
Abstract
Background:
Despite the fact that the number of disabled individuals participating in sports is increasing, there are only sparse reports in the literature concerning overuse injuries.
Objectives:
The purpose of this study was to compare scapular resting position, shoulder pain, and function in wheelchair basketball, amputee soccer, and disabled table tennis players.
Study design:
Descriptive study.
Methods:
A total of 63 disabled players from amputee soccer, wheelchair basketball, and disabled table tennis participated in our study. Scapular resting position was taken as primary outcome; pain and function were taken as secondary outcome measurements. Scapular resting position was evaluated with Lateral Scapular Slide Test. Visual Analog Scale was used for evaluating shoulder pain intensity. Quick disabilities of the arm, shoulder, and hand questionnaire were used to assess upper extremity function.
Results:
There was a significant difference in shoulder pain, function, and scapular resting position in all groups (p < 0.05). Paired comparisons between amputee soccer and wheelchair basketball players and also amputee soccer and disabled table tennis showed difference for all measurement parameters (p < 0.05).
Conclusion:
When the results are evaluated, it may be stated that amputee soccer players have better scapular resting position than other sports. Crutch usage may not negatively affect scapular resting position and perceived function as much as wheelchair usage. Exercise techniques for shoulder and resting position could be included in training programs of disabled athletes.
Clinical relevance
Wheelchair/crutch usage is a risk, and special exercise techniques for shoulder and dyskinesis could be included in training programs to prevent injury. However, it may not just be important for wheelchair athletes, it may also be important for amputee soccer players. In particular, total upper extremity evaluations and exercises could be added within exercise programs.
Background
After the 1960s, sport activities for disabled people gradually increased with developments in medicine and special operation techniques, demands, and production of adaptive device for sport activities. 1 Individuals with physical disabilities participate in many sports including high-level activities such as track and field, basketball, swimming, and table tennis. Most of these disabled sports could be adapted for rehabilitation programs, so that people with disabilities become more productive and they take active roles in social life. Also, they overcome their disabilities more easily; their motivation and functional levels are increased. 1 Besides the beneficial effects of sport, long training hours and intensive competition schedule increase rate of injury in athletes. 2
There is a lack of evidence concerning the etiology of shoulder pathology in the sports of wheelchair basketball, amputee soccer, and disabled table tennis. Most of the abnormal biomechanics and overuse injuries that occur about the shoulder girdle may be traced to alterations in the function of the scapular-stabilizing muscles.3,4 The abnormal scapular biomechanics occurring from dysfunction may predispose to shoulder injuries.4–6 Also, shoulder pain and scapular and functional problems commonly occur as a result of shoulder injuries. 7 However, abnormal scapular biomechanics are not always associated with athletes with painful shoulder. 8
Wheelchair athletes are at particular risk for overuse injuries of the shoulder complex due to repetitive use of the upper extremities for propulsion. Repetitive wheelchair propulsion mechanics encourage repetitive protraction of the scapula, which has been suggested to lead to altered posture, weaker scapular stabilizers, and tighter anterior muscles. Also, compensatory muscle imbalances may develop at the shoulder because of long-term wheelchair propulsion or training program deficient in the strengthening of the rotator cuff and scapular stabilizer muscles. This can lead to musculoskeletal injury in those athletes participating in sports, which require different movement patterns such as in swimming, throwing, or racquet sports. 9 In addition to wheelchair athletes, amputee athletes who use conventional crutches have the same problems but in different ways. Although using conventional crutches is necessary, it can present numerous problems for crutch users. 10 Conventional axillary crutches transmit jarring forces to the wrists and shoulders and can cause injuries to the crutch user. 11 As support and device usage are important for disabled sports, it is also important for daily living activities. Shoulder- and scapula-related pathologies that develop with or without devices are very important for functionality in sports and daily living. There are no studies specific to shoulder injury mechanisms of disabled table tennis players in the literature. However, according to study in the literature, 12 predominance of shoulder injuries was observed with 32% in paralympic table tennis athletes.
Although there are lots of disabled athletes and disabled sporting activities still developing, the literature is limited about injuries in disabled sports.12,13 Wheelchair basketball, disabled table tennis, and amputee soccer are the three important sports in the Paralympics and also are at great risk of shoulder and scapular pathologies, which could lead to the end of their participation in sport. To our knowledge, there was no study investigating shoulder problem in these three disabled sports.
The purpose of this study is to compare the scapular resting position, shoulder pain, and function in wheelchair basketball, amputee soccer, and disabled table tennis players. Our hypothesis was that there is no significant difference in scapular resting position, shoulder pain, and function in wheelchair basketball, amputee soccer, and disabled table tennis players.
Methods
Participants
A total of 63 disabled players participated in this study, including 19 male athletes (age = 29.0 ± 6.4 years; body mass index (BMI) = 22.9 ± 2.1 kg/m2) from amputee soccer, 22 male athletes (age = 25.2 ± 9.1 years; BMI = 21.2 ± 3.6 kg/m2) from wheelchair basketball, and 8 female (age = 20.0 ± 2.7 years; BMI = 18.2 ± 1.1 kg/m2) and 14 male athletes (age = 20.4 ± 2.5 years; BMI = 20.0 ± 6.0 kg/m2) from disabled table tennis. Descriptive and clinic characteristics of subjects are shown in Table 1.
Descriptive and clinical characteristics of disabled players.
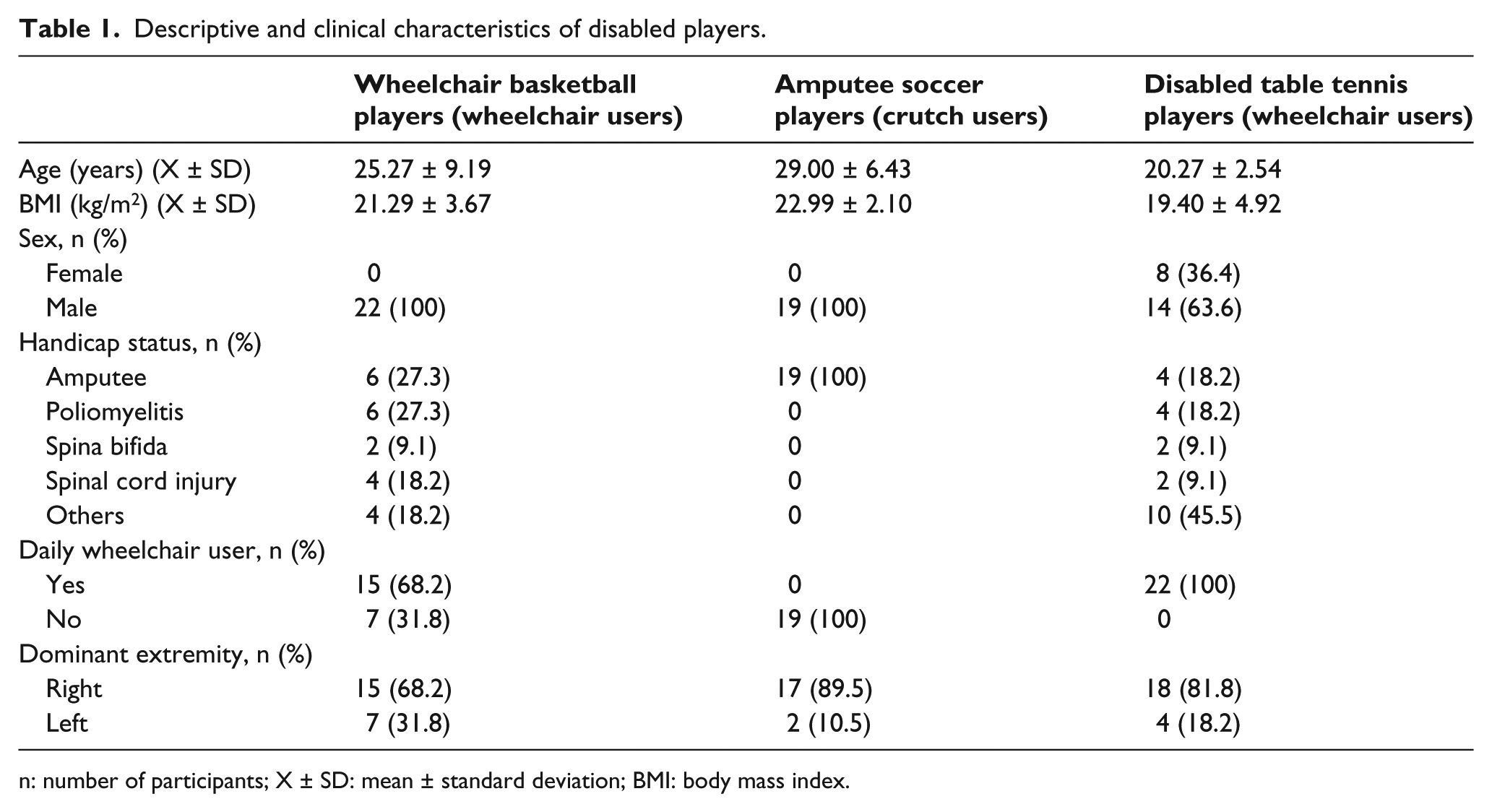
n: number of participants; X ± SD: mean ± standard deviation; BMI: body mass index.
Ethical approval was from the Turkish Sports Federation of the Physically Disabled. Before study participation, all subjects were informed verbally for the details of the study, and all of them signed informed consent forms. All procedures were performed in accordance with the Declaration of Helsinki.
The eligibility criteria were as follows:
≥15 years old;
Having played disabled sport for at least 6 months prior to the start of the study.
Exclusion criteria were as follows:
Suffering from any chronic problems, upper-extremity-effected neurologic disorders, or systemic disease (diabetes mellitus, hypertension, and heart disease);
Having any type of (C or S) scoliosis or cervical problems;
Having any scar or wound in the measurement regions.
The sample size required to detect significant differences was determined as 16 subjects in each group with the alpha level set at 0.05 to achieve 95% powers with scapular resting position as primary outcome. 14
Measurements
All of the measurements were done by the same physiotherapist. The data related to the descriptive and clinic characteristics of the subjects were collected before the study began. Scapular resting position was taken as primary outcome; pain and function were taken as secondary outcome measurements.
Scapular resting position
Scapular resting position was evaluated with the Lateral Scapular Slide Test (LSST) designed by Kibler to evaluate scapular asymmetry under varying loads. According to Kibler, 15 three test positions were used. 16 For test position 1 (LSST-1), subjects were instructed to keep their upper extremities relaxed at their sides. In test position 2 (LSST-2), subjects were instructed to actively place both hands on the ipsilateral hips and, consequently, the humerus was positioned in medial rotation at 45° of abduction in the coronal plane. In test position 3 (LSST-3), subjects were instructed to actively extend both elbows and to elevate with maximal internal rotation at both upper extremities to 90° in the coronal plane. In this procedure, the distance between inferior aspect of the inferior angle of the scapula and the closest spinous process in the same horizontal plane was measured bilaterally with a tape measure for all three positions. A difference of 1.5 cm or more in any of the three positions was considered a positive result of the LSST. Kibler reported that the test–retest (intratester) ratio of LSST ranges from 0.84 to 0.88, and that the intertester reliability ranges from 0.77 to 0.85, depending on the position, and he suggested that LSST is reliable in terms of reproducibility (Figure 1(a) to (c)).15–17 In this study, LSST was assessed at modified position of sitting.

(a) LSST Position 1, (b) LSST Position 2, and (c) LSST Position 3.
Pain
A visual Analog Scale (VAS) was used for evaluating shoulder pain intensity during game. 18 Subjects were asked to indicate intensity by marking a 100-mm-long horizontal line that was labeled with the anchors, “no pain,” on the one hand, and “worst pain possible,” at the other. This required the subjects to be able to equate the length of the line (as measured from the left-hand side to the point marked) with the amount of pain they were experiencing. 19
Perceived function
Perceived function as defined in this study was a person’s perceived ability to perform activities of daily living and some higher level activities such as those specific to disabled athletics. Perceived function of upper extremity may include activities of daily living, athletic participation and cognitive function. The Turkish version of the quick disabilities of the arm, shoulder, and hand questionnaire (Q-DASH-T) was used to assess upper extremity perceived function. Q-DASH-T was developed to measure physical disability and symptoms for all upper extremity disorders. The Q-DASH-T is a shortened version of the DASH outcome measure. The questionnaire consists of a disability/symptom scale (11 items) and two optional scales: work (4 items) and sports/performing arts (4 items). To calculate a Quick DASH score, at least 10 of the 11 items must be completed similar to the DASH, each item has five response options, and from the item scores, scale scores are calculated, ranging from 0 (no disability) to 100 (most severe disability).20,21 Reliability of the Turkish version of the Quick DASH Scale was found very good with high internal consistency (Cronbach’s alpha of 0.84 for disability/symptom subscale, 0.937 for work subscale, and 0.926 for sports/performing arts subscale) and test–retest reliability (intraclass correlation coefficient of 0.931 for disability/symptom subscale, 0.925 for work subscale, and 0.779 for sports/performing arts subscale). 21
Statistical analysis
The Statistical Package for the Social Sciences, version 17.0 (SPSS 17.0), was used to perform statistical analysis. Means, standard deviations, and percentiles were calculated for descriptive and clinical characteristics of disabled players.
Kruskal–Wallis analysis was used to compare differences of three groups. Mann–Whitney U test was used in comparison of paired groups. p-value of ≤0.05 was accepted as the level of statistical significance for the comparison data. The normality analyses as the primary outcome of age found 0.001 for three groups. Because of this, we used non-parametric tests. Also, the number of participants in each group led us to use non-parametric tests.
Results
There was a significant difference in shoulder pain, function, and scapular resting position in all groups (p < 0.05). Paired comparisons between amputee soccer and wheelchair basketball players and also amputee soccer and disabled table tennis showed difference for all measurement parameters (p < 0.05). There was no difference found for shoulder pain, function, and dyskinesis (p > 0.05) in comparison of wheelchair basketball and disabled table tennis players (Table 2). Wheelchair-using sports have higher percentages of abnormal scapular resting position (wheelchair basketball (77.3%), disabled table tennis (54.5%)), whereas crutch-using sports (amputee soccer) have better scapular resting position (15.8%). Pain reported is slightly higher in wheelchair basketball players. As we look at Q-DASH-T scores, amputee soccer players have better perceived shoulder functionality than players in wheelchair-using sports.
Outcome measurements of disabled players.
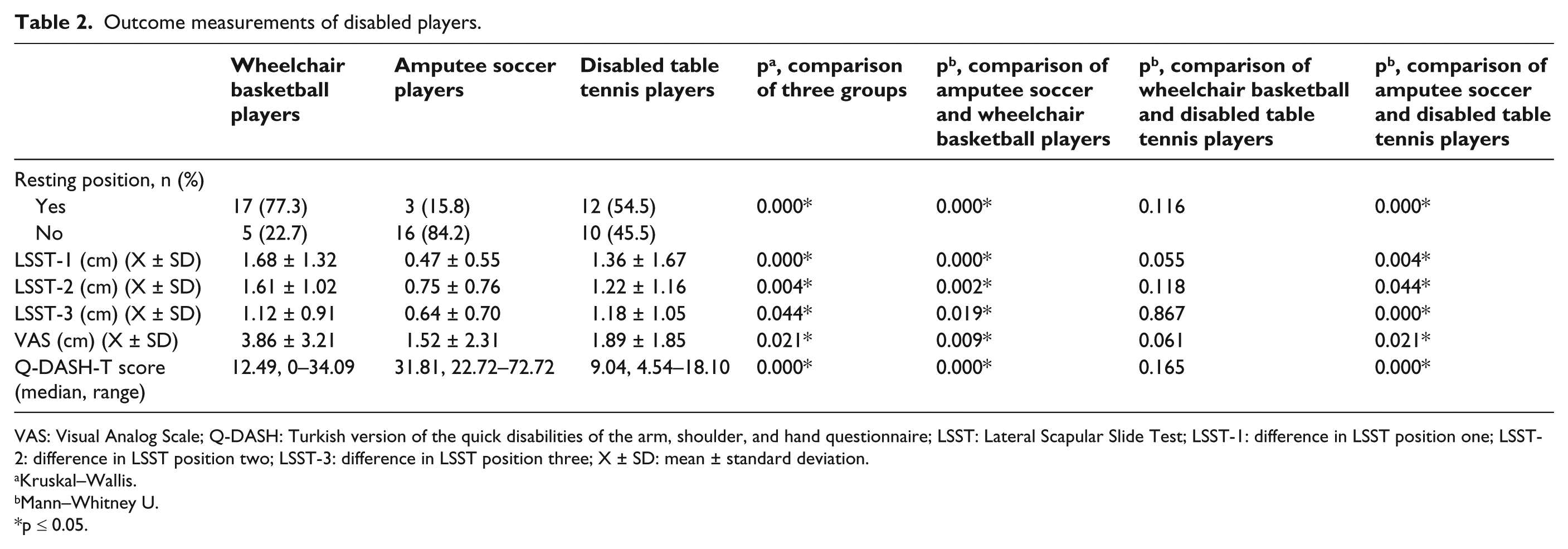
VAS: Visual Analog Scale; Q-DASH: Turkish version of the quick disabilities of the arm, shoulder, and hand questionnaire; LSST: Lateral Scapular Slide Test; LSST-1: difference in LSST position one; LSST-2: difference in LSST position two; LSST-3: difference in LSST position three; X ± SD: mean ± standard deviation.
Kruskal–Wallis.
Mann–Whitney U.
p ≤ 0.05.
Discussion
Participation in sport activities for people with disabilities continues to gain in popularity. With participation in sports, there would be increase in injury and repetitive trauma risk. The chosen disabled sports (amputee soccer, wheelchair basketball, and disabled table tennis) involved in this study are all sports that could affect upper extremity because of the nature of the sports. The use of crutches in amputee soccer, repetitive use of upper extremities for wheelchair propulsion and other sportive positions in wheelchair basketball, and using table tennis racquet in disabled table tennis could be the cause of shoulder or upper extremity problems. Based on these reasons, we compared shoulder pain, function, and scapular resting position in wheelchair basketball, amputee soccer, and disabled table tennis players. When the results are evaluated, it may be stated that amputee soccer players have better scapular resting position than other sports. Crutch usage may not negatively affect scapular resting position and function as much as wheelchair usage.
A previous study 9 reported that wheelchair athletes are at particular risk of overuse injuries of the shoulder complex due to repetitive use of the upper extremities for propulsion. Also, compensatory muscle imbalances may develop at the shoulder from long-term wheelchair propulsion, or from a training program deficient in the strengthening of the rotator cuff and scapular stabilizer muscles. This can lead to musculoskeletal injury in those athletes participating in sports requiring different movement patterns such as in swimming, throwing, or racquet sports. 9 Although the recent literature mentions the relationship between wheelchair athletes and shoulder problems, it does not involve amputee soccer or disabled table tennis players and their relation with shoulder problems. However, according to our knowledge, it could be in similar relation also in these two sports.
The results of this study indicated that there were shoulder pain, function, and dyskinesis problems in wheelchair basketball, amputee soccer, and disabled table tennis. Scapular resting position could lead us to symptoms such as pain, muscle weakness, loss of control, and crepitation.22,23 Pain and dyskinesis are found worse more in wheelchair basketball, disabled table tennis, and amputee soccer players. This expected result could be the cause of the wrong positioning in the wheelchair. A study 24 reported that sitting posture is important, as it is related to the wheelchair athlete and shoulder mechanics. Typical posture is posterior pelvic tilt, increased thoracic kyphosis, and forward head position in wheelchair. Such posture results in anterior displacement of the shoulder girdles. This positional issue can become a structural deformity when abnormal shortening of the anterior soft tissue structures occurs (i.e. pectoral muscles and anterior capsule) and combines with a compensatory lengthening posteriorly and relative weakness of the scapula thoracic muscles. 25 Weakness of the scapula thoracic muscles potentially leads to abnormal positioning of the scapula, disturbances in scapula humeral rhythm, and generalized shoulder dysfunction. 26
Wheelchair propulsion and other required sportive positions appear to be related to high mechanical loads on the upper extremity in wheelchair basketball. Commonly, use of upper quarter of the body in daily life and manual wheelchair usage causes high mechanical burden on upper extremities. Disabled table tennis sport is the secondary sport in which loading of the upper extremity is affected as we found in our study. Repeated upper extremity movements at or above shoulder level, trunk movements, and compensatory shortening of neck and anterior muscles of shoulder girdle during the table tennis could be the reason for shoulder pain and dyskinesis in addition to daily living loading. 27 Otherwise, comparison of the results between amputee soccer with wheelchair basketball and disabled table tennis showed differences in this study. Hence, there are many reasons of shoulder problems that could be different in wheelchair and crutch sports. Loading mechanisms are different in two types of sports. Mechanisms of the sports and loading directions are different in both sports, so these could be the cause of the difference. There are harsh forces on the body due to crutch walking with axillary crutches. 28 Forces at the crutch tip are transferred directly to the hand and wrist and indirectly to the axilla. Based on the nature of crutch usage, the same forces play a part in amputee soccer in similar ways. In the literature, rolling resistance is defined in wheelchair usage. In daily use, rolling resistance generally is the major resisting force and body weight is one of the factors, which increases in direct proportion to it. 7 In crutch usage, one’s body weight creates downward direction of resultant force and its effects on the upper extremity are more direct. Also, most of the body weight is on anterior part of the vertebral column that is why strong back muscles are necessary to compensate. These muscles are important for fine postural movements. Superficial back muscles, such as trapezius, latissimus dorsi, rhomboids, and levator scapulae, connect the upper extremity with the scapula and control extremity movements. The latissimus dorsi is very important for amputee players who use two crutches. It causes adduction, extension, and medial rotation of the humerus. Therefore, it is called the climbing muscle. 29 Due to movement pattern in crutch usage, the latissimus dorsi could be the most used and effected muscle. Considering our results, these could be the reasons for the difference that we stated before.
The results of this study showed that amputee soccer players’ functionality scores were higher than others. There could be several reasons; Q-DASH does not only evaluate shoulder joint but also evaluates elbow and hand functions. Crutch usage causes pressure on axillar region of the body in daily life, or amputee soccer could be another reason. A previous study 11 stated that this can impair conduction in the damaged nerves and can lead to total or partial paralysis in some of the muscles of the arm and hand. In addition to this, forces at the crutch are transferred directly and primarily to the hand and then wrist before the shoulder.
Limitations and implications for further study
There are several limitations of this study. Only three types of disabled sports are compared in this study. Other disabled sports with adaptive devices and their effects could be measured. Gender discrimination could be done, but some sports like amputee soccer are only played by male disabled players. More objective outcome measurements such as magnetic resonance imaging or three-dimensional (3D) scapular motion analysis methods could be used to evaluate whether there are any shoulder, upper extremity, or scapular disorders. In the assessment of scapular resting position, different tests (scapular reposition, scapular retraction, and scapular assistance tests) such as manual muscle tests, posture analysis, pectoralis minor, and posterior shoulder tightness could be used to increase reliability of LSST. Finally, LSST measurements were done at sitting position. This is a modified position for LSST and could change the posture and hence the position of the scapula. As some of our participants had no chance to take the original LSST position, a modified position was used. In addition, a limitation of the study is the lack of control group.
Conclusion
We may speculate that wheelchair and crutch usage are a risk and preventive physiotherapy and shoulder evaluations are important to prevent injuries. Special exercise techniques for shoulder and dyskinesis could be included in training programs. However, it is not just important for wheelchair athletes; it is also important for amputee soccer players. Especially, total upper extremity evaluations and exercises could be added within exercise programs. It is not easy to interpret this study to general disabled sports, and future studies with large sample size are recommended.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.