
Abstract
Background:
The use of a finger prosthesis following finger amputation is a common approach that is linked to many factors.
Objectives:
The aim of this study was to evaluate the effect of a new method of suspension on quality of life, satisfaction, and suspension in these patients.
Study design:
Quasi-experimental.
Method:
A total of 24 patients with finger amputation and 12 healthy subjects as control group participated in this study. Two types of finger prostheses with conventional suction suspension and new method suspension were provided. A force gauge was used to evaluate suspension force along with a World Health Organization Quality of Life-BREF questionnaire instrument. Satisfaction of the prosthesis was also evaluated using a visual analog scale.
Results:
There was significant difference in quality of life assessment between the patient group and healthy control group, but there was no statistical difference (p > 0.05) between the two patients groups at baseline and after prosthesis use. Using finger prosthesis improved all domains after prosthesis wearing in patients with finger amputations. There were significant differences (p < 0.05) between the two types of prosthesis in terms of suspension and satisfaction.
Conclusion:
Wearing the prosthesis with the new method of suspension had an effective role in terms of providing suspension and an increase in satisfaction in patients with finger amputation.
Clinical relevance
Patients with finger amputation usually use a prosthesis with a simple suspension technique, yet many of these patients experience atrophy and subsequently loss of appropriate suspension. This paper presents a new method of suspension and showed that using this approach improved satisfaction and suspension in patients with finger amputation.
Background
Finger amputation and partial finger amputation are common injuries that occur to the upper extremity. Traumatic injuries, congenital absences, or malformations are the most common causes of these amputations. 1 Loss of digits in the hand has psychological and physical effects which can have an impact on patients. From a psychological perspective, this includes people’s attention to the amputated hand, and reduction of grasp strength and security from a physical perspective.2–4
Prosthetic reconstruction is a common approach in rehabilitation of finger amputation. 5 Prosthetic rehabilitation is related to many factors, which include enhancing natural appearance, eliminating dysfunction, and providing efficient psychological satisfaction and suspension. Suspension has an important role in providing prosthesis function via decreased displacement of prosthesis on the stump. Suction, adhesive, anatomical, and mechanical approaches (e.g. ring) are current methods used to provide suspension in finger prosthesis to maintain prosthesis on residual limb.
Leow et al. 6 demonstrated that a 5%–7% circumference reduction in the finger positive model was an effective approach to provide good suspension in thimble-type prosthesis for distal finger amputations. Kini et al. 5 also showed that a snug fit of the silicone prosthesis on the tissue of the stump reduced accurately by around 0.5–1 mm of the positive stump model. Through this method of suspension, they fabricated a silicone finger prosthesis which had good suspension and adequate function, and was comfortable to use and aesthetically acceptable to a 32-year-old male patient. 5 In an evaluation of a new method of suspension, Mohammad et al. 7 provided a number of ridges on the inner socket of finger prosthesis. They showed that the measured suspension forces in this new design are more than that of the conventional finger prosthesis. 7 In a separate study, Arazpour et al. developed a new method in providing suspension in fabrication of digit prosthesis. In this approach, the socket was reduced by 2 mm less than the original value, and a central tunnel with 4 mm width and depth with length matching the distance between the end of the stump and the nail section was provided. This method, however, was only evaluated in one patient with a finger amputation and the findings showed that the finger prosthesis had acceptable suspension, was user-friendly and of a light design. 8
Patients with finger amputation may have low self-esteem and post-traumatic stress symptoms.4–10 Finger prostheses provide nonoperative rehabilitation seeking to provide function, aesthetic satisfaction, and quality of life (QOL). The evaluation of QOL in subjects with finger amputation associated to prosthetic rehabilitation may provide valuable data to assist the prosthetic rehabilitation team in treatment planning, monitoring, and outcome assessment. Although there are many studies evaluating the influences of prosthetic rehabilitation on QOL in individuals with maxillary defects,9–11 recent studies have reported that using facial prostheses had significant enhancement in QOL in patients.12–14 The QOL in subjects with acquired eye and nose amputations was reported to be lower than healthy individuals. 15 To our knowledge, there is no published study evaluating the QOL in patients with finger prostheses. Therefore, the aim of this study was to evaluate the effect of a new method of suspension on QOL, satisfaction and suspension in subjects with finger amputation. It is hypothesized that patients with finger amputation would have lower QOL scores than the control healthy group. Significant differences would exist between patients who used different types of finger prostheses in satisfaction and suspension.
Methods
Subjects
A total of 24 patients (18 males and 6 females) with finger amputation participated in this quasi-experimental study. These patients were allocated randomly to two groups, according to the type of the finger prosthesis, as follows: (1) patients wearing conventional finger prosthesis and (2) patients wearing finger prosthesis based on new method of suspension. All patients referred received aesthetic finger prosthesis from the Natel prosthetic center. The age of the patients at the time of receiving prosthesis ranged from 22 to 57 years. Three patients from the 24 patients in this study had multiple-digit loss. In total, 29 amputated fingers (21 patients with one finger amputation, 2 patients with three finger amputations, 1 participant with the two finger amputations) were fitted with the prosthesis. Patients were selected, and met the following inclusion and exclusion criteria: aged 18 years and over, at least 6 months after amputation surgery, have adequate cognitive ability and level of literacy to complete the QOL questionnaire, no persistent or recurrent disease, and a clinically and functionally acceptance of prosthesis after receiving and no injuries to other parts of the body in patients with finger amputation. A total of 12 healthy subjects with no history of mental disorders and systemic diseases, absence of prosthesis or deformity in body, willingness to participate in the study and to give written informed consent, and aged 18 years or older were recruited as the control group. These subjects were matched according to age, body mass index (BMI), and gender with patients with finger amputation who participated in this study. It is not possible to match patients and control groups according to vocation in this study. The demographic information is present in Table 1.
Characteristics of the control and two intervention groups at baseline.
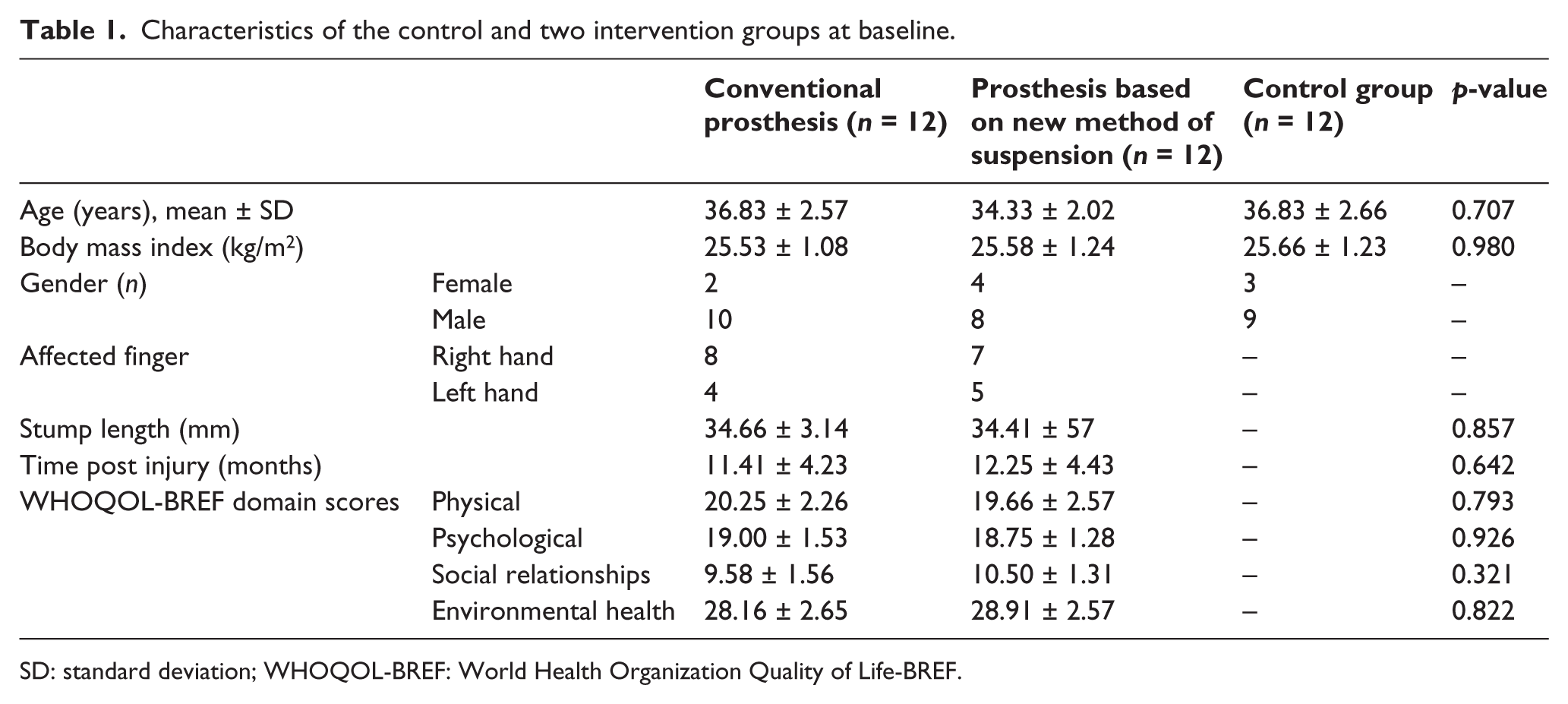
SD: standard deviation; WHOQOL-BREF: World Health Organization Quality of Life-BREF.
Intervention
The amputated finger was lubricated with Vaseline to prepare a negative model and to prevent adhesion of the hand to the casting material. Using alginate (Tropicalgin; Zhermack, Italy) over the palmar and dorsal view of the patient’s hand, a negative cast of the patient’s amputated finger was taken in the neutral resting position. Plaster of Paris was used to provide positive model of stump. To prepare the amputated parts of the finger, a negative cast was taken from the patient’s contralateral uninjured hand (healthy side) in the corresponding finger by alginate. A positive cast of the healthy finger was reconstructed via pouring melting wax (modeling wax; Covex Company, Haarlem, the Netherlands) into the negative cast. A positive cast of healthy finger was put on the positive cast of the stump. A negative cast of the reconstructed finger was prepared via putty impression material (Aquasil putty; Dentsply, Konstanz, Germany). Silicone biomaterial with matching color was prepared and poured into the putty impression cast according to the patients’ hand color.
Two types of prostheses (finger prosthesis with conventional suction suspension and finger prosthesis with new method suspension) were provided for the patients groups. Using a conventional suction method of suspension, the circumference of the positive cast was reduced to 2 mm compared to circumference of stump. However, in the new method, to provide more suction suspension, an additional reduction of stump value, the central tunnel with 4 mm width and depth with length matching the distance between the end of the stump and the nail section was provided. 8 This tunnel provided additional suction system to maintain the prosthesis on stump based on suction mechanism into tunnel. Figure 1 shows finger prostheses that were used in this study.

Finger prosthesis used in this study.
Procedure
The study was approved by the ethics committee at the University of Social Welfare and Rehabilitation Sciences. All patients and subjects were fully informed about the study, and informed consent was obtained from each patient and subject before participation in the study.
Included patients were allocated to two groups: (1) patients wearing finger prostheses with conventional suspension and (2) patients wearing finger prostheses with new method of suspension. Study information was gathered via face-to face interviews with a trained research colleague at the clinic.
Data collection
Force gauge was used to evaluate suspension force. The patients used a constructed prosthesis; gauge of FORCE GAUGE (5000g Model: FG-5005, Lutron Electronic, Taiwan) was attached to the fabricated finger, and the required force to pull (remove) the prosthesis from the stump with the hand in a pronated position on the desk the was noted. This analysis was repeated three times for each condition. The average of the mean forces was considered as the total needed force needed to overcome the suspension.
Demographic and clinical characteristics were collected for all subjects. QOL information was gathered with a World Health Organization Quality of Life-BREF (WHOQOL-BREF) questionnaire instrument twice. The first section was performed in baseline to compare the QOL parameter between the patients with finger amputation and the healthy control group. The second section was performed after 6 weeks of wearing the prosthesis in the patient groups.
The 27-item WHOQOL-BREF includes two overall items measuring general QOL and health condition and 24 items that are universally adopted for the WHOQOL-BREF in four domains: physical health, psychological health, social relationships, and environment. Each subtitle was measured using a 5-point Likert scale, and the domain scores were evaluated on a scale from 0 to 100 to enable comparisons to be made between domains composed of unequal numbers of items. Domains are not evaluated if patients did not answer for 20% of the items or more. If two or more items are missed, domains are not acceptable except in the environment domain, which with two missing items is acceptable to analysis.16,17
Satisfaction of patients in using the prosthesis was evaluated by the visual analogue scale (VAS). The VAS includes a 100 mm horizontal line ranging from 0 (no satisfaction) to 100 mm (high satisfaction). Patients were asked to mark the line vertically at a point which matched their satisfaction. The distance was measured in millimeters and was altered to the same number of points. Figure 2 shows the data collection chart used in this study.
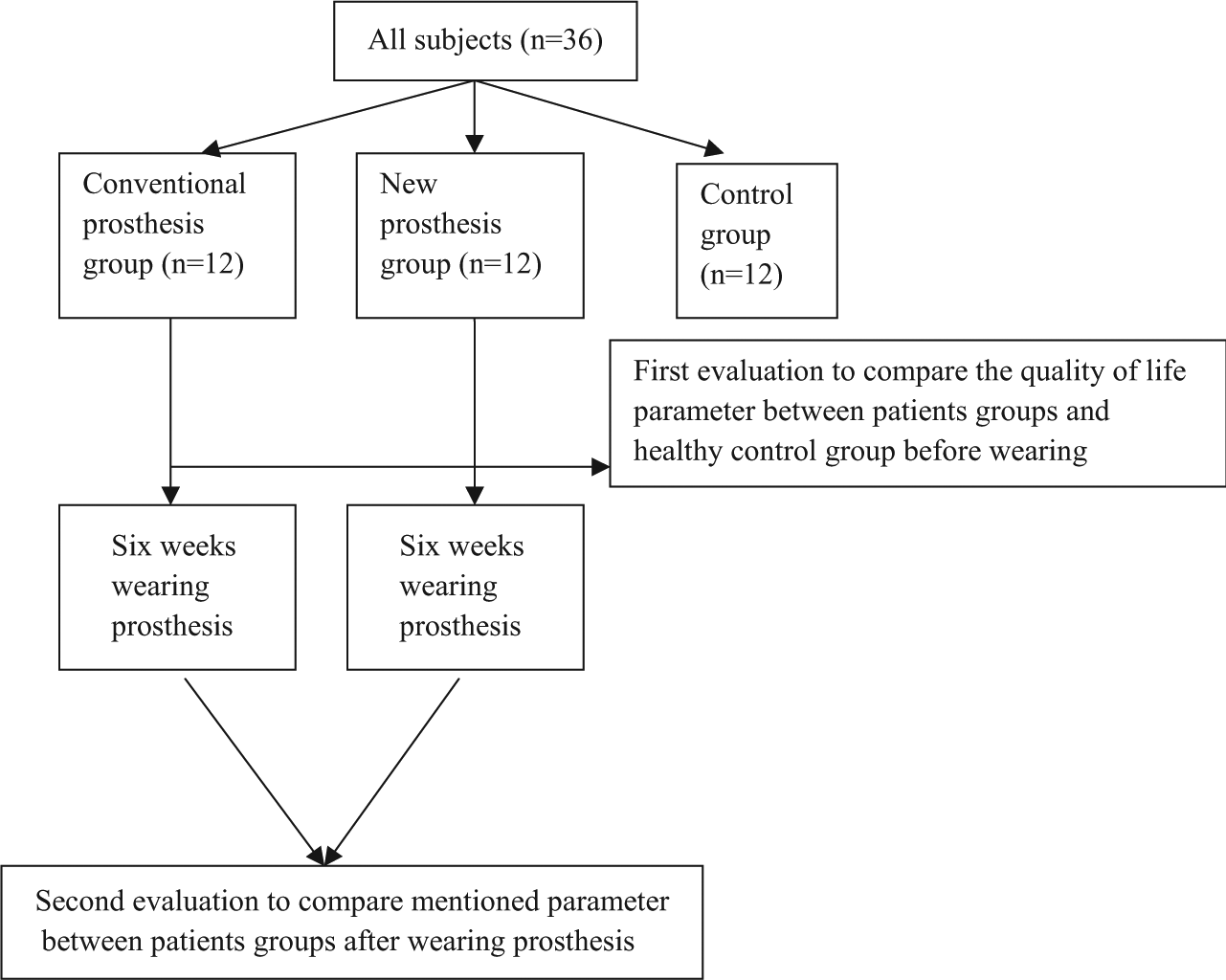
Data collection chart in this study.
Statistical analysis
Normality of data was determined using the Kolmogorov–Simonov test. There were no significant differences (p > 0.05) between patients in the two groups and control group on age and BMI in baseline. A one-way analysis of variance (ANOVA) was used to compare QOL between patients and the healthy control group at baseline. Paired t test was used to evaluate the effect of prosthesis wearing before and after 6 weeks of using. An independent t test was used to compare the patient groups in terms of QOL, suspension strength, and satisfaction. Statistical analyses were done by using IBM SPSS Statistics 16 (SPSS Inc., Chicago, IL, USA). Significant level was considered α = 0.05.
Results
Table 1 shows the information of the patients and control group. There was no significant difference between the three groups in terms of basic variables at baseline. There was no statistically significant difference between the patient groups in terms of stump length, age, and time post amputation (p > 0.05). There were no missing data in the domains of the WHOQOL-BREF in this study. All patients had finger surgery amputation.
There was significant difference in all domains in QOL assessment between patients group and healthy control group, but there was no statistical difference (p > 0.05) in QOL between two patients groups at baseline and after prosthesis using (Table 2). In evaluation of the QOL based on the WHOQOL-BREF, using finger prosthesis improved all domains after prosthesis wearing in patients with finger amputations (Table 3).
Comparison of quality of life parameter between patients with finger amputation and healthy control group before receiving prosthesis at baseline.
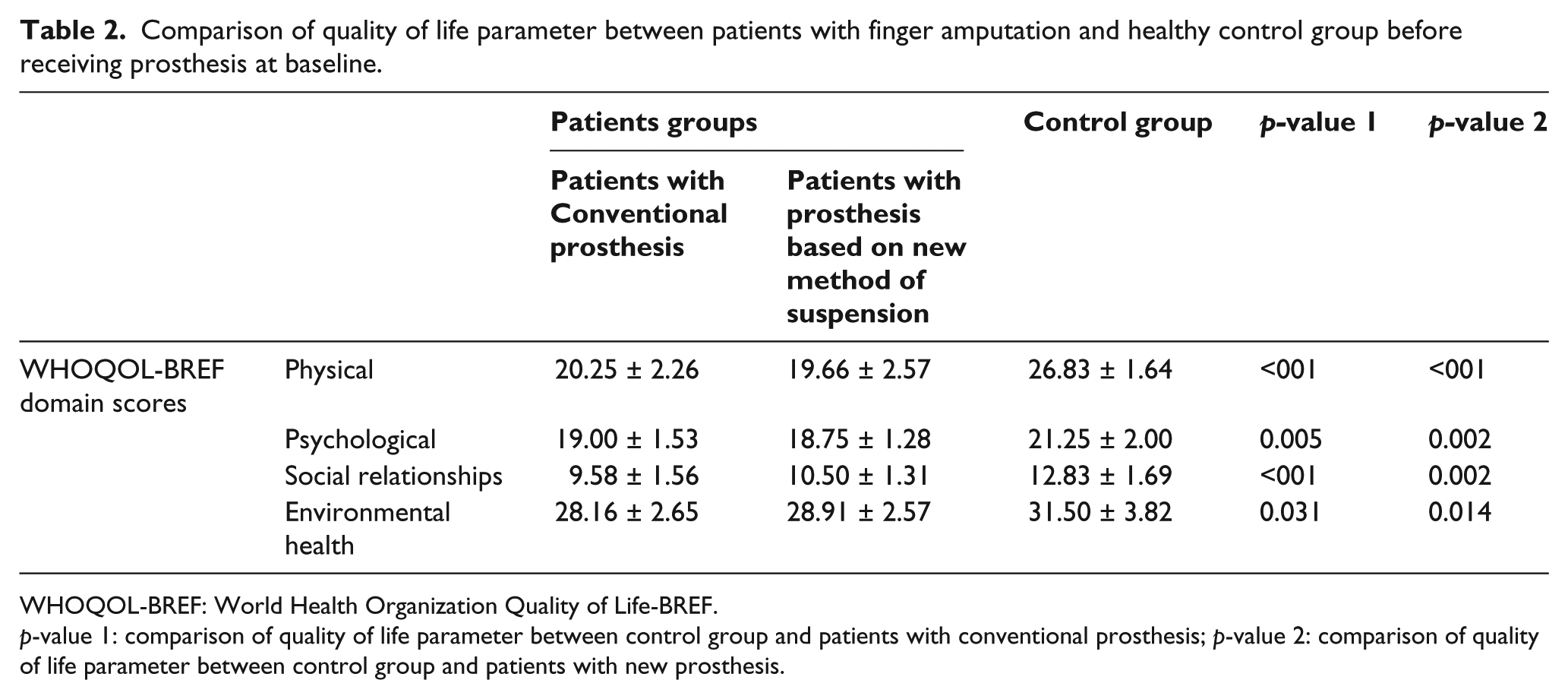
WHOQOL-BREF: World Health Organization Quality of Life-BREF.
p-value 1: comparison of quality of life parameter between control group and patients with conventional prosthesis; p-value 2: comparison of quality of life parameter between control group and patients with new prosthesis.
Comparison of quality of life subscales, suspension strength, and satisfaction inter and intra groups after 6 weeks wearing the prosthesis.
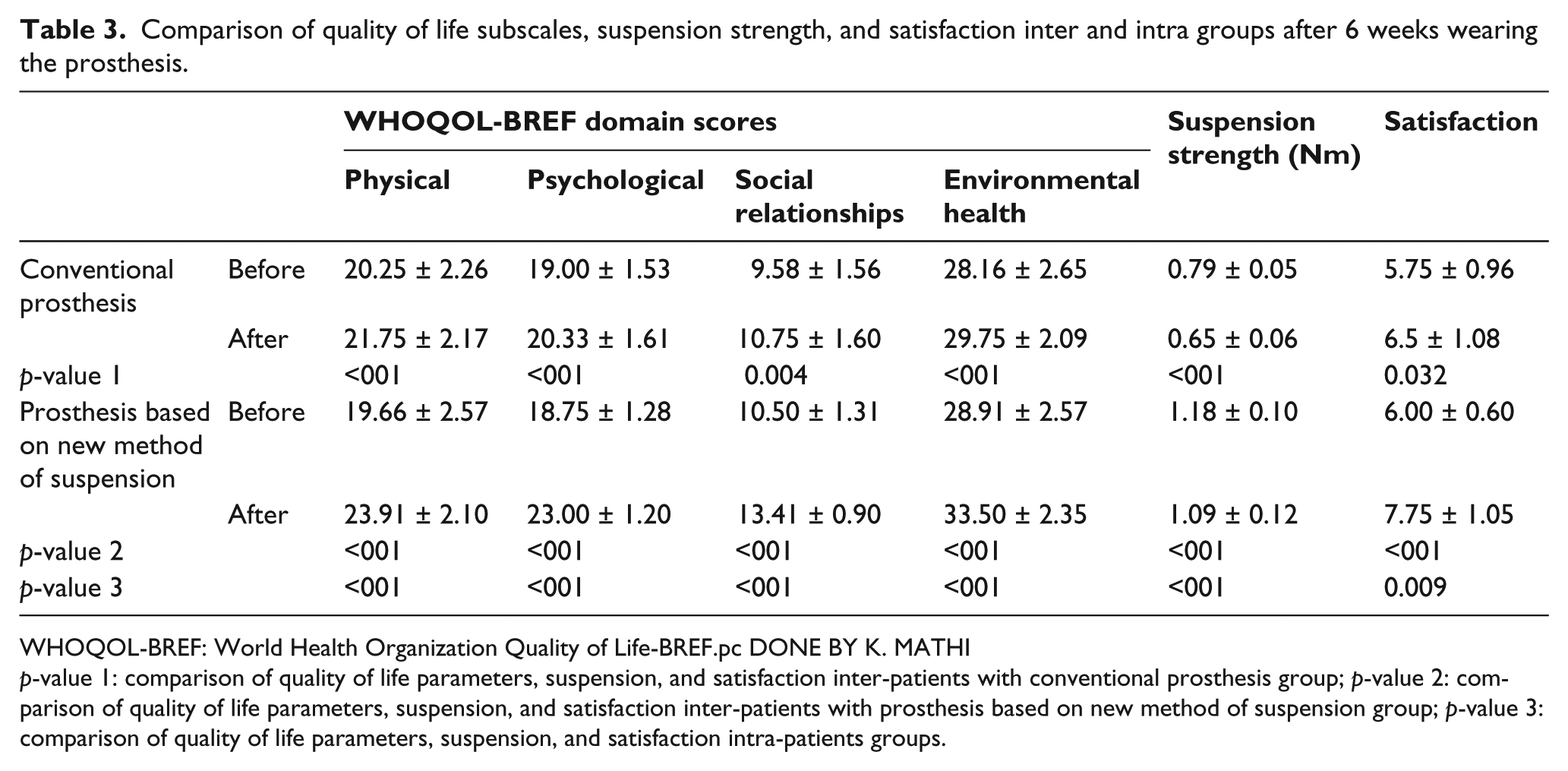
WHOQOL-BREF: World Health Organization Quality of Life-BREF.pc DONE BY K. MATHI
p-value 1: comparison of quality of life parameters, suspension, and satisfaction inter-patients with conventional prosthesis group; p-value 2: comparison of quality of life parameters, suspension, and satisfaction inter-patients with prosthesis based on new method of suspension group; p-value 3: comparison of quality of life parameters, suspension, and satisfaction intra-patients groups.
Table 2 demonstrates the suspension strength and satisfaction in using prosthesis in patients with finger amputation. Although the mean of suspension strength reduced after 6 weeks of wearing the two types of prosthesis in the two patient groups, the reduction rate in the new prosthesis was less than the conventional prosthesis. There were significant differences between two types of prosthesis in these parameters. After 6 weeks of prosthesis wearing, the mean of suspension strength was 0.65 ± 0.06 Nm in using prosthesis with conventional method, while using prosthesis based on the new method of suspension, this rate was 1.09 ± 0.12 Nm. The satisfaction rate in using conventional prosthesis was 6.5 ± 1.08, while using prosthesis based on the new method of suspension increased satisfaction rate in patients with finger amputation to 7.75 ± 1.05 (Table 3).
Discussion
The aim of this study was to evaluate the QOL, suspension strength, and satisfaction of patients with finger amputation at the proximal interphalangeal (PIP) joint. The main purpose of prosthetic rehabilitation is improvement in QOL for amputated patients when using the prosthesis. Analyzing QOL in clinical practice can provide important data for planning and evaluation of extensive prosthetic rehabilitation.14,15,18,19
QOL and satisfaction in patients with facial defects were related to the localization, the causes of defects, the age of used prostheses, and the suspension method of the prosthesis.14,15 A finger or partial amputation had a significant influence on the physiological and psychological view of daily living in patients.2,4 Therefore, these patients had less QOL compared to healthy normal subjects. The findings of this study appear to support this information. Function of patients was affected by the level of amputation and number of it. Patients with less level of finger amputation in one finger may have less dysfunction compared to subjects with proximal amputation in some fingers. Prosthetic rehabilitation can improve function in the activity of daily living and potentially increase QOL in patients. 8 The results of this study demonstrated that using the prosthesis for six weeks increased patients QOL in physical, psychological, social, and environment domains compared to before using prosthesis. Improvement of suspension and providing aesthetic view of finger prosthesis may affect QOL in these patients.
A suitable suspension approach plus a user-friendly design of prosthesis is critical for the use of an aesthetic prosthesis. In this study, a new method of suspension based on simple application associated with use of biomedical silicone material was evaluated on large sample size of patients with finger amputation. The results of this comparative study showed that a 2 mm circumference reduction of residual limb can provide suspension with 0.79 ± 0.05 Nm strength, while in prosthesis with new method of suspension, this rate was 1.18 ± 0.10 Nm, which was sufficient to achieve a secure prosthetic fit at baseline. Although the mean of suspension strength reduced after wearing the prosthesis for 6 weeks for the two types of prosthesis in two patient groups, the reduction rate in the new prosthesis was less than the conventional prosthesis. The use of a central tunnel with 4 mm width and depth with length matching the distance between the end of the stump and the nail section provided additional and continued suspension in patients. Leow et al. 6 provided suspension of prosthesis for finger amputation and suggested that for a bony stump, a moderate model circumference reduction (5%-7%) was required to achieve a good prosthetic fit. Whilst in a stump with good soft tissue cover, a more aggressive model circumference reduction would be required (8%-9%). In another method, Nadoushan et al. provided some ridges on the inner socket of finger prosthesis and reported that suspension forces in a new design of finger prosthesis increased 53% compared to the conventional finger prosthesis, while in this study the new method increases suspension strength 67% compared to conventional prosthesis. The influence of the lengths of the stump to provide prosthesis suspension was not considered in this study. Further study in this field to compare the effect of using new method of suspension stumps with multilevel of amputation is required.
Satisfaction of patients in using prostheses was related to aesthetic nature of the prostheses, color, and fitting of them. 20 The results of this study demonstrated that good fitting and the patient’s skin-matched color-fabricated prosthesis provided good satisfaction in using the prosthesis, while according to improvement of suspension in constructed finger prosthesis, the new method of suspension had increased satisfaction rate compared to another prosthesis.
The authors acknowledge a number of limitations to this study and recognize that data were collected on patients only with amputations above the PIP joint. A larger sample size study with overall finger amputation in each level below metacarpophalangeal (MP) joint should be considered to evaluate the usage of prosthesis based on the new method of suspension and improve the generalizability of the results and the conclusions. In this study, the relationship between QOL and age of patients, level of amputation, and stump length was not analyzed. Additional study with different patients who present with multilevel amputation with age differences with considering other sociodemographic characteristics such as education, income, and employment status will be beneficial in this field.
Conclusion
According to QOL scores, patients with finger amputation had less QOL in physical, psychological, social impairment, and environmental health domains than the control group. Based on these findings, there is a clear need for improving the QOL in these patients. While using a finger prosthesis in patients with finger amputation demonstrated that this intervention can improve QOL compared to without a prosthesis, there was no significant difference between the two types of prosthesis on the improvement in QOL. However, wearing a prosthesis based on the new method of suspension had an effective role in providing suspension strength and increased satisfaction in patients with finger amputation compared to a conventional suspension method.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.