
Abstract
Background and aim:
In recent years, there has been an increased interest in recording high-quality electromyographic signals from within the sockets of lower-limb amputees. However, successful recording presents major challenges to both researchers and clinicians. This article details and compares four prototypical integrated socket–sensor designs used to record electromyographic signals from within the sockets of transfemoral amputees.
Technique:
Four prototypical socket–sensor configurations were constructed and tested on a single transfemoral amputee asked to perform sitting/standing, stair ascent/descent, and level ground walking. The number of large-amplitude motion artifacts generated using each prototype was quantified, the amount of skin irritation documented, and the comfort level of each assembly subjectively assessed by the amputee subject.
Discussion:
Of the four configurations tested, the combination of a suction socket with integrated wireless surface electrodes generated the lowest number of large-amplitude motion artifacts, the least visible skin irritation, and was judged to be most comfortable by the amputee subject.
Clinical relevance
The collection of high-quality electromyographic signals from an amputee’s residual limb while maximizing patient comfort holds substantial potential to enhance neuromuscular clinical assessment and as a method of intuitive control of powered lower-limb prostheses.
Background and aim
Electromyographic (EMG) signals recorded from the residual limbs of lower-limb amputees present a rich source of neuromuscular information that is potentially useful for both clinical evaluation1,2 and active prosthesis control.3–9 For example, in clinics, knowing the muscle activation patterns of residual limbs can assist in efficiently evaluating lower-limb amputee gait.1,2 More excitingly, recent research has reported promising results in the use of surface EMG signals from residual muscles for volitional control of motorized artificial legs.3–9 In this case, EMG signals are used as a neural control source, enabling lower-limb amputees to intuitively operate their prostheses based on user intent. For both applications, recording high-quality and reliable EMG signals is essential.
However, reliable collection of EMG signals from the residual limbs of lower-limb amputees presents a major practical challenge to researchers and clinicians. Inserting sensors into a prosthetic socket may create regions of high pressure and friction against the residual limb, leading to discomfort during ambulation and poor gait patterns. This problem is particularly acute in the case of transfemoral amputees, individuals whose prosthetic socket may completely cover their residual limb. Approaches that mitigate this pressure and friction may lead to loose socket suspension, resulting in pistoning of the residual limb in the socket during normal ambulation. This pistoning can cause severe motion artifacts in EMG recordings, resulting in the loss of EMG data due to inconsistent electrode contact. Successful engineering solutions must therefore achieve two goals in the design of interfaces between the residual limb, EMG sensors, and prosthetic socket: the consistent collection of high-quality EMG data from an amputee’s residual limb, and the maintenance of high levels of user comfort while wearing the prosthesis.
Several EMG socket–sensor interfaces have been reported for lower-limb prostheses.4,7–10 Some of these approaches used EMG electrodes that were directly mounted to the prosthesis socket; due to the relative motion between the prosthetic socket and residual limb during normal ambulation, these approaches resulted in EMG signals contaminated with motion artifacts. To resolve the problem, the latest studies have embedded EMG sensors into gel liners, adding an additional layer between the residual limb and socket wall. These gel liners are compliant with the shape of the residual limb, add additional compressive force to ensure secure electrode–skin contact, serve as a cushioning layer to reduce friction between the residual limb and prosthetic socket, and provide mechanisms for socket suspension. However, gel liners alone do not guarantee comfort; researchers must use additional approaches, such as modifying EMG electrode locations, to reduce pressure against the residual limb in order to avoid user discomfort.
Despite the increased number of reported studies using EMG signals recorded from the residual muscles of lower-limb amputees performing dynamic movements, to the authors’ knowledge, no studies have been conducted to date which systematically compare EMG signal quality collected from differing lower-limb socket–sensor integration approaches, nor has user comfort during the use of such integrated systems been directly investigated. Hence, this technical note details the construction of four prototypical integrated socket–sensor configurations designed in the authors’ lab within the last 5 years to surmount these challenges, and compares their performance in terms of both EMG signal quality and user comfort. This technical note may contribute significantly to the field of prosthetics by describing differing socket–sensor configurations and quantifying their performance, benefiting other groups interested in recording reliable EMG signals from the residual limbs of lower-limb amputees for both clinical evaluation and prosthesis technology development.
Technique
Socket–sensor configuration designs
Table 1 details the components of each socket–sensor configuration, which are pictured in Figure 1. The differing electrode integration methods used for each configuration are illustrated in Figure 2.
Prosthesis and EMG sensor components of each socket–sensor configuration.
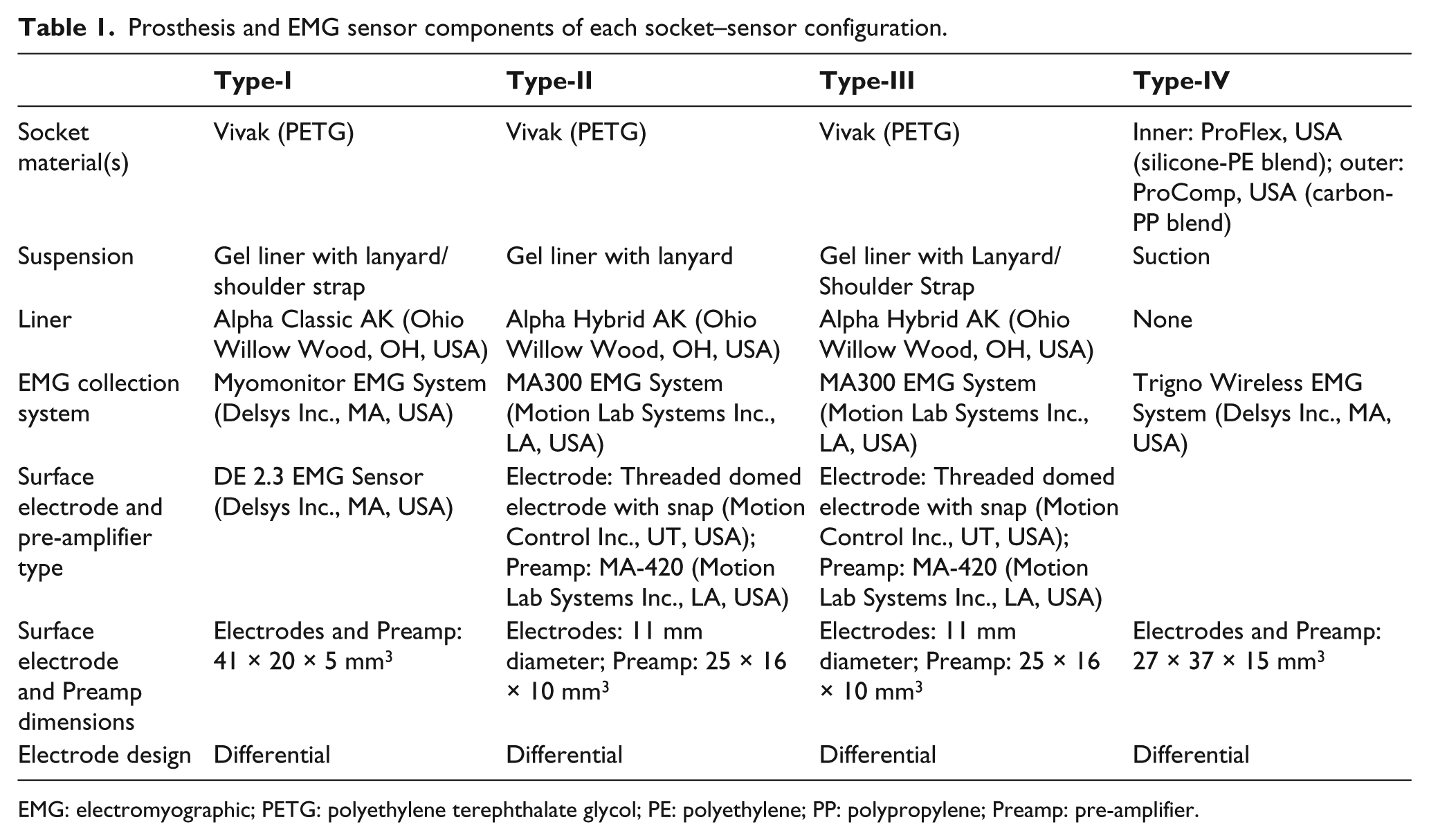
EMG: electromyographic; PETG: polyethylene terephthalate glycol; PE: polyethylene; PP: polypropylene; Preamp: pre-amplifier.
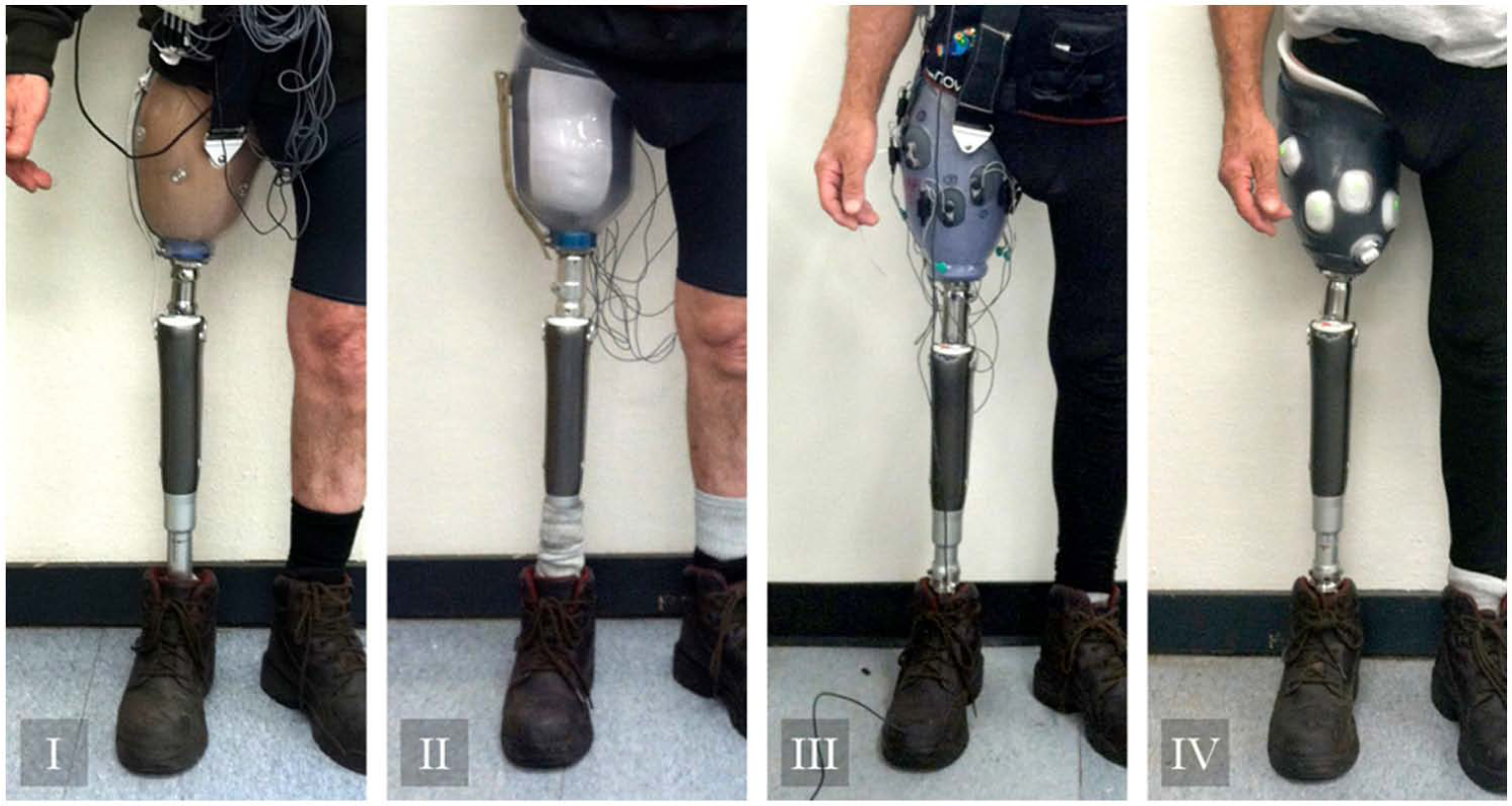
The four socket–sensor configurations while donned by the amputee subject.
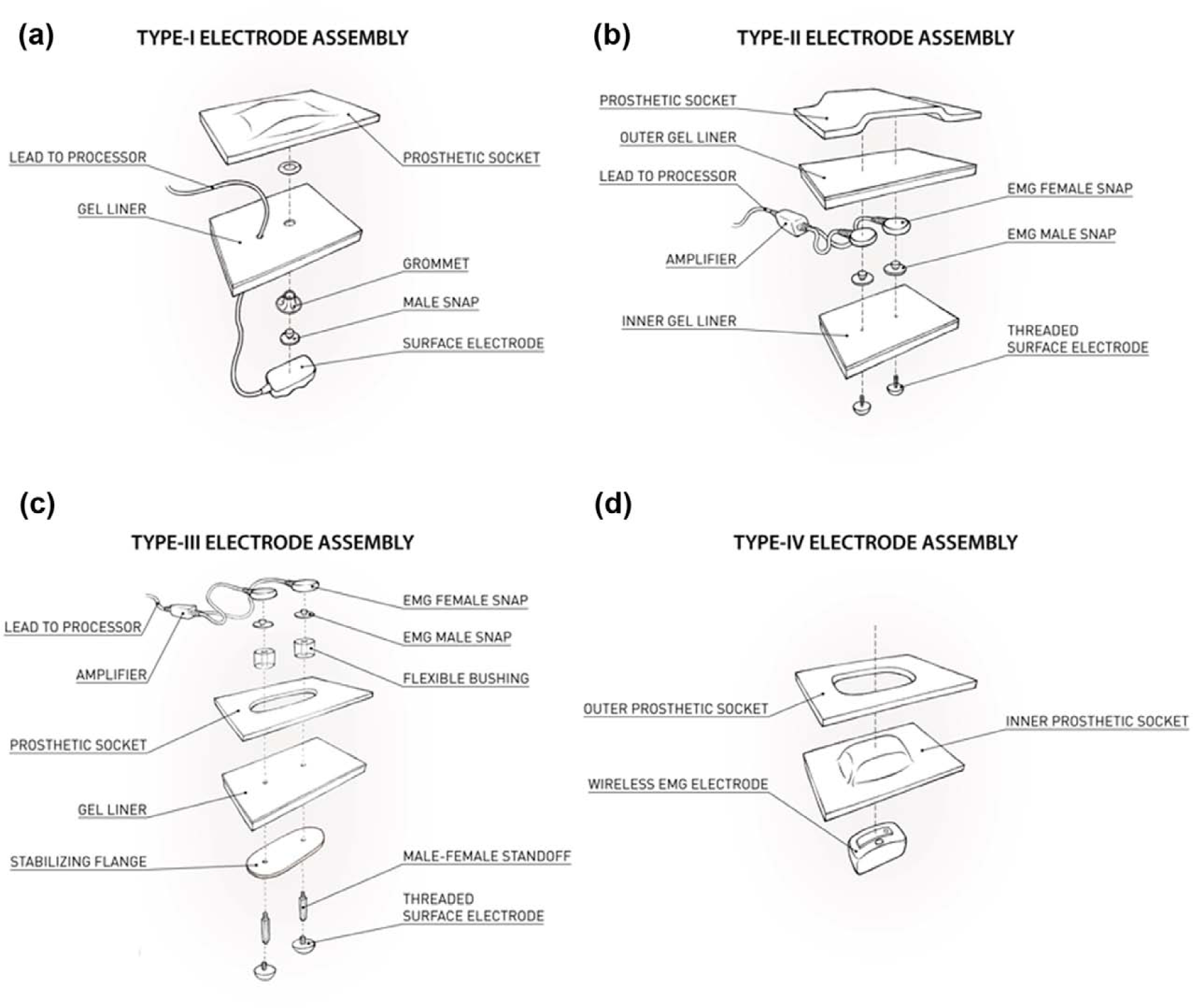
Schematic illustration of the four tested socket–sensor integration methods: (a) Type-I electrode assembly, (b) Type-II electrode assembly, (c) Type-III electrode assembly, and (d) Type-IV electrode assembly.
The first socket–sensor configuration (Type-I) used combined surface EMG electrodes and pre-amplifiers (DE 2.3; Delsys Inc., MA, USA). These electrodes were embedded within a modified gel liner (Alpha Classic AK; Ohio Willow Wood, OH, USA). The liner was rolled onto the subject’s residual limb before donning a custom-designed socket (Vivak PETG (polyethylene terephthalate glycol)). Molded reliefs in the socket wall were incorporated to minimize discomfort due to pressure against the subject’s residual limb from electrode contact.
The second configuration (Type-II) used snap-electrodes (Motion Control Inc., UT, USA) in combination with EMG pre-amplifiers (MA-420; Motion Lab Systems Inc., LA, USA). Two layers of gel liner were applied. Domed electrodes were embedded within the inner gel liner, while electrode snaps and pre-amplifiers were positioned between the inner and outer liner layers. The outer gel liner was rolled over the assembly to reduce the relative motion of snaps, pre-amplifiers, and lead wires. A socket (Vivak PETG), modified to accept the double-liner setup, was then donned by the amputee subject.
The third configuration (Type-III) also used snap-electrodes (Motion Control Inc.) in conjunction with EMG pre-amplifiers (MA-420; Motion Lab Systems Inc.). The electrodes were permanently mounted to a gel liner (Alpha Hybrid AK; Ohio Willow Wood) via polyethylene stabilizing flanges, allowing the electrodes to be maintained at a constant inter-electrode distance. Openings in the socket wall (Vivak PETG) allowed the electrodes to protrude out of the socket with the aim of reducing discomfort due to electrode pressure and to limit the effects of pistoning between socket and liner.
The fourth configuration (Type-IV) used wireless surface EMG electrodes with embedded pre-amplifiers (Trigno; Delsys Inc.). Wireless electrodes were placed in wells cast into the wall of a flexible interior suction socket (ProFlex, USA, USA; silicone–polyethylene (PE) blend) that did not require the use of a gel liner. A second, more rigid outer socket (ProComp, USA; carbon–polypropylene (PP) blend), provided added stability and was mounted to the prosthetic pylon.
Testing protocol
This study was conducted in accordance with Institutional Review Board (IRB) approval. In order to better assess the quality of EMG data gathered and user comfort level maintained by each of the four configurations, a new prototype of each design was constructed and tested using a single transfemoral amputee subject. The subject used a transfemoral ischial containment total contact suction socket (one-way expulsion valve) with a microprocessor prosthetic knee (C-Leg; Ottobock, Germany) as a standard prosthesis for daily use. The subject reviewed and signed informed consent documentation for study participation before any experimental procedure. Each socket–sensor configuration used the same number and placement of EMG electrodes. The electrode locations were determined based on the protocol reported in the authors’ previous study. 11
Five testing sessions were conducted in total: one to determine electrode locations used across the four socket–sensor configurations, and one session for each of the four described configurations. The configuration evaluation sessions were completed in a randomized order: Type-III, Type-IV, Type-II, and Type-I. The testing sessions were separated by a minimum of 4 days in order to reduce the confounding potential of fatigue and residual limb condition changes potentially resulting from preceding trials. Each experiment was conducted in a climate-controlled laboratory space for a duration of approximately 2 h.
During each experimental session, the subject used his own prosthetic knee (C-Leg; Ottobock) and donned one type of socket–sensor configuration. Each configuration was tested over the course of five trials in which the subject was asked to perform one of three task modes: sitting/standing transitions, stair ascent/descent, or level ground walking. For sitting/standing transitions, 10 repetitions were performed over 100 s. For stair ascent/descent, the subject ascended and descended five stairs every 30 s over two 120-s trials. For level ground walking, the subject walked back and forth 4 times along a 10-m track over two 120-s trials. EMG signals were recorded and sampled at 1000 Hz.
Data and analysis
Motion artifact is one of the major causes of EMG signal distortion. Large motion artifacts can saturate EMG recordings, which cannot be restored by any signal processing technique. Therefore, the number of motion artifacts that were large in magnitude was quantified as a method of evaluating the four socket–sensor configurations.
Raw EMG signals were first filtered using a 20–450 Hz band-pass filter (6th-order Butterworth filter) and rectified; these data were considered to consist primarily of EMG signal. Raw signals were again filtered using a 20 Hz low-pass filter and rectified; signal components lower than 20 Hz were considered to consist primarily of motion artifacts. 12 The largest amplitude EMG signal for each channel during each experimental session was determined; these values were defined as threshold voltages. Low-passed data were then analyzed in the time domain. A large-amplitude motion artifact was identified if the low-passed data were of greater magnitude than the determined threshold voltage for each channel. Since a single motion artifact can consist of both positive and negative deviations from baseline, successive motion artifacts were quantified only after a period of 200 ms had elapsed following the start of the preceding artifact to avoid over-counting. The number of motion artifacts per movement cycle for each channel was then calculated by dividing the total number of large-amplitude motion artifacts by either the number of gait cycles (for walking, stair ascent/descent trials) or the number of transitions (for sitting/standing trials). The calculated values of the seven channels were then averaged for each configuration and method of ambulation.
User comfort was evaluated using a questionnaire. Experimenters verbally prompted the subject for feedback regarding comfort for each task in each experimental session. In addition, the subject was asked to report aspects of prosthesis usability for the tested socket–sensor configuration at the end of each session. Responses to the questionnaire were used as the basis of comparison of comfort levels between the four configurations. Additionally, a set of photographs documenting the condition of the subject’s residual limb was taken prior to and within 5 min of socket doffing at the conclusion of each testing session.
Results
The number of motion artifacts per movement cycle per channel for each socket–sensor configuration across each ambulatory method is presented in Table 2. Through all three performed tasks, the Type-IV configuration produced the lowest number of motion artifacts per movement cycle per channel.
Number of large-amplitude motion artifacts recorded per movement cycle per channel and relative comfort level as reported by amputee subject of the four tested socket–sensor configurations.
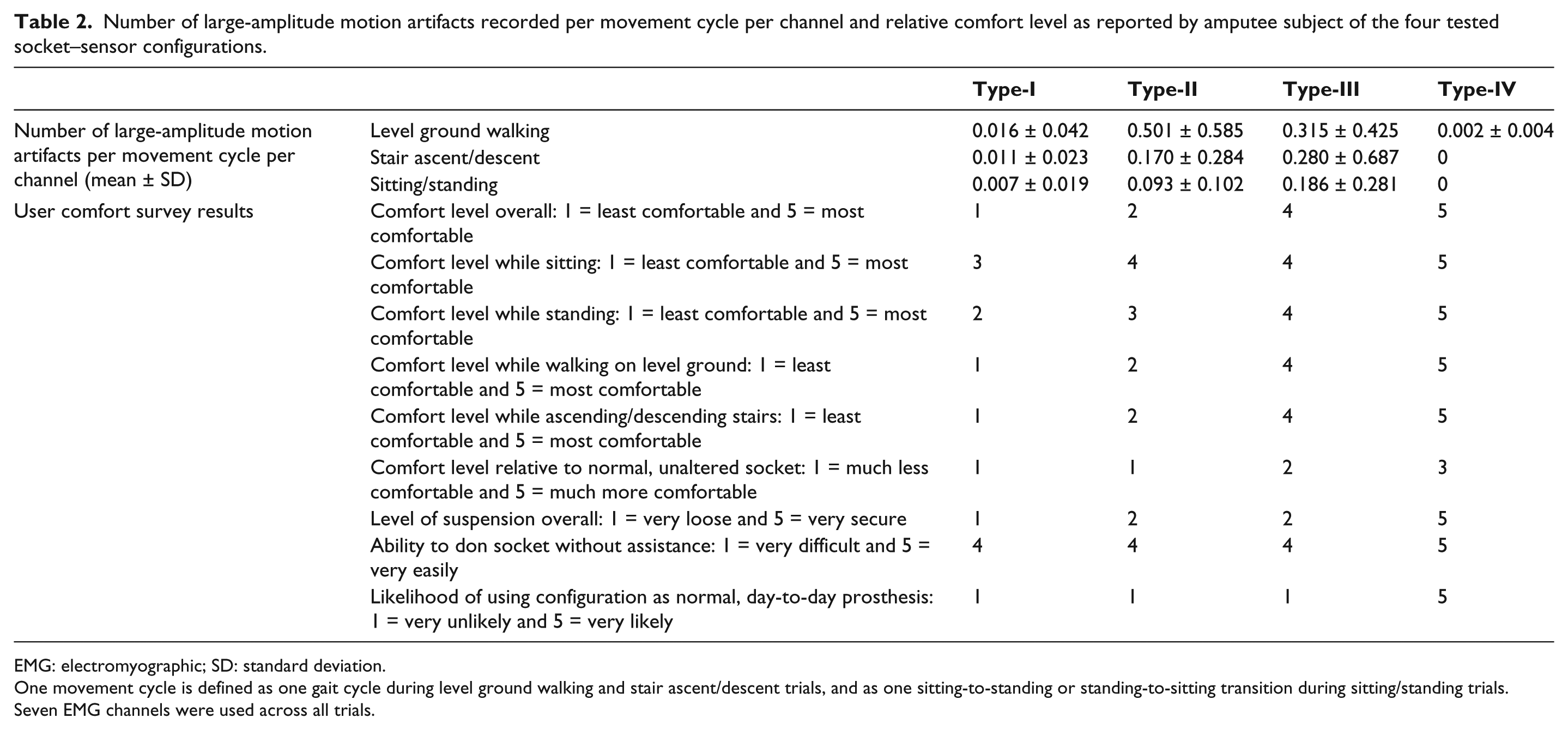
EMG: electromyographic; SD: standard deviation.
One movement cycle is defined as one gait cycle during level ground walking and stair ascent/descent trials, and as one sitting-to-standing or standing-to-sitting transition during sitting/standing trials. Seven EMG channels were used across all trials.
The results of the subjective evaluation of comfort level and usability of each configuration by the amputee subject are presented in Table 2. In all areas assessed, the Type-IV configuration was judged to be most comfortable by the amputee subject, while the Type-I configuration was assessed to be least comfortable in all circumstances.
Each of the four configurations tested generated markings on the skin of the amputee subject’s residual limb which persisted beyond socket doffing. The severity of the markings varied considerably between configurations, with Type-I generating the most severe and Type-IV generating the least severe as per the clinical opinion of the prosthetist associated with the study. Photographs documenting these observations are presented in Figure 3.

Effects of each socket–sensor configuration on the surface of the residual limb at the conclusion of each testing period.
Discussion
In this study, four EMG socket–sensor configurations were developed and compared. All four configurations can be fabricated using methods typically available to clinical prosthetic and orthotic practitioners. The results demonstrate that the Type-IV configuration produced both the lowest number of large-amplitude motion artifacts and the highest level of user comfort, two important conditions for successful EMG socket–sensor interface design. Additionally, the Type-IV configuration eliminated the requirement for wire management and maintenance, adding to the configuration’s practicality.
The authors speculate that the use of suction suspension, which may have maximized secure skin–electrode contact and limited the relative motion between the prosthetic socket and the patient’s residual limb, may be the primary driver of these results, both in terms of signal quality and user comfort. The wireless sensors utilized in the Type-IV configuration allowed for the fewest modifications to a normal, clinically available suction socket by eliminating the need for wires to exit the socket, either through perforations in the socket wall or by traveling along the length of the residual limb, which would potentially increase the likelihood of a loss of suction and the resulting loss of prosthesis suspension. These observations imply that the emerging wireless EMG sensor, which is already commercially available, is a promising technology for myoelectric prostheses. Drawbacks unique to wireless EMG sensors exist however. These include the need to re-charge batteries powering each sensor, a limiting factor that may render them insufficient for long-term daily use, and the potential for external sources of interference.
A recent study 8 has reported an approach in which myoelectric sensors were directly embedded into the wall of a transparent test socket and used to measure muscle activity. However, the study only recorded and evaluated EMG signals while the amputee subjects remained seated. A socket–sensor design using flexible, wired electrodes has also been designed by this group. 10 The electrodes are currently donned using a gel liner; further work is needed to integrate the electrodes within a suction socket. It is also noteworthy that the patented design uses a customized EMG wire connector at the bottom of the socket that may require additional engineering efforts to construct. Consequently, future work should further investigate these and similar socket–sensor integration methods, evaluating construction techniques, signal quality, and user comfort for configurations in which wired electrodes are directly embedded within the transfemoral suction socket and tested during ambulation.
The maintenance of high levels of both signal quality and user comfort is an important aspect of the successful integration of EMG sensor technology into the prostheses of lower-limb amputees. The short-term benefits of this successful integration extend to researchers and clinicians interested in characterizing the muscle activity of amputees’ residual limbs, while the potential long-term benefits of widely available, electromyographically controlled lower-limb prostheses extend to all present and future transtibial and transfemoral amputees. However, engineering efforts are still needed to make the reported configurations practical for daily prosthesis use.
Limitations
This study utilized a single amputee subject and one testing session each for the four described configurations. As a result, the data presented in this study should be considered preliminary. Additionally, the amputee subject’s familiarity with a specific socket type and suspension method for daily use may affect the subject’s perception of comfort. The authors hope to mitigate this possibility by including more amputee subjects during future configuration evaluations.
The electrode positions used for each of the four configurations followed the same positioning scheme, minimizing differences in signal quality due to electrode position variability. However, exactly identical electrode positioning could not be rigorously maintained between trials.
Additionally, it is noteworthy that the three EMG electrode systems employed differing pre-amplification and hardware filtering methods, also affecting the overall quality of EMG signals during data collection. However, the focus of this evaluation was not on a direct comparison of the differing commercial EMG systems, which have been successfully utilized by researchers investigating both biomechanical assessment and the design and engineering of rehabilitative devices.13–18 Hence, instead of quantifying overall signal quality, such as signal-to-noise ratio, the authors chose the number of large-magnitude motion artifacts, which are difficult, if not impossible, to eliminate using all commercially available EMG electrodes and systems, as the evaluative metric. As a consequence, the authors believed that whether or not large-magnitude motion artifacts were present in raw EMG recordings was more pertinent to the stability of the socket–sensor integration method, method of socket construction, or prosthesis suspension than the electronic configuration of EMG electrodes and systems. However, even by using the number of large-magnitude motion artifacts as the evaluation metric, the authors acknowledge that the effects of socket design and EMG system cannot be fully separated in individual configurations. Therefore, the authors recommend interested research and clinical groups duplicate all the aspects (i.e., both socket–sensor integration design and EMG system) of the Type-IV configuration, if affordable, for reliable EMG recording from the residual lower limb within the socket.
Key Points
Signal quality and user comfort are important considerations for the successful integration of EMG sensors with lower-limb prostheses.
The design and comparison of four EMG socket–sensor configurations was reported.
Of the four configurations tested, the combination of wireless electrodes and a suction socket (Type-IV) generated the fewest large-amplitude motion artifacts during all three methods of ambulation.
The Type-IV configuration produced the least visible deformation of the skin of the residual limb and was subjectively assessed by the amputee subject to be most comfortable during use.
Footnotes
Acknowledgements
The authors would like to thank Ming Liu, Lin Du, Ding Wang, Doug Wilson, and Desiree Roberts for their contributions.
Conflict of interst
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Science Foundation (grant numbers 0931820 and 1149385), the United States Department of Defense (grant number W81XWH-09-2-0020),the National Institutes of Health (grant number RHD064968A), and the National Institute on Disability and Rehabilitation Research (grant number H133G120165).