
Abstract
Background:
Studies have not been conducted to investigate the influence of the height of the rotational axis of a wheelchair’s back support on the shear force applied to the buttocks during the reclining motion.
Objectives:
The purpose of this study was to investigate the influence of the difference in the rotational axis position of back support in the vertical direction on the horizontal force applied to buttocks for preventing decubitus ulcers.
Study design:
Repeated measures design.
Methods:
The subjects were 13 healthy adult men without leg and/or trunk diseases. The shear force was measured using a force plate. A comfortable sitting posture in the experimental chair was selected for measurement. The rotational axis was positioned 13 cm forward on the horizontal plane from the intersection between the seat and the back support. The axis positions on the vertical plane as two experimental conditions were the seat height and the 7.5-cm upward from the seat height which was nearer to the hip joint.
Results:
In returning the back support to an upright position, the horizontal force was 12.4 ± 1.6 (percent body weight) under the seat height-axis condition and 10.1 ± 1.8 (percent body weight) under the upward-axis condition (p < 0.01).
Conclusion:
This result suggested that the wheelchair might have to be capable of adjusting the height of the rotational axis of the back support to reduce the horizontal force applied to buttocks.
Clinical relevance
This study shows one of the suggestions regarding seating approach for the prevention of decubitus ulcers. There is a possibility of reducing horizontal force applied to buttocks after reclined back support, by adjusting the height of the rotational axis position of wheelchair back support.
Background
The causes of decubitus ulcers are a mixture of internal and external factors. Several combinations of factors, including external pressure and shear force, temperature, humidity, hygiene, nutrition, deterioration in sensory and motor function, and posture may contribute to the formation of these ulcerations. 1 The National Pressure Ulcer Advisory Panel (NPUAP) 2 defined a decubitus ulcer as a localized injury to the skin and/or underlying tissue usually over a bony prominence because of pressure or pressure in combination with shear. Additionally, there are four known mechanisms contributing to decubitus ulcer formation: ischemia, lymphatic compromise, reperfusion injury, and sustained deformation under high loads.
Reclining wheelchairs are commonly used to transport persons who cannot sit in a conventional wheelchair. Many such individuals require reclining back support and cannot independently correct incidents of postural collapse, in which the angle between the trunk and the hip increases because the buttocks slide forward; thus, many tend to shift downward in their chairs. From these observations, we postulated that there is greater shear force applied to the buttocks of these wheelchair-bound individuals when their posture collapses 3 and that this may lead to an increased incidence of decubitus ulcers.
Regarding the shear force, in the 1970s, Guttmann 4 attributed a larger role to shear force than pressure in reducing the vascular supply. In addition, Bennett et al. 5 reported that a combination of pressure and shear force effectively promote blood flow occlusion. The effects of various pressures on blood flow and ulceration, with and without shear, in normal and paraplegic swine showed that in animals subjected to pressure and shear force, ulceration occurred at lower pressures than in those animals experiencing only pressure. 6 Although any load varies depending on the individual and his or her body location, further investigations suggested that 50 mmHg of pressure and 9 kPa of shear force were nearly equivalent for their effects on biological soft tissue. 7 Goossens et al. 8 also reported that a shear force of 3.1 kPa significantly reduced blood flow in the sacrum of healthy subjects and pointed to the importance of reducing shear force for preventing decubitus ulcers. Thus, shear force as a factor contributing to the development of decubitus ulcers has attracted attention since the 1970s.
Relatively recent reports, investigating the etiology of decubitus ulcers, have suggested that ischemia, alone, cannot explain the etiology of deep tissue injuries in decubitus ulcers and that other mechanisms, particularly excessive cellular deformation, are likely involved.9–12 Linder-Ganz et al. 9 reported that the skeletal myocytes of rats can survive 2 h of complete ischemia but die within 15 min of a load causing shear deformation. Other authors 10 who conducted rat studies that isolated the effects of ischemia and shear loading found that 2 h of ischemic conditions caused by a tourniquet resulted in reversible tissue changes, whereas 2 h of static loading by an indenter induced irreversible damage. The areas damaged corresponded to the region undergoing high shear strain, as determined in separate experiments. Thus, animal studies involving static loading and finite-element modeling have suggested that the shear deformation of tissue initiates short-term tissue damage. After the initiation of damage, ischemia may accelerate injury due to hypoxia, glucose depletion, and acidification.11,12 Conversely, Lahmann and Kottner 13 reported that there is a strong relationship between friction forces and superficial skin lesions and between pressure forces and deep tissue injury. In addition, a systematic review by Reenalda et al. 14 revealed “a weak qualitative relation” between interfacial pressure and the development of decubitus ulcers. In fact, the study concluded that “the predictive or prognostic value of interface pressure cannot be quantified.” Ohura et al. 15 reported that shear force combined with a small amount of pressure is a major factor in the development of Stage II decubitus ulcers, but its role in Stage III and IV ulcers is less certain. Regardless, there may be a strong relationship between shear force and the formation of decubitus ulcers.
Gilsdorf et al. 16 studied the effect of the angle of back support on the shear and normal forces applied to the buttocks. They found that a shear force was applied to the buttocks in the posterior direction when the back support was reclined and in the anterior direction when it was returned to the upright position. Hobson 17 reported that a back support recline angle of 30° caused a 25% increase in the surface shear force applied to the buttocks as compared with a recline angle of 10° in subjects with spinal cord injuries. Bennett et al. 18 compared the shear and normal forces applied to the buttocks of normal, hospitalized geriatric and paraplegic subjects and showed that the normal force did not differ significantly among the three groups. However, the shear forces applied in seated, hospitalized geriatric and paraplegic individuals were roughly three times those in normal subjects, and the rate of pulsatile skin blood flow volumes applied to the buttocks in seated paraplegic individuals while roughly equal to those of hospitalized geriatric subjects was only one-third of those in comparable normal subjects. Furthermore, in a previous study, we investigated the mechanism of shear force fluctuations applied to the buttocks while a wheelchair’s back support was reclined. 19 The results suggested that shear force applied to buttocks is greatest as the positions of the axes of rotation for the back support and for the trunk–pelvis are separated. In another study, the results suggested that the rotational axis of a wheelchair back support might need to be closer to the hip joint, on the horizontal plane, to reduce the shear force applied to the buttocks when a patient is returned to an upright position. 20 However, the height of the rotational axis position did not need to be moved closer to the hip joint. Studies have not been conducted to investigate the influence of the height of the rotational axis of a wheelchair’s back support on the shear force applied to the buttocks during the reclining motion.
The purpose of this study was, therefore, to investigate the influence of the rotational axis height on the shear force applied to the buttocks, with the goal of preventing decubitus ulcer formation in individuals using wheelchairs with a reclining back support. We hypothesized that the shear force applied to the buttocks would be reduced by reducing the rotational axis of the hip joint on the vertical plane.
Methods
Participants
The participants included 13 healthy, adult men without leg and/or trunk disease (mean age, 22.6 ± 4.2 years; height, 171.7 ± 5.0 cm; and body weight, 68.3 ± 9.8 kg). Participants were excluded from the study if they experienced pain while sitting on a chair, experienced back pain, had undergone surgery, or had rheumatism or neurologic disorders. The study was conducted with the approval of the Research Ethics Committee at Kawasaki University of Medical Welfare (#074), and informed consent was obtained from all participants.
Measurement of the forces applied to the buttocks and back support
The NPUAP 21 defined shear as “an action or stress resulting from applied forces which causes or tends to cause two contiguous internal parts of the body to deform in the transverse plane.” NPUAP said, therefore, that the shear force is difficult to measure. Thus, in this study, we measured the horizontal and normal forces in substitution of the shear force. The horizontal and normal forces applied to the buttocks were measured using a force plate (Kyowa Electronic Instruments, Tokyo, Japan). The force plate measured the reaction force in the posterior direction, which is equivalent to the horizontal force in the anterior direction, with a sampling frequency of 100 Hz. A Predia pressure and shear force sensor (Molten, Hiroshima, Japan) was also used in conjunction with a data logger (Omron, Kyoto, Japan) to measure the timing of the force applied to the chair’s back support. This sensor, made of plastic and having an elliptical shape, uses air displacement to measure pressure and a strain gauge to measure shear force. The Predia sensor, 28.14 cm 2 in size, can measure pressures ranging from 0 to 200 mmHg and shear forces ranging from 0 to 50 N. 22 In previous studies, such a sensor was adhered to a flat, rigid surface, and different wound dressings were evaluated by applying a horizontal displacement across the static sensor.23,24 The results of these previous studies suggested that the Predia sensor could perform measurements, with a high degree of confidence, under similar surface conditions. However, because the form and measured surface conditions of the back support material differed from those used in previous studies, only the fluctuation patterns of the forces applied to the back support were considered in this study.
The sensor was attached to the participant’s back at the point of highest pressure caused by the back support when comfortably seated in the experimental chair. The location of highest pressure was manually determined by the examiner. This point was near the longissimus thoracis on the left side and near the seventh or eighth thoracic spinous process; the position was similar for each participant. The measured shear force was positive for a force directed downward from the trunk to the back support and negative for an upward force.
We used an experimental chair with electric controls for reclining the back support (Hashimoto Artificial Limb Manufacturer, Okayama, Japan) (Figure 1). The dimensions of the experimental chair were back support height, 97 cm; depth of seat, 40 cm; backward angle of seat, 0°; reclining angle of back support, 10°–40°; and angular velocity at which the back support reclined, 3°/s. The chair’s back support was covered with artificial leather. By inserting L-shaped pieces at the junction between the back support and the seat frame, the position of the rotational axis of the back support could be adjusted without changing the relative positions of the back support and the seat frame. For measurements, the subjects were made to sit comfortably with bilateral symmetry and were made to rest on the back support and the force plate. In addition, to achieve constant friction between the clothing and the surfaces of the seat, all subjects wore clothing made of 100% cotton. As the smooth metal surface of the force plate was conducive to the participant sliding forward in the chair, a rubber net was laid over the plate to minimize sliding and the risk of postural collapse. The coefficients of friction were 0.9 between the clothing and the rubber net, 0.8 between the rubber net and the surface of the force plate, and 0.4 between the surface of the back support and the clothing. These coefficients of friction were calculated based on the maximum static friction force measured using a pull tension gauge and a weight. To reduce the effects of differences in the positions of the lower extremities, the horizontal thigh angle was adjusted by elevating the feet with wooden boards stacked under the experimental chair, 25 and the foot position was adjusted so that the lower legs were perpendicular to the feet. 26 Furthermore, to reduce the resistance of the lower extremities, a roller board was placed under subjects’ feet. Participants were instructed to fold their arms in front of their chest in a relaxed state and not to intentionally change their body position during the experiment. Each participant’s buttocks were positioned so that the distance from the back support to the dorsal surface of the sacrum in the measurement posture was 3 cm3.
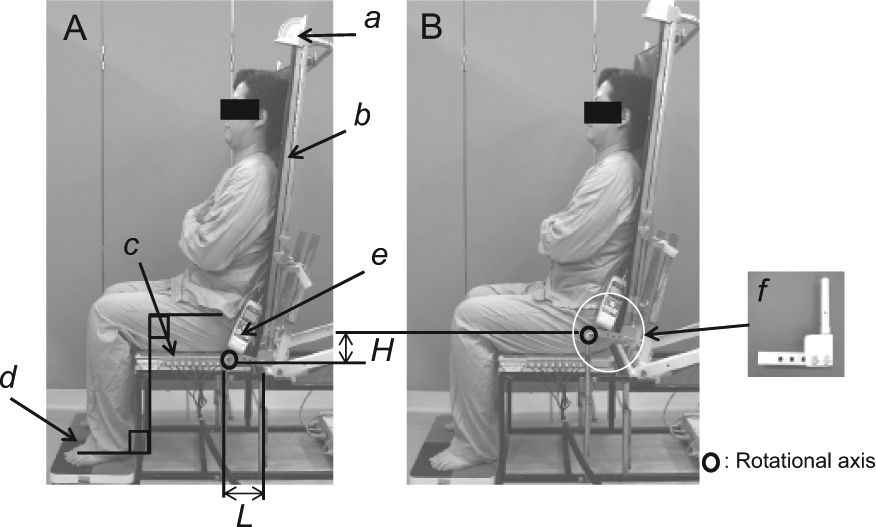
Measured posture and experimental conditions: (A) the seat height-axis and (B) the 9-cm upward-axis. (a) Level goniometer, (b) experimental chair (height of back support: 97 or 106 cm, depth of seat: 40 cm, backward angle of seat: 0°, reclining angle of back support: 10°–40°, and angular velocity at which back support reclines: 3°/s), (c) force plate, (d) roller board, (e) Predia sensor, and (f) L-shaped pieces.
In this study, two experimental conditions were tested. In the seat height-axis condition, the rotational axis was located at the same height as the seat and 13 cm forward of the point farthest back in the seat, so that the buttocks–trochanterion length, in a seated position, was 12.8 ± 1.1 cm for a young, Japanese adult male. 27 In the upward-axis condition, the rotational axis of the back support was positioned at a point 7.5 cm above the seat height-axis condition so that the height of trochanterion from the seat, in a seated position, was 7.1 ± 7.0 cm in a young, Japanese adult male. 27
We refer to this rotational axis position as the upward-axis condition. To correct for the influence of each subject’s postural collapse while making measurements, the measurements were performed 10 s after the posture was set. The experimental back support was reclined at increasing angles, beginning at the fully upright position of 10° from the vertical (initial upright position (IUP)), proceeding to a fully reclined position (FRP) of 40° from the vertical, and returning to the upright position (RUP). The time required to measure the horizontal force in each phase was 5 s in the IUP, 10 s in the FRP, and 5 s in the RUP. For each condition, we used the average value for the horizontal and normal forces applied to the buttocks after measuring 201 stable samples for each subject. The two conditions were measured in random order with one trial for each condition. The participants were permitted to rest between trials. The relationship between the forces applied to the buttocks and those applied to the back support was also considered by visually inspecting the data.
Statistical analyses
The measured horizontal and normal forces applied to the buttocks were normalized by body weight (percent body weight (%BW)), based on the raw data from the force plate in order to correct the effects of body weight. We used Shapiro–Wilk’s normality test as a preliminary analysis of the horizontal and normal forces applied to the buttocks. To investigate the influence of the height of the back support rotational axis position, the horizontal and normal forces in the three reclining phases (IUP, FRP, and RUP) were compared between the two experimental conditions. For statistical analysis, a paired t-test was performed with the level of significance set at p < 0.05. In addition, to investigate the changes in the horizontal and normal forces applied to the buttocks by reclining the back support, the forces created in the two experimental conditions were compared among the three reclining phases. The statistical analysis involved one-way analysis of variance (ANOVA) and Bonferroni’s multiple comparison tests with a level of significance set at p < 0.05. The statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) ver. 16.0J for Windows (SPSS, Chicago, IL, USA).
Results
Table 1 shows the measured horizontal and normal forces applied to the buttocks, and Figure 2 shows the wave representing the fluctuation pattern of the forces in a typical example.
The forces applied to the buttocks on various back angles (n = 13).
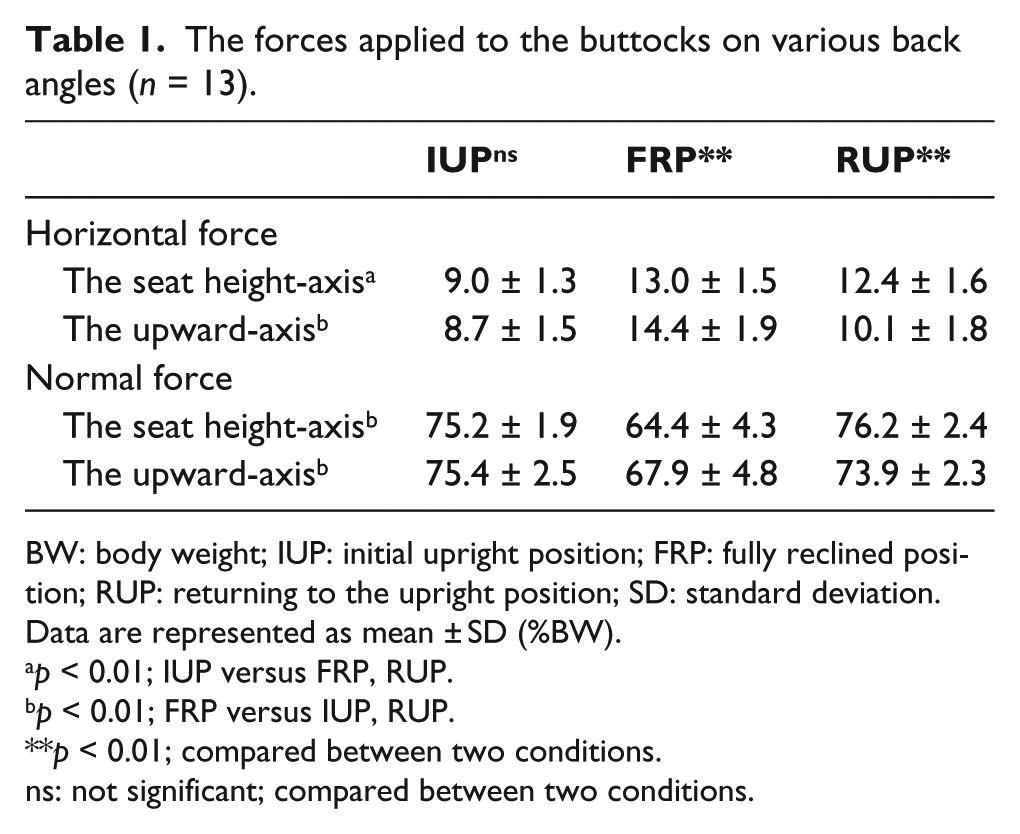
BW: body weight; IUP: initial upright position; FRP: fully reclined position; RUP: returning to the upright position; SD: standard deviation.
Data are represented as mean ± SD (%BW).
p < 0.01; IUP versus FRP, RUP.
p < 0.01; FRP versus IUP, RUP.
p < 0.01; compared between two conditions.
ns: not significant; compared between two conditions.
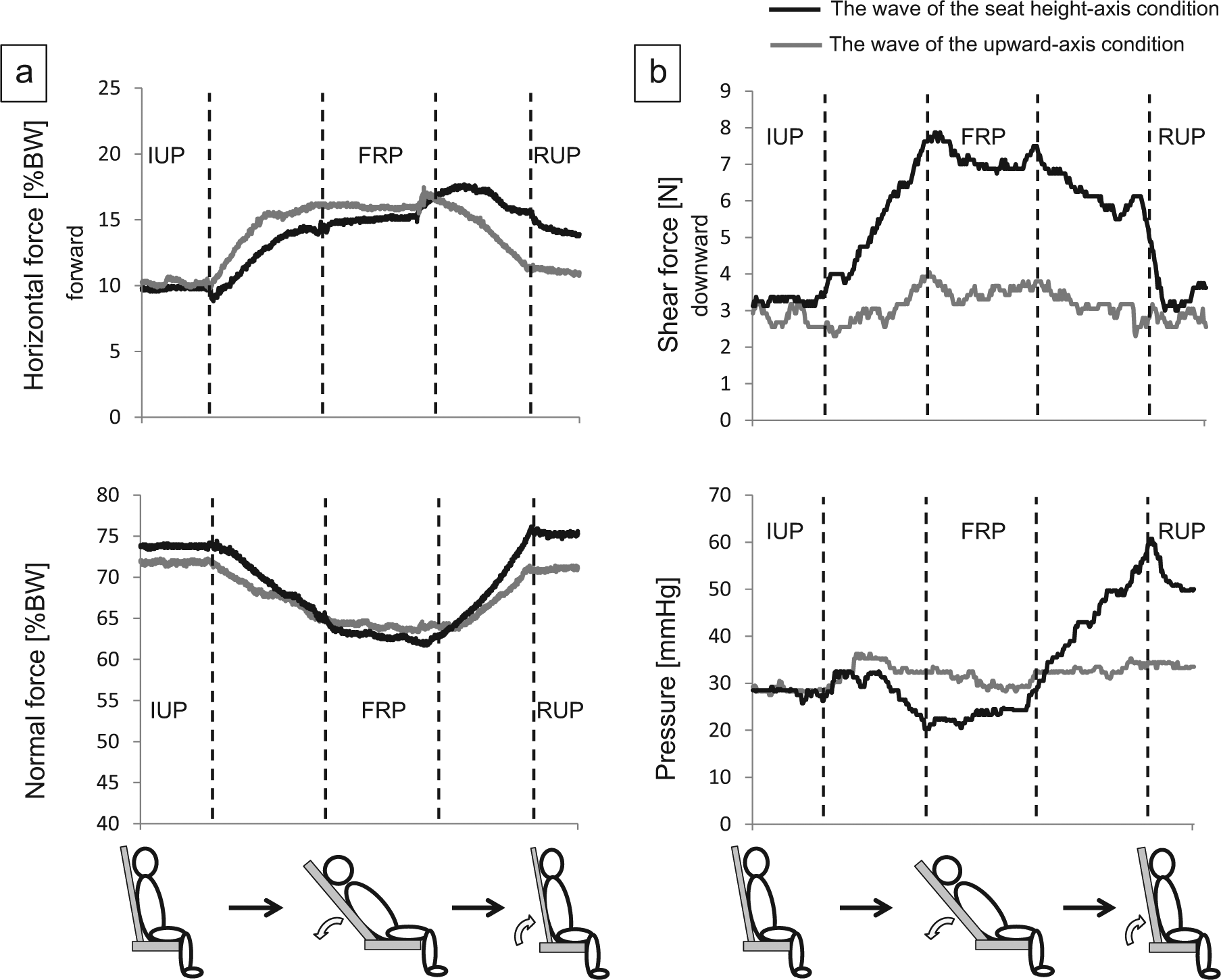
The wave of fluctuation pattern of the forces (the typical example): (a) the forces applied to buttocks and (b) the forces applied to back support.
In the seat height-axis condition, the average value of the horizontal force applied to the buttocks was 9.0%BW ± 1.3%BW in the IUP, 13.0%BW ± 1.5%BW in the FRP, and 12.4%BW ± 1.6%BW in the RUP. In the upward-axis condition, the value of horizontal force was 8.7%BW ± 1.5%BW in the IUP, 14.4%BW ± 1.9%BW in the FRP, and 10.1%BW ± 1.8%BW in the RUP. In addition, in the seat height-axis condition, the average value of the normal force applied to the buttocks was 75.2%BW ± 1.9%BW in the IUP, 64.4%BW ± 4.3%BW in the FRP, and 76.2%BW ± 2.4%BW in the RUP. In the upward-axis condition, the value of normal force was 75.4%BW ± 2.5%BW in the IUP, 67.9%BW ± 4.8%BW in the FRP, and 73.9%BW ± 2.3%BW in the RUP. A significant difference in the horizontal and normal forces applied to the buttocks appeared during the FRP and the RUP phases when comparing the two experimental conditions (p < 0.01). In addition, the horizontal and normal forces applied to the buttocks showed significant differences when compared among the three reclining phases (p < 0.01).
The fluctuation patterns of the measured forces are described below. The fluctuation patterns for the measured forces were similar for all subjects; however, the fluctuation phases of the horizontal forces applied to the buttocks differed for each condition. During the IUP to FRP phase, the value of the horizontal force showed a significant increase under both conditions. Subsequently, during the FRP to RUP phase, the horizontal force showed a significant decrease under the upward-axis condition, but did not change under the seat height-axis condition. The wave of the normal force applied to the buttocks showed a similar pattern, with a significant decrease in the FRP, under both conditions. Under the seat height-axis condition, the downward shear force on the back support showed a remarkable increase from the IUP to FRP phase, and the pressure showed a remarkable increase from the FRP to RUP phase. On the other hand, under the upward-axis condition, neither the shear force nor the pressure showed a remarkable change through the phases.
Discussion
In this study, a force plate was used to examine the influence of the height of the rotational axis position on the horizontal force applied to the buttocks as a step toward understanding how to prevent decubitus ulcers in individuals using wheelchairs with reclining back supports. During the FRP, the horizontal force applied to buttocks under the upward-axis condition was significantly higher than under the seat height-axis condition, but the difference was equivalent to about 1.4%BW. In addition, the horizontal force in the forward direction under both conditions was significantly higher in the FRP than in the IUP. The L-shaped pieces that were placed between the back support and the seat frame allowed the lower end of the back support to move downward as the back support was reclined. Because the distance between the seat and the upper end of the back support was short, the trunk also shifted downward. Therefore, the horizontal force applied to the buttocks during the FRP phase was higher than that in the IUP. Gilsdorf et al. 16 reported that the horizontal force occurred in a backward direction during the FRP phase. The differences in the results of these two studies may be due to the low value of the static friction force applied to the back support in this study because of the difference in the position of the rotational axis. If the static friction force increased, it might attenuate the horizontal force increase applied to the buttocks.
However, as the trunk slides upward when the back support is moved backward, the stress on the body may increase. Therefore, the motion of the back support and trunk while reclining should be investigated in greater detail. Furthermore, Carlson et al. 28 have described techniques to minimize friction/shear in wheelchair seating through the orientation of the seat surface, positioning of the foot supports, and the use of low-friction seat cover materials. Thus, to prevent an increase in the shear force during the FRP, consideration should be given to all of the wheelchair’s parts, including the tilting mechanism of the seat.
During the RUP phase, the horizontal force applied to the buttocks under the upward-axis condition was significantly lower than that under the seat height-axis condition. In previous studies,20,29 we reported that the horizontal force applied to the buttocks fluctuated greatly, leading to a greater distance between the rotational axis of the back support and the hip joint, which is the rotational axis of the trunk–pelvis. In this study, the position of the rotational axis of the back support, under both experimental conditions, is close to the hip joint and on the horizontal plane, but the conditions were dissimilar with respect to the height of the rotational axis. The inclination angle of the back support and the trunk may show similar changes because the height of the rotational axis was close to the hip joint under the upward-axis condition. Therefore, the forces applied to the back support under the upward-axis condition were lower than those under the seat height-axis condition. In addition, a shear force can exist only when two surfaces are pressed against each other.
Goossens et al. 8 indicated that the maximum shear force just before sliding occurs is defined by the equation
where f is the coefficient of friction and FN is the normal force. This implies that in regions where the pressure is relatively high, the shear force can also become high. This formula is similar to the formula for calculating the maximum static friction force. If we define Fs, friction, max as the maximum static friction force, the friction force cannot be greater than Fshear, max or Fs, friction, max. Thus, there is a strong relationship between shear and frictional forces. The static friction force applied to the back support may be low under the upward-axis condition, in which the pressure applied to the back support was also low. Other authors reported that the trunk slides upward on the back support during the return to the upright position. 30 However, if the static friction force applied to the back support is high, the trunk does not slide upward easily. As a result, the force applied to the back support causes the buttocks to slide forward, producing horizontal force to the buttocks. 31 Under the upward-axis condition, which is presumed to generate the lowest static friction force on the back support, the reaction force can be released without restricting the relatively easy upward slide of the trunk. Thus, the horizontal force applied to the buttocks was significantly lower under the upward-axis condition. In a previous study, 20 the horizontal force applied to the buttocks was measured when the rotational axis of the back support was positioned at the intersection of the seat and the back support, defined as the point farthest back in the seat. During the RUP phase, the horizontal force applied to the buttocks was about 17%BW under these conditions. Compared with the horizontal force under the upward-axis condition, the horizontal force could be reduced about 7%BW by moving the rotational axis closer to the hip joint.
Cushions are commonly used to prevent decubitus ulcer formation in individuals requiring the use of reclining wheelchairs. Therefore, the results of this study suggest that reclining wheelchairs should possess the function of adjustment of the height of the rotational axis not only the location of the rotational axis of the back support on the horizontal plane in order to reduce the horizontal force applied to buttocks during the RUP.
Limitations
A limitation of this study was that it included only healthy, adult males. In addition, because the measurement times were short, we could not evaluate the effect of delayed postural collapse. In addition, regarding the methods of this study, it should be considered that the highest pressure point on the back support detected by the sensor was determined manually by the examiner’s palpation, and the forces were measured on one trial per condition in order to improve validity of these results on this study. In addition, this study did not consider the force peak values and fluctuations of these forces during two phases of transition on reclining the back support. Furthermore, the form, material, and coefficient of friction of the experimental wheelchair’s seat were different from those used to measure the shear forces. Moreover, we could not consider microclimate factors (i.e. urinary incontinence and sweat) that interact with the frictional force; these problems affect many wheelchair users. Therefore, direct extrapolation of the results of this study to all wheelchair users is difficult.
Conclusion
The current results suggest that reclining wheelchairs might require the function of adjusting the height of the rotational axis of the back support in wheelchair-bound individuals. In the future, we plan to investigate the influence of the seat material and the frictional force of the back support on the shear force applied to buttocks while reclining the wheelchair. Furthermore, these results need to be adapted for all wheelchair users.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors report no conflicts of interest.
Funding
This study was supported by a grant-in-aid from the 2010 Kawasaki University of Medical Welfare’s expense budget for medical welfare study and research.