricated orthoses produced a significant change in symptoms. Another study identified first MTP joint dorsiflexion as a distinct pronation-sensitive attribute of the weight-bearing foot. 8 The authors applied a low-dye strap to determine whether limiting pronation in stance increased the range of dorsiflexion and found that anti-pronation strapping increased the range of dorsiflexion of the first MTP joint.
The literature is lacking studies that measure the movement of the first metatarsal bone and hallux in the three planes of motion: dorsiflexion/plantarflexion, adduction/abduction, and inversion/eversion, with and without wearing a cut-out functional orthosis. The purpose of this study was to examine the effect of the cut-out orthosis design on the kinematic behavior of the hallux and first metatarsal bone in these three planes at the push-off period of gait in individuals with FHL.
We hypothesized that wearing the cut-out functional foot orthosis would result in greater hallux and first metatarsal bone joint motion in the three planes under load conditions from midstance to the push-off phase of gait. By increasing plantarflexion of the first metatarsal bone, we further hypothesized that use of this orthosis would help relieve symptoms related to FHL.
Methods
Subjects
The Institutional Review Board at Rey Juan Carlos University approved the study. All subjects gave their written informed consent prior to participation in the study.
Participants for this cross-sectional study were recruited from the same school of professional female tennis players over a 1-year period (January 2012 to January 2013). Out of 146 subjects who initially volunteered to participate in the study, 85 subjects did not meet the inclusion criteria, and an additional 15 subjects did not return to the study for unknown reasons, leaving 46 female subjects to participate in the study. The average age of the participants was 25.66 ± 5.70 years (range: 19–42 years), with an average weight of 66.86 ± 8.82 kg (range: 56–83 kg) and an average height of 165.52 ± 9.33 cm (range: 150–181 cm).
All subjects were required to meet the following inclusion criteria: (1) no history of trauma to the foot; (2) the presence of at least 10° of dorsiflexion at the ankle with the knee fully dorsiflexed; (3) unrestricted motion of the functional subtalar joint of 30°; (4) unrestricted motion along the longitudinal axis of the midtarsal joint of 15°; (5) unrestricted nonweight-bearing motion of the first ray of at least 8 mm; (6) greater than 50° of dorsiflexion of the hallux to the first metatarsal bisection during nonweight-bearing; (7) age greater than 18 years and younger than 60 years; (8) at the time of data collection, no lower limb dysfunction or chronic injury; and (9) no evidence of a non-fixed deformity at first MTP and first metatarsal cuneiform joints.
Participants were excluded if they had established hallux valgus, a previous history of foot and ankle trauma, fracture, surgery, or an existing diagnosis of inflammatory, metabolic, neurological, or vascular disease. Individuals were also excluded from the study if they exhibited less than 40° of available first MTP joint dorsiflexion (as measured using a nonweight-bearing technique previously described by Buell et al. 9 This has been reported to be the range of first MTP joint dorsiflexion used during normal propulsion10 –12 and would, therefore, have indicated structural limitation at the joint. In addition, no subject had a history of congenital deformity, pain, or traumatic injury involving either of their lower extremities during the 6 months prior to study enrollment.
Assessment of functional hallux limitus
All participants underwent a clinical examination of passive hallux dorsiflexion to compare the range of available dorsiflexion upon weight-bearing and nonweight-bearing.
For each participant, the range of motion of the hallux was tested with the foot in plantarflexion to rule out the presence of hallux rigidus. Assessment of FHL has been described both for weight-bearing and nonweight-bearing situations.13,14
Dorsal mobility of the first MTP joint was measured with the subject nonweight-bearing and lying prone. Using a classic goniometer with the legs aligned along the longitudinal axis of the hallux and the first metatarsal bone, first MTP joint range of dorsal motion was calculated as the angular difference between the position with the hallux aligned with the first metatarsal bone and the position at maximal dorsiflexion (Figure 1). The latter was measured with the hallux dorsiflexed until firm resistance was sensed, while the first metatarsal bone was fixed manually and the subtalar joint was left in a relaxed position. This measurement accorded well with the definition of assisted hallux dorsiflexion as described by Buell et al.; 9 because reference values for assisted dorsiflexion of the hallux range from 65° to 90°, it was difficult to reach a consensus concerning the degree of limitation in first MTP joint dorsiflexion that should be considered hallux limitus. In this study, the value of 70° was chosen as an acceptable hallux limitus separator, as proposed by Van Gheluwe et al. 15
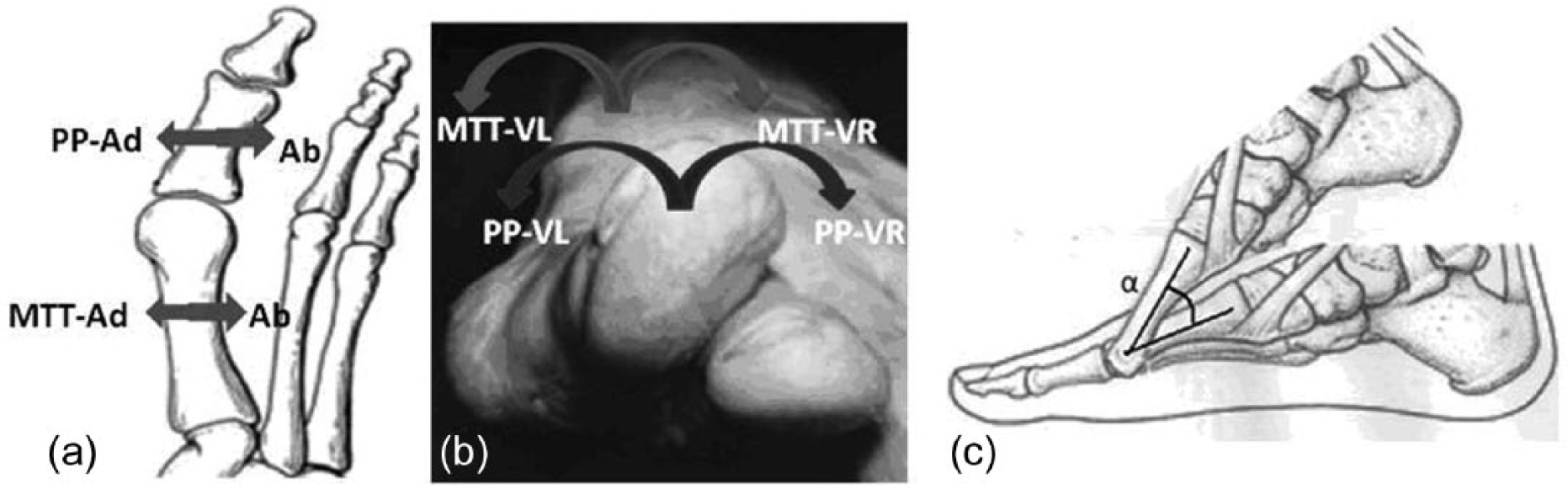
Local anatomical movements are measured according to coordinate systems for the proximal phalanx of the Hallux (PP) and first metatarsal (MTT) bone segments. (a) PP and MTT in Adduction (Ad) and Abduction (Ab). (b) PP and MTT valgus (VL) and varus (VR). (c) Metatarsal declination angle, α, is the angle measured from midstance to push off, indicating the angle subtended by inclination of the metatarsal bone calibrated to 0° and the angle obtained during the push-off phase of gait.
Musculoskeletal assessment was performed in subjects who demonstrated clinical FHL in stance phase. FHL was defined as the presence of passive hallux dorsiflexion in quiet stance phase <40°, despite a nonweight-bearing range of motion >50°; the cutoffs were based upon the normative data of Nawoczenski et al. 16 Weight-bearing examinations were taken with the subjects standing in a relaxed double-limb support with knees fully extended, and with the foot in its relaxed position. Nonweight-bearing examinations were taken with the subject sitting, knee and ankle flexed to 90°, and the heel aligned to the long axis of the shank. A clinician passively dorsiflexed the hallux by pushing up on the proximal phalangeal until a maximum dorsiflexion was reached.
Where subjects reported bilateral FHL, the joint which gave the most motion restriction was selected for the purposes of the study. Participants were screened using the above two methods of assessment to ensure that all subjects met the criteria for FHL by the same clinician (R.S.G.) who has 10 years of experience in the field of podiatry.
The degrees of movement (Figure 2) of the first metatarsal bone, dorsiflexion/plantarflexion, adduction/abduction, and inversion/eversion at the first metatarsal cuneiform, and the degrees of movement of the first proximal phalanx bone, and dorsiflexion/plantarflexion, adduction/abduction, and inversion/eversion at the first MTP joint, without and while wearing the cut-out functional orthosis, were studied.
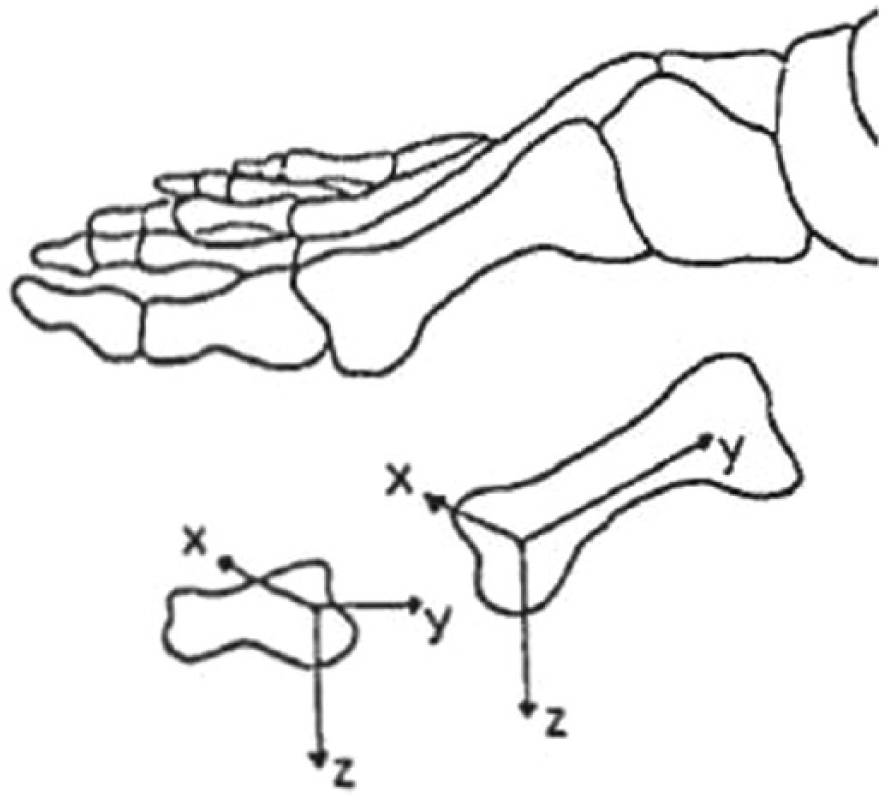
Illustration showing the local anatomical coordinate systems for the hallux and first metatarsal segments. The positive x-axis is directed laterally, the positive y-axis is directed posteriorly, within the long axis of the hallux and metatarsal segments, and the positive z-axis is directed inferiorly. Dorsiflexion rotation of the hallux with respect to the first metatarsal head is described about the x-axis.
Measurements
All measurements were made using the 3Space Fastrak® (Polhemus, Inc., Colchester, VT, USA), which had a sampling rate of 120 Hz. A transmitter, containing three orthogonal coils, created a magnetic field, and the position of a sensor (also containing three coils) was monitored as it moved within the magnetic field. Measurements of sensor position were made relative to the transmitter, with 6 degrees of freedom. The system had a static accuracy of 0.8 mm for sensor position and 0.15° for sensor orientation. The range (transmitter/sensor separation) was 0.76 m at the stated accuracy and up to 3.05 m with a reduced accuracy. The resolution was 0.5 mm/m of transmitter/sensor separation for position and 0.025° for orientation.
Recordings can be affected by metallic objects close to the transmitter. To minimize such effects, large metallic objects were kept over 1 m away from the transmitter, and subjects were positioned to minimize the distance between the transmitter and sensor. No interference from metallic objects in the vicinity was noted, however, during calibration tests.17 –20
Movement of the hallux at the first MTP joint and movement of the first metatarsal bone at first metatarsal cuneiform joint of each individual’s right extremity were measured using the 6D research electromagnetic motion analysis system (Skill Technologies Inc., Phoenix, AZ, USA). This system was based on the Fastrak tracking device and used an electromagnetic transmitter with up to four electromagnetic sensors. The signals from each sensor were input into a digital signal processor that computed the sensor’s position and orientation relative to a transmitter.
For this study, the electromagnetic transmitter was positioned at a height of 96 cm, at the midway point of a 6-m raised walkway. The walkway did not have metal reinforcement to avoid any possible distortion of the electromagnetic fields caused by metal reinforcement in the laboratory’s floor. Two electromagnetic sensors were used to collect the angular position data of the hallux and first metatarsal bone during push-off phase of walking. The sampling rate for each sensor was 60 Hz.
Procedure
Two electromagnetic sensors were attached to one lower extremity of each individual using double-sided adhesive tape (Figure 3). One sensor was placed along the medial aspect of the proximal phalanx of the hallux, the second sensor was placed at the medial aspect of the head of the first metatarsal bone, and both were attached with double-sided tape, and secured with Hypafix™ tape over the sensors. The anatomical sites chosen had minimal overlying soft tissue to reduce possible sensor movement during walking in accordance with a protocol devised by Welsh et al. 21

Photograph showing the location of motion receivers over the proximal phalanx of the hallux and first metatarsal head.
Excursion of extensor hallucis longus tendon has been previously described as a significant source of error when mounting a sensor over the dorsum of the hallux. 20 This source of error was minimized by securing the sensor with a Velcro strap that encircled the toe according to a recently described protocol modification. 22 All cables were secured with straps to the limb and waist with a belt. The 6D Research™ software package was used to process the data from the sensors, as described previously. The signal produced by each switch was recorded and synchronized with the kinematic data.
For calibration, subjects stood near the center of the electromagnetic field, with the calcaneus vertical and talar head equally palpable on both medial and lateral sides to establish a reference position.21,23 The sensors were connected to a microcomputer for data collection by means of a 30-foot serial cable. The individual’s right lower extremity was then positioned so that the calcaneus and the lower leg were perpendicular to the supporting surface at the normal angle of gait. While in this position, each sensor’s orientation was initialized relative to the laboratory reference frame. This position was used as the “zero” reference point for all angular measurements. After initializing the sensors in a barefoot anatomical position, each participant walked along the walkway in the same direction at a self-selected speed, before entering the 1.5-m calibrated capture volume and continued walking for an additional 1.5 m. Five trials were completed for each of the experimental conditions: “orthoses” and “no orthoses.” The order of data collection was randomized. Care was taken when inserting the foot orthoses into, and removing them from, the boots so that the sensors were not disturbed or displaced. This was enabled by the Hypafix fastening. During the study, motion of the first MTP during the second step was used to acquire motion data of the proximal phalanx of the hallux and first metatarsal bone during gait. 24
The mean of the five trials was used in subsequent analyses. A Cardan system of three orders of rotations (X-Y-Z) was used to extract angular and linear information of the hallux and first metatarsal. Movement about the mediolateral axis (X) was defined as dorsiflexion and plantarflexion. Movement about an anteroposterior axis (Y) was defined as inversion/eversion. Movement about a craniocaudal axis (Z) was defined as abduction and adduction. The anatomical landmarks and coordinate systems have been previously described.10,16 Hallux and first metatarsal movements were assessed with respect to the laboratory coordinate system. 25
For each subject, we fabricated a pair of rigid functional custom foot orthoses devoid of an arch in order to avoid any restriction to the movement of the first metatarsal cuneiform joint. This was accomplished from a negative cast of the foot using a Root-method-neutral-position nonweight-bearing cast 26 with the first metatarsal intentionally plantarflexed by dorsiflexion of the first MTP joint to create a cut-out under the head of the first metatarsal bone. This functional foot orthosis permitted plantarflexion of the first ray at the first metatarsal cuneiform joint. The same clinician (R.S.G.) performed all the casting. Each orthosis was made with a shell of 3 mm vacuum-formed polypropylene with minimum filling positive. 27 The forefoot was fabricated with 3 mm hard ethylene vinyl acetate (EVA) (450 kg/m3) with a cut-out under the head of the first metatarsal bone 21 covered with 1 mm of Poron full length cover, with a slot to allow for strap adjustment at the first digital web space.
Subjects were also issued a pair of sandals that were used during the study before and after wearing the orthosis (Figure 4). The sandals had a strap between the first digital web space and the rearfoot that enabled the orthosis to be held onto the foot. Data were analyzed during the push-off period of gait. Midstance of the reference extremity was identified as the midpoint between heel contact and toe off. Push off was defined as the period of gait between heel off and toe off, which was the time when peak dorsiflexion of the first MTP joint and metatarsal declination angle due to plantarflexion at first metatarsal cuneiform joint occurred in the three planes. 11

Sensor placement with sandal shows the position of the EMT sensors attached at the anatomical landmarks used during capture of the kinematic data.
Statistical analysis
After an initial Kolmogorov–Smirnov test, which demonstrated the data were normally distributed, paired Student’s t-tests were performed to determine whether there were significant differences between orthosis with cut-out versus orthosis without cut-out, and an alpha level of 0.01 was established for all tests of significance. Intraclass correlation coefficients (ICCs) 28 and standard error of measurements (SEM) 29 were used to assess the within-day trial reliability of each participant’s push off and stance phase duration.
Using the classification proposed by Landis and Koch, 28 coefficients between 0.20 and 0.40 were considered fairly reliable, scores between 0.40 and 0.60 had moderate reliability, scores between 0.60 and 0.80 had substantial reliability, and the highest category, scores between 0.80 and 1.00 were considered almost perfect. We interpreted a reliability coefficient of 0.90 as a desirable magnitude of reliability based on recommendations that clinical measurements with reliability coefficients exceeding 0.90 enhanced the likelihood that the measurement was also reasonably valid. 30
In addition to ICC values, the SEM was also calculated as another index of reliability. The SEM was also used to calculate the minimal detectable change (MDC) for all measurements, also called Reliable Change Index (RCI). We used the RCI as a statistical method for determining clinical significance, as proposed by Jacobson and Truax. 31
Paired Student’s t-tests were performed to determine differences between the mean of maximum peak range of motion in three axes at the proximal phalanx and first metatarsal bone while wearing versus not wearing the cut-out orthosis. We calculated the MDC proportion (MDCP) as a percentage.
For all analyses, p < 0.05 (within a 95% confidence interval) was considered statistically significant. Data analysis was conducted with SPSS software, version 19.0 (SPSS Science, Chicago, IL, USA).
Results
All data were analyzed to establish the effect of the cut-out orthosis in three axes of movement with the medial line of the body taken as reference movement. Within-day trial-to-trial ICC and SEM values with the subjects wearing the orthosis versus not wearing the orthosis in each plane of motion for hallux and first metatarsal bone are shown in Table 1. All variables measured for this study had a value coefficient between 0.931 and 1.00. All variables were found to exhibit this level of between-trial reliability. Using this criterion, all 24 variable measurements were considered reliable.
Within-day trial-to-trial reliability as measured by ICC and SEM for peak hallux and first metatarsal bone plane movement at the push-off period of gait.
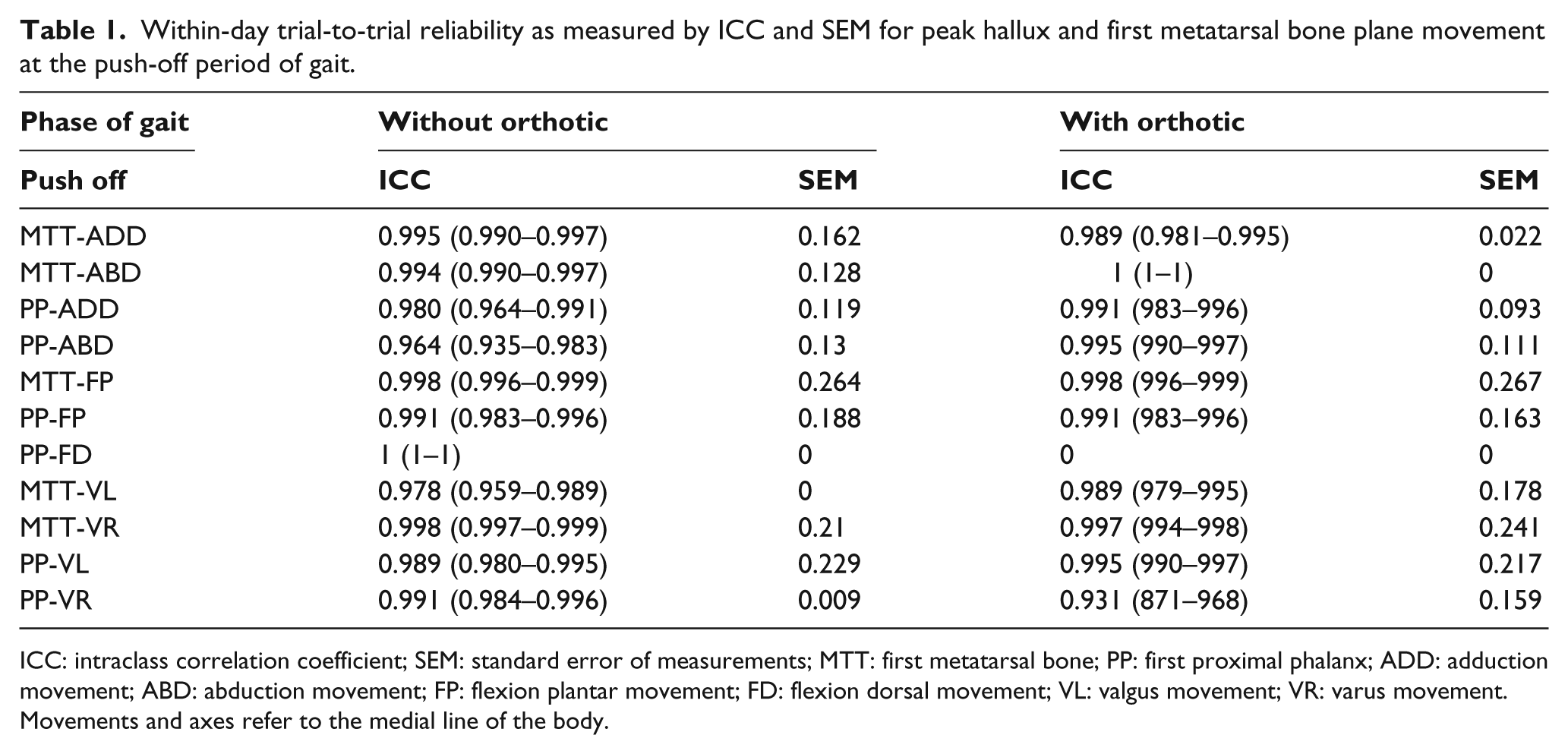
ICC: intraclass correlation coefficient; SEM: standard error of measurements; MTT: first metatarsal bone; PP: first proximal phalanx; ADD: adduction movement; ABD: abduction movement; FP: flexion plantar movement; FD: flexion dorsal movement; VL: valgus movement; VR: varus movement.
Movements and axes refer to the medial line of the body.
ICC values for peak range of motion in the three planes ranged from 0.964 to 0.998 when not wearing the orthosis, while ICC values while wearing the cut-out orthosis ranged from 0.931 to 1.00; thus, all the ICC values were valid measurements. 30 The ICCs indicate a high degree of within-subject consistency at both proximal phalanx and first metatarsal bones, at their joint complexes (first MTP joint and first cuneiform metatarsal joint), during the push-off phase of gait (Table 1).
The results of the movement in the three planes for the hallux at the first MTP joint and for the first metatarsal bone at the first metatarsal cuneiform joint in each plane of motion are shown in Table 2. The lower movement of the first metatarsal bone in adduction in the transverse plane was significant and measured 2.61° ± 2.29° without orthosis compared with 0.31° ± 0.21° measured with orthosis (p = 0.001). Also, the declination angle (on plantarflexion) of the first metatarsal bone was significantly higher using the orthosis (29.84° ± 5.98°) relative without it (27.69° ± 5.91°) (p = 0.031). The abduction and the valgus, varus, and dorsiflexion movements of the metatarsal bone and all the movements at the hallux did not show any differences (p > 0.05).
Movements in the axis between the “without cut-out” and “with cut-out” population.
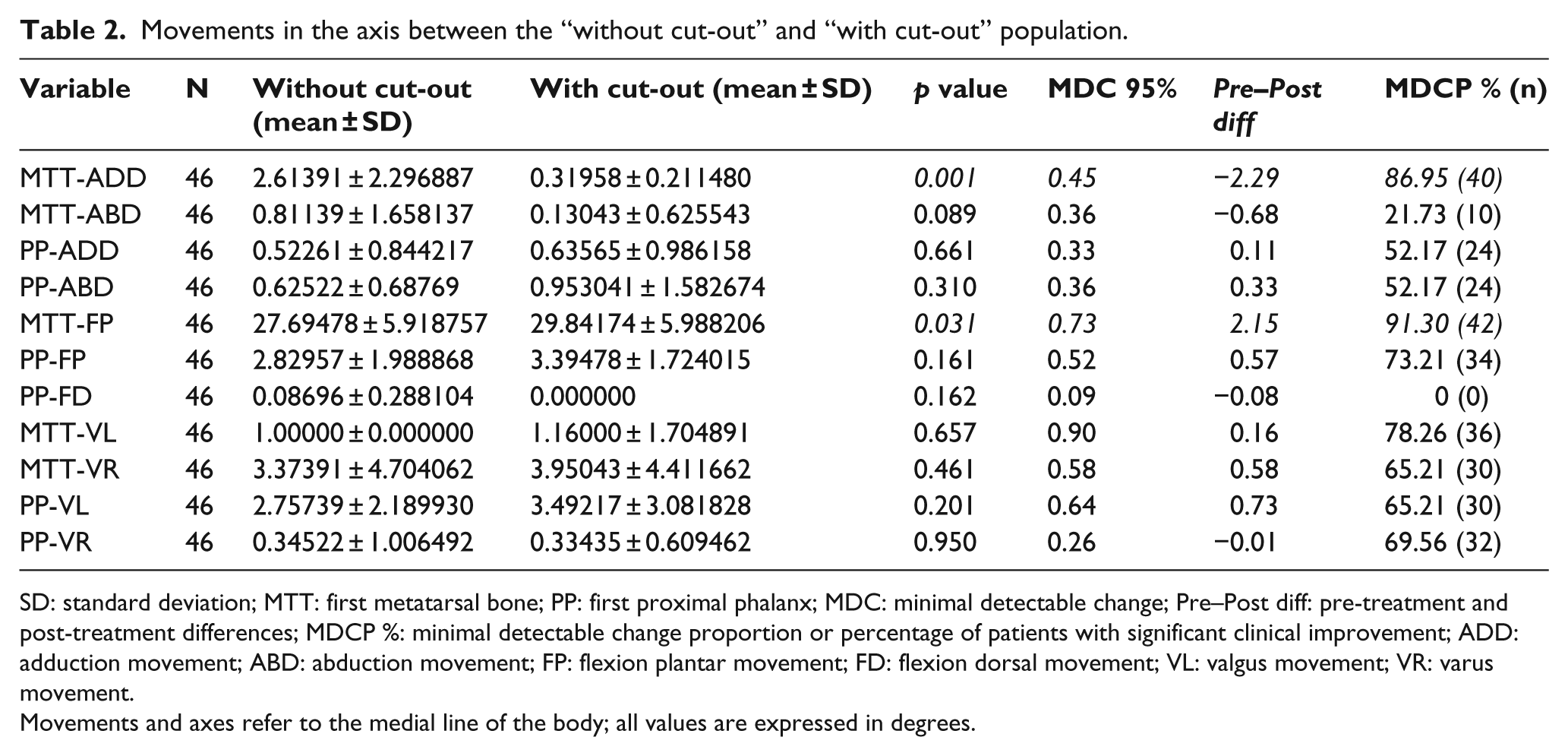
SD: standard deviation; MTT: first metatarsal bone; PP: first proximal phalanx; MDC: minimal detectable change; Pre–Post diff: pre-treatment and post-treatment differences; MDCP %: minimal detectable change proportion or percentage of patients with significant clinical improvement; ADD: adduction movement; ABD: abduction movement; FP: flexion plantar movement; FD: flexion dorsal movement; VL: valgus movement; VR: varus movement.
Movements and axes refer to the medial line of the body; all values are expressed in degrees.
The inter-rater MDC 95% values (Table 2) ranged from 0.90° to 0.09°. The first metatarsal bone adduction movement (MTT-ADD) showed a significant difference when comparing “with” versus “without” orthosis (p = 0.001) with a MDC 95% of 0.45° (Table 2). The plantarflexion of the first metatarsal bone (MTT-FP) also showed a significant difference (p = 0.031) with a MDC 95% of 0.73° (Table 2). The MDCP values (which demonstrate that the percentage of patients with significant clinical improvement for each variable studied) are also shown in Table 2 for the MTT-ADD and MTT-FP.
Discussion
The aim of this study was to explore whether a cut-out orthosis treatment could increase plantarflexion of the first metatarsal bone by increasing the declination angle of the first metatarsal. The cut-out orthosis modification used in this study was based on the work by Dananberg 32 who first recommended a modification in the midsole of an orthosis for patients with hallux limitus. We found that the declination angle of the first metatarsal with the orthosis was significantly greater than without the orthosis. We also detected a significant difference between “with” versus “without” orthosis for the plantarflexion of the first metatarsal bone. Surprisingly, we found that the adduction displacement of the first metatarsal bone is significantly lower when wearing the cut-out orthosis, allowing for the quantification of the plantarflexion of the first metatarsal bone, a detail that has not been described previously in the literature.
During the stance to push-off phase of gait, first MTP flexion is a requisite for unrestricted first MTP joint dorsiflexion to occur. 33 This angle of declination reflects the dorsiflexion at the first MTP joint, such that an increase in the metatarsal declination angle corresponds to an elevation of the medial longitudinal arch.33 –35 In addition, an increase in this angle places the first metatarsal in a position of plantarflexion, which is considered favorable for the propulsive phase of gait.36,37 Thus, creating a cut-out under the head of the metatarsal bone would permit a higher plantarflexion of the metatarsal bone due to the pull of the peroneus longus muscle, increasing the declination angle of metatarsal and keeping the hallux in contact with the floor due to the load, thereby increasing the dorsiflexion of the first MTP joint and reducing pain at the joint.
In contrast to our findings, Welsh et al. 21 found that a reduction in joint pain at the first MTP joint following orthosis intervention was not accompanied by a change in first MTP joint dorsiflexion. They determined that the maximum dorsiflexion values obtained at the first MTP joint had a median value of 8.34°, demonstrating a large kinematic variability in both the no-orthoses versus orthoses conditions. Other authors, using similar electromagnetic track (EMT) systems to measure first MTP joint motion, reported angles of 37°, 12 42°, 10 and 38°–40°. 11
Nawoczenski and Ludewig 11 measured the peak dorsiflexion of the first MTP joint in 18 subjects using two orthosis designs. One design incorporated an extrinsic rearfoot and forefoot post, and the second design had a medial longitudinal arch in combination with an extrinsic rearfoot post. An electromagnetic tracking device was used to collect three-dimensional positions of the hallux and first metatarsal. They found that the dorsiflexion at the MTP joint averaged between 38° and 40° across all conditions, but the first metatarsal declination in subjects not wearing orthosis was 20.4° versus 23.6° and 23.5°, respectively, for those wearing forefoot post and arch orthosis.
We measured the movement, in the three planes, of both the proximal phalanx of the hallux and the first metatarsal bone because movement of the first metatarsal bone depends on two joints: the first metatarsal cuneiform joint and the first MTP joint. Thus, we felt it was more appropriate to measure first metatarsal movement instead of measuring the range of motion at the first MTP joint, alone. Based on our results, when using the EMT system, we propose measurement of the degree of movement of each bone separately; in this case, proximal phalanx and first metatarsal bone, instead of a joint motion formed by the combined movement of two bones at the joint. Studies are lacking that measure the plantarflexion of the first ray at the first cuneiform joint, and further research in this aspect is needed.
Another important finding involved significantly less adduction displacement when using the cut-out orthosis in the transverse plane of the metatarsal bone (p < 0.001). This may aid those afflicted with hallux valgus deformity since increased adduction of the first metatarsal bone is the main deformity causing increased separation between the first and second metatarsal bones, thereby increasing the intermetatarsal angle. 38 Scherer et al. 27 stated that the orthosis made from a negative cast with the first ray plantarflexed and a 4-mm medial skive could increase the maximum degree of dorsiflexion in patients with limited dorsiflexion in stance and gait. Thus, a cut-out orthosis that increases the range of dorsiflexion at the first MTP joint, by increasing the declination of the first metatarsal, might contributeto a reduction in symptoms caused by this deformity. Furthermore, functional activities (e.g. running, stair-climbing, squatting) may require additional movement of the first ray in plantarflexion and less movement in adduction to better stabilize the first metatarsal bone as shown in Table 2. The relationship between these two movements has not been fully established, highlighting the importance of our study.
Limitations to our study include the fact that the results reported are specific to the orthosis device tested, and therefore, it is not known whether the results obtained would have been different for a device manufactured by a different method, and/or from different materials. Future research should extend the scope of the study by investigating a variety of manufacturing and prescription methods commonly employed. In addition, although enabling direct access of the sensors to skin overlying the bony segments of the hallux and metatarsal bones,39,40 the use of sandals may have minimized the magnitude of motion changes associated with both non-orthosis and orthosis use.
Conclusion
The cut-out orthosis demonstrated a beneficial functional effect within non-fixed first MTP and metatarsal cuneiform joints in FHL, significantly increasing the declination of the metatarsal angle. Also, the use of cut-out orthosis significantly reduced the adduction movement of the first metatarsal bone in the transverse plane.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.