
Abstract
Background:
Rheumatoid arthritis is a chronic inflammatory joint disease which affects the joints and soft tissues of the foot and ankle. Rocker shoes may be prescribed for the symptomatic foot in rheumatoid arthritis; however, there is a limited evidence base to support the use of rocker shoes in these patients.
Objectives:
The aim of this study was to evaluate the effectiveness of heel-to-toe rocker shoes on pain, disability, and activity limitation in patients with rheumatoid arthritis.
Study design:
Clinical trial.
Methods:
Seventeen female patients with rheumatoid arthritis of 1 year or more duration, disease activity score of less than 2.6, and foot and ankle pain were recruited. Heel-to-toe rocker shoe was made according to each patient’s foot size. All the patients were evaluated immediately, 7 and 30 days after their first visit. Foot Function Index values were recorded at each appointment.
Results:
With the use of rocker shoes, Foot Function Index values decreased in all subscales. This reduction was noted in the first visit and was maintained throughout the trials.
Conclusion:
Rocker shoe can improve pain, disability, and activity limitation in patients with rheumatoid foot pain. All the subjects reported improved comfort levels.
Clinical relevance
The results of this study showed that high-top, heel-to-toe rocker shoe with wide toe box was effective at reducing foot and ankle pain. It was also regarded as comfortable and acceptable footwear by the patients with rheumatoid foot problems.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory articular disease 1 that affects about 0.3%–1.5% of people. 2 Foot problems are one of the major problems in the RA patients. 3 About 16% of the RA patients may have foot joints involvement, 4 which will increase to 90% with the progress of disease. 5 Common foot deformities in the RA patients are hallux valgus, lesser toe deformities (hammer toe and claw toe), subluxation of metatarsophalangeal (MTP) joints, 6 valgus heel deformity, and flat foot. 7 These foot deformities increase plantar pressure and cause musculoskeletal foot pain in the RA patients. 8 Foot pain is major problem in about one-third of the RA patients, especially in forefoot, rear foot, and ankle. 9 Foot pain is said to have negative effect on functional performance that might in turn drastically change quality of life. 10
The goals of foot care in the patients with RA are to decrease and control pain, to maintain functional activity, and to improve the quality of life. 11 There is some evidence that therapeutic footwear is a beneficial intervention for relief of foot pain, improvement in foot function and health, and increase in patient’s mobility. 12 The rocker soles (RSs) are the most commonly prescribed external shoe modifications. 13 As its name suggests, the basic function of RS is to literally rock the foot from heel strike to toe-off without bending the shoe. 14 RSs are used in the treatment of conditions requiring limitation of motion where pain exists in the foot and ankle to redistribute pressure. 15 There are various types of rockers such as toe-only rocker, double rocker, heel-to-toe rocker, and negative heel rocker. 14 Theoretical consideration and initial experimental results indicated that a heel-to-toe RS (unstable shoe) design may be beneficial for movement and reduction of pain and discomfort in joints. 16 The purpose of this study was to evaluate the effect of heel-to-toe rocker shoe on pain, disability, and activity limitation in RA patients immediately, 7 and 30 days after their first visit. It was hypothesized that high-top shoe with wide toe box and heel-to-toe RS would decrease pain, disability, and activity limitation in RA patients.
Methods
Subjects
Seventeen female patients with RA who met the 1987 American College of Rheumatology criteria 17 for RA were examined. Inclusion criteria were disease longer than 1 year, nonactive disease (defined as a disease activity score of 28 (DAS 28) of <2.6), and foot and ankle pain. Exclusion criteria included the following: (1) previous lower limb joint surgery, (2) skin ulcers or dermatitis, (3) rigidly fixed foot deformities (i.e. rigid flat foot or Pes cavus), (4) central or peripheral nervous system disorder, (5) intra-articular steroid injection at least 3 weeks before the first visit, and (6) ankle sprain or strain in last 3 months prior to the first visit.
The ethical committee of Faculty of Rehabilitation Sciences, Iran University of Medical Sciences (IUMS), reviewed and approved the study procedures, and informed written agreement was received from each subject.
Footwear and RS
High-top shoes extended above the lateral malleoli for decreased ankle motion. The toe box was wide to allow extra room for the deformed toes. Velcro closures were chosen as RA patient mostly have hand problem (Figure 1(a)). Furthermore, heel-to-toe RS was added to the basic shoe (Figure 1(b)). 18
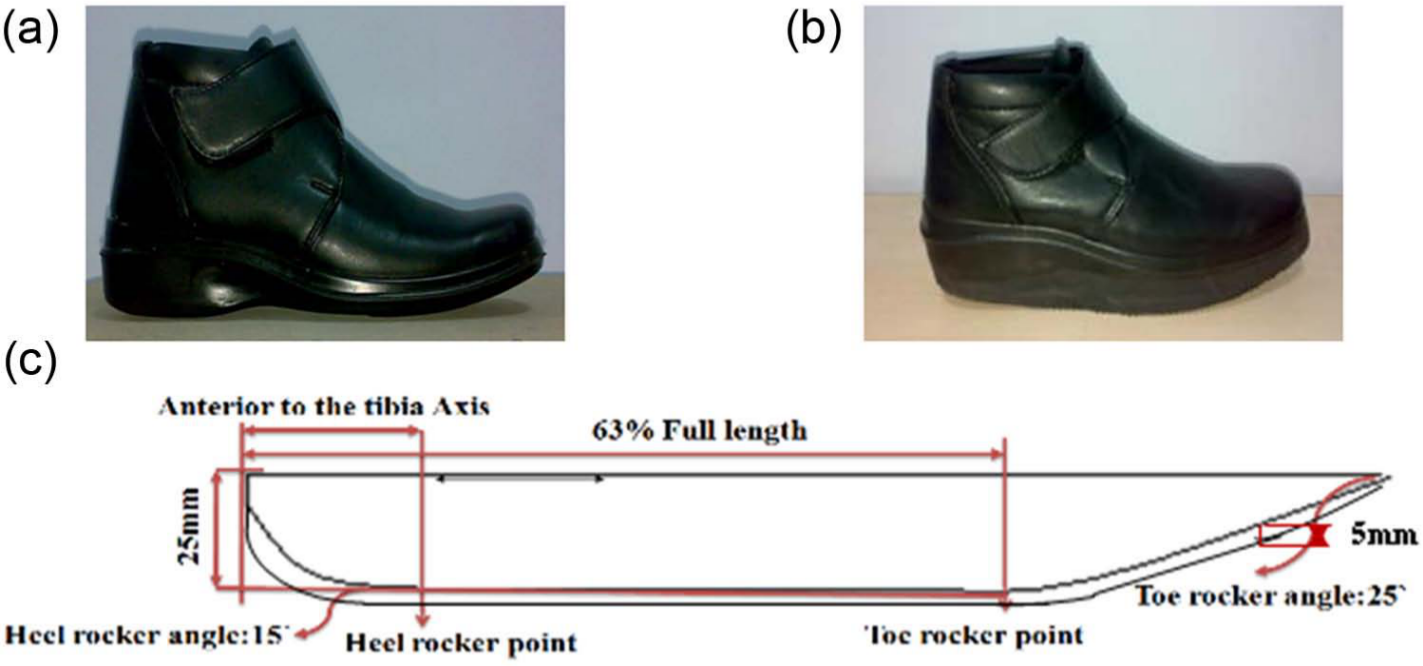
The shoe and rocker sole used in this study: (a) basic shoe, (b) rocker shoe, and (c) structure of rocker sole.
Heel-to-toe RS was made of ethylene vinyl acetate (EVA)of 25 mm thickness with standard hardness (shore-A 30-40) for midsole and 5 mm thickness hard texture rubber (shore-A 50-60) for outsole. Thick, soft midsoles are comfortable, but it can decrease stability, impair proprioception, and increase ankle movement. Thin, hard midsoles are uncomfortable but more stable. 19 The toe rocker started at 63% of the total shoe length (about 1 cm distal to the metatarsal head) for maximal forefoot plantar pressure reduction, 20 and the apex of the heel rocker was proximal to medial malleolus (proximal to tibia). 21 If the heel rocker was placed distal to the medial malleoli, ground reaction force (GRF) crossed distal to the knee and caused flexion moment in early stance phase. The heel rocker proximal to the medial malleolus caused GRF to cross proximal to the knee and increased knee extension moment at late stance phase. However, if heel rocker was proximal to the medial malleolus, improper knee extension and flexion moment in stance phase was reduced. 21 The toe rocker angle was 25° because the first MTP joint pressure was the lowest with a 25° angle rocker 22 and 15°heel rocker. The reason was that increased ankle range of motion 23 and compensatory effect of high-top shoe decreased ankle motion (Figure 1(c)).
Procedures
At the first visit, age, sex, disease duration, DAS 28, body height, and weight were recorded. Foot deformities, foot and ankle range of motion, and skin callosities were examined by rheumatologist.
Pain location was divided into three regions: forefoot, rear foot, and ankle. Rheumatologist determined pain location through physical examination and patients’ subjective reports.
The RS was custom fabricated for each patient based on the foot size by an expert shoe technician. Afterward, each patient wore the shoe and walked for 5 min to adapt to RS. 24 If patients expressed that the shoe was comfortable, they were asked to fill the Foot Function Index (FFI) questionnaire.
FFI was used to define foot pain and disability. The FFI was expanded to measure the impact of foot problem on function in terms of pain, disability, and activity limitation by Budiman-Mak et al. 25 The FFI is a self-administered questionnaire including 23 items divided into three subscales. All the responses are based on the visual analogue scale (VAS). The pain subscale consists of nine items that measure the level of foot pain. The disability subscale consists of nine items for determining the level of difficulty in performing daily activity owing to foot problem. The activity limitation subscale consists of five items for determining the level of activity limitation owing to foot problem. Subscale scores range from 0 to 10, with higher scores informing greater impairment. If a subject did not play an activity, such as running or did not use an assistive device, this section was excluded from the total. 25
After the first evaluation, other appointments were scheduled at 7- and 30-day intervals to check the footwear and perform necessary adjustments.24,26 In each session, the patients answer the FFI questionnaire. They were also asked to report the daily wear time (hours per day).
Statistical analysis
To analyze the impact of rocker shoe on the FFI values during the study, and to study the efficacy of pain location on the FFI results, analysis of variance for repeated measures was used (P < 0.05). All the analyses were performed using SPSS for Windows version 13.0 (SPSS Inc., Chicago, IL). Alpha levels were set at 0.05 for all the tests.
Results
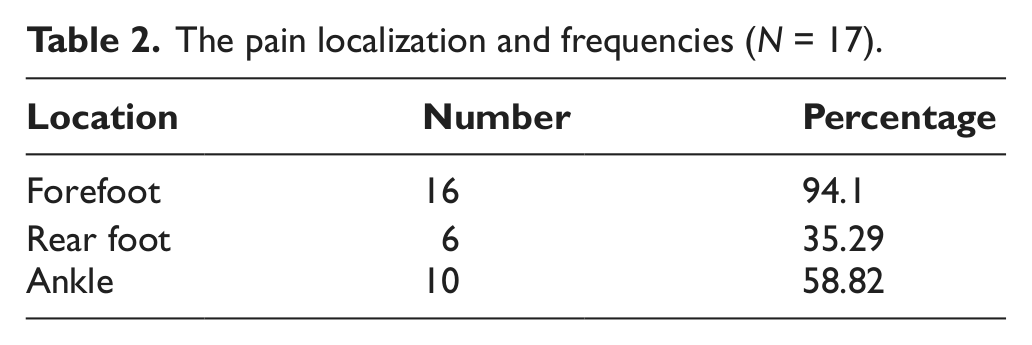
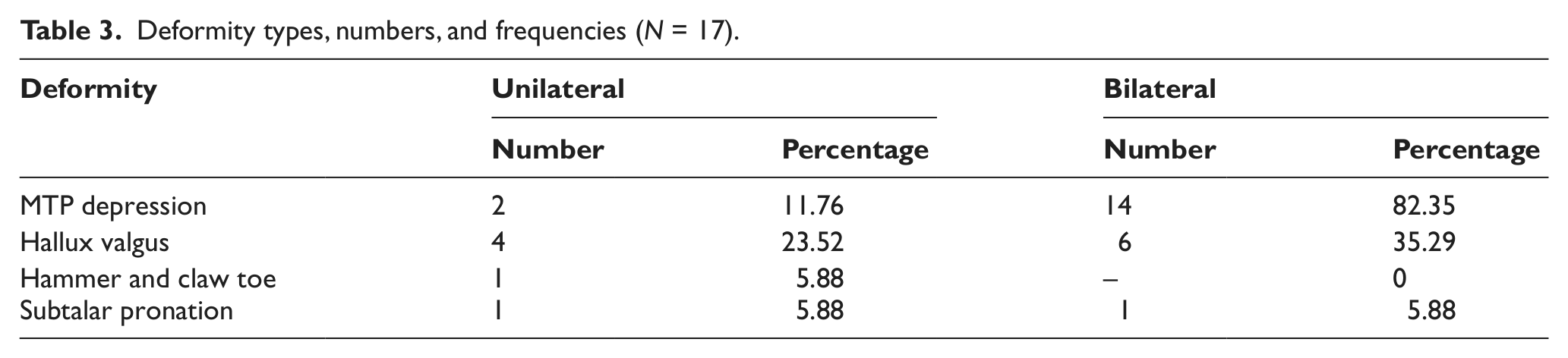
Eighteen patients were recruited at the beginning. After 7 days, one patient withdrew from the study as she did not use the rocker shoe (Table 1). The pain localization and percentage of frequencies are shown in Table 2, and deformity types, numbers, and percentage of frequencies are shown in Table 3.
Demographic characteristics of the subjects (N = 17).
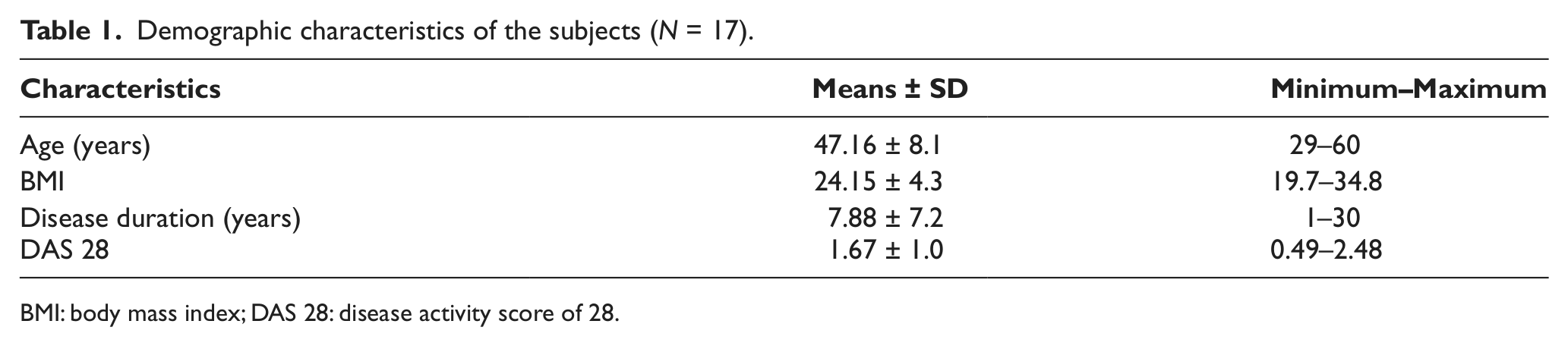
BMI: body mass index; DAS 28: disease activity score of 28.
The pain localization and frequencies (N = 17).
Deformity types, numbers, and frequencies (N = 17).
In comparison of result variables of pre- and post-intervention, significant improvements were seen in pain, disability, activity limitation, and total scores in 30-day follow-up (P < 0.05). All the consequence variables were analyzed according to the anatomical location of foot and ankle pain (forefoot, rear foot, and ankle). Table 4 shows the mean amount of pain, disability, activity limitation, and FFI total scores for all the patients.
The comparison of FFI scores.
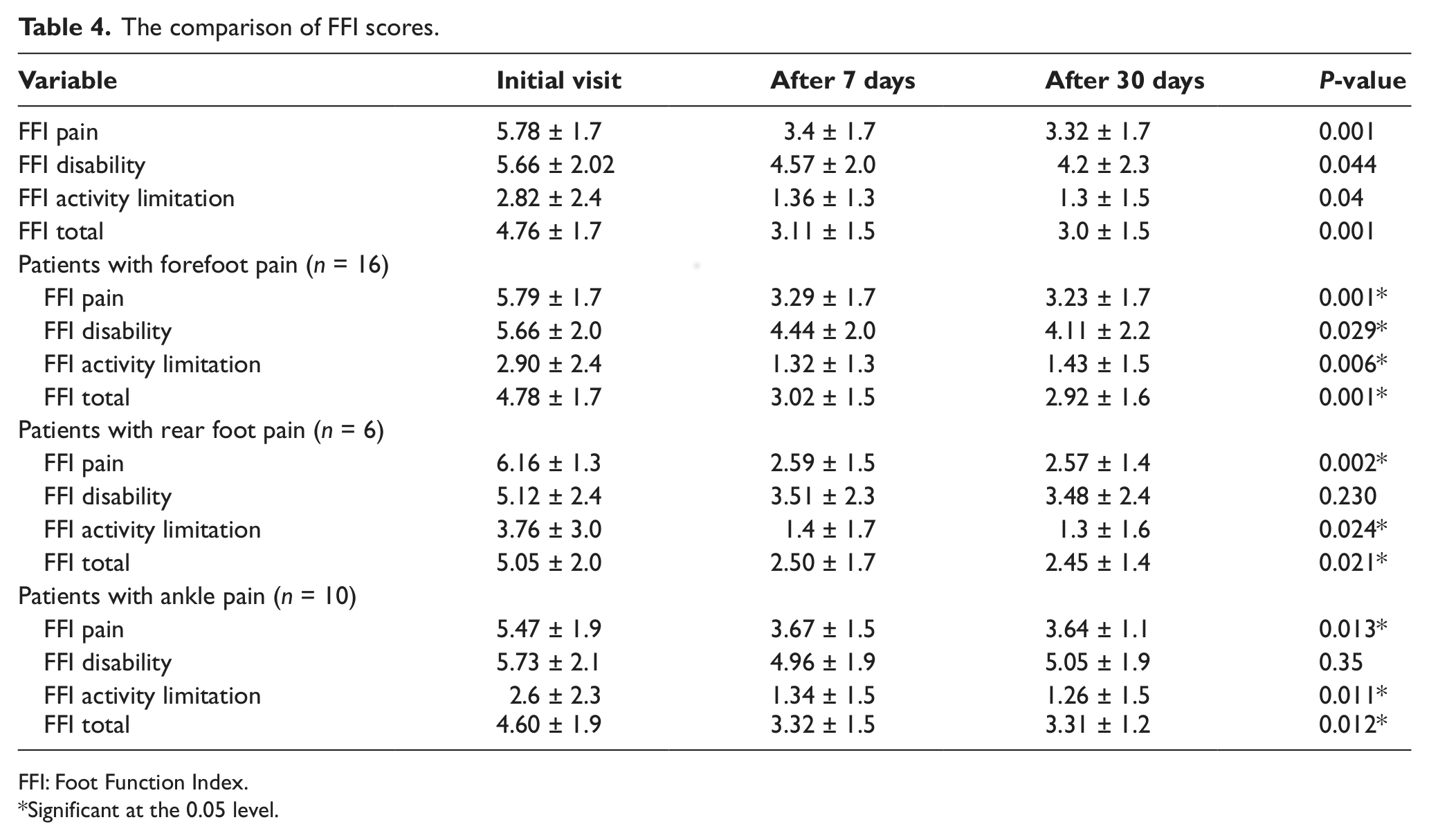
FFI: Foot Function Index.
Significant at the 0.05 level.
The group with forefoot pain demonstrated significant improvement (P < 0.001) in pain, disability, activity limitation, and total scores from baseline to 30 days (Table 4). In the group with rear foot pain and ankle pain, the results showed significant improvement (P < 0.05) in terms of pain, activity limitation, and FFI total scores after 30 days, but there was no significant improvement (P > 0.05) in disability score (Table 4). The statistical analysis of all the patients revealed an early decline in pain, disability, activity limitation, and total scores after 7 days of wearing the rocker shoe, and this improvement was sustained after 30 days of follow-up.
Discussion
According to the hypothesis of this study, use of high-top rocker shoes with wide toe box significantly decreased pain, disability, and activity limitation and improved comfort in the RA patient with foot problems after 7 and 30 days of follow-up.
Rocker shoes are generally prescribed for the conservative treatment of the foot and ankle problems in RA patients.18,27 A number of previous investigators have examined the effects of RS on plantar pressure, 28 electromyography, 29 gait kinetics, and kinematics22,30,31 on diabetic 32 or normal individuals.28,30 However, only a limited number of studies have been performed on the effect of RS on pain, disability, and activity limitation in RA patients with foot and ankle pain.33,34 Our findings agree with those of the previous studies on the effectiveness of orthopedic footwear on foot and ankle pain, disability, and activity limitation.33,34 Cho et al. 33 compared custom-made semirigid insole and a ready-made 6-mm simple soft insole in extra-depth, toe-only rocker shoe with bare foot in RA patients. The results showed significant decrease in VAS and total FFI scores in both groups compared to the bare foot. Kavlak et al. 34 reported that appropriate foot orthoses with proper shoe correction such as rocker bar, RS, and wedge can improve function and decrease pain in RA patients with foot problems.
Pain is a major symptom of RA and is the leading reason for seeking the medical care. 26 Forefoot plantar pressure is 2–3 times higher in RA patients, and increased foot pressure leads to musculoskeletal pain in RA patients. 8 RSs are designed to relieve high-pressure areas, reduce shock and shear to the foot, and limit painful motion. 15 Research has shown that RS decreased plantar pressure in the forefoot. 28 Praet and Louwerens 32 showed that high-top shoe with RS reduced ankle joint range of motion, increased affective contact area, and decreased pressure under the forefoot. However, in this study, we could not measure the plantar pressure; the results showed significant decrease in pain in this population, which is consistent with the above-mentioned studies.
With further pain and deformity, custom-made footwear may be required to improve ambulation and reduce the need for surgery in RA patients. The compliance with custom-made shoes is low as they fail to meet expectations of comfort, cosmetic, and function 35 for such a high cost. Instead, RA patients tend to make their own modifications to their footwear or find shoes that provide sufficient pain relief to enable them to ambulate. 36 Williams et al. 12 found that patients prefer to wear own shoes as they feel comfortable, fit, with appropriate appearance and long-term function. Both researchers and clinicians have supported appropriate footwear as the most important part of nonoperative care in RA patients.27,37,38 Park and Craxford 39 found significant pain decrease with surgical shoes and total contact plastazote compared with conservative treatments. In general, the findings of this study indicated that RA patients with foot and ankle pain intended to wear high-top RS with wide toe box as it could decrease their foot pain and improve their activities.
Some limitations of this study should be noted. The study population was small for the analysis of patient subgroups because we recruited patients with stable disease who had not received injection and had no skin ulceration. Our results were also limited by a short follow-up period. Prospective, longitudinal evaluation of various RSs and footwear interventions on the plantar pressure, kinematics, and time of use in a large group of RA patients is needed to determine more accurate influence of rocker shoes.
Conclusion
The results of this study showed that high-top, heel-to-toe rocker shoe with wide toe box might be effective in decreasing the foot and ankle pain, disability, and activity limitation. Further studies are needed to define the long-term effect of rocker shoes on plantar pressure, kinematics, kinetics, and pain relief in RA patients.
Footnotes
Acknowledgements
We would like to thank Mr. Haseli for the fabrication of rocker shoes, and Dr Frank bell for the critical review of this article. All the experimental tests were conducted at RRC IUMS Biomechanics Lab.
Declaration of conflicting interests
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.