
Abstract
Background:
Degenerative joint disease is not uncommon in amputees and reaches the orthopedic surgeon when all other conservative methods to manage these patients have failed. Several case reports describing hip and knee arthroplasties in patients with hip and knee joint diseases or fractures with the distal part amputated, either in the contralateral or ipsilateral limb, exist in literature.
Objective:
This article focuses only on total knee and total hip arthroplasty in amputees who have had severe osteoarthritis of the ipsilateral hip and knee joints.
Study design:
Literature review.
Method:
Literature search in database and summary of all the cases.
Results:
All narratives indicate positive outcomes with improvement in physical function and quality of life.
Conclusion:
The reports suggest that slight modifications in surgical procedure and in the rehabilitation protocol as compared to other patients with joint arthroplasties can alleviate pain and make such patients ambulatory and gain maximum range of motion. Therefore, it appears that careful preoperative evaluation and planning tailored to suit individual cases maximizes postoperative good end results beneficial to the patients regardless of age or cause of osteoarthritis.
Introduction
Lower-extremity amputation is one of the oldest known surgically performed procedures. Amputation is still often viewed only as a failure of treatment; however, amputation can be the treatment of choice for severe trauma, chronic vascular disease, congenital limb deficiency, and tumors. 1 Lower limb amputations are common procedures with about 130,000 per year in the United States, with 80% linked to vascular disease. Multiple secondary physical conditions, including osteoarthritis (OA), osteoporosis, back pain, and other musculoskeletal problems, have been observed in long-term survivors. 1
This article is based on a literature search that focused on knee and hip joint arthroplasties among lower limb amputees. Our search strategy included the PubMed and Google Scholar databases only. Search terms were very broad and included “ipsilateral knee joint arthroplasty in amputees” and “ipsilateral hip joint arthroplasty in amputees.” A total of four articles describing ipsilateral knee arthroplasty were located. One article (Prickett and Scanlon 2 ) described total hip and knee joint arthroplasties. Seven articles with ipsilateral total hip arthroplasties (THAs) conducted on knee amputees were located.
To our knowledge, there was no article that described total knee and hip joint arthroplasties and outcomes on surgeries conducted only on the ipsilateral limb of amputees placed together in a single report. Hence, in our article, we present what is known about the experiences of surgeons who have conducted knee and hip joint arthroplasties on the ipsilateral above- or below-knee amputations.
Association between lower limb amputation and OA
The association between lower limb amputation and OA is well established. The degradation of articular cartilage and remodeling of subchondral bone results in deterioration of joint function. Up to 90% of people with amputation wear a prosthesis at least 7 hours a day to aid mobility and perform everyday activities. 1 An “improper fit” alters forces on the skeletal and soft tissues of the intact limb that can lead to degenerative conditions. In addition, the contralateral limb also gets predisposed to degenerative arthritis, and so it is not uncommon to find the contralateral limb affected with OA more than the amputated limb. A lot of surgeons have examined OA of hip and knees in war veteran amputees. Amputees tended to have a higher incidence of patellofemoral osteoarthritic degeneration on their intact limb than people without amputation, with 41% OA with transtibial amputation and 63% with transfemoral amputation. 3 This was attributed to gait asymmetry and an increased load on the intact limb and to increased weight gain due to sedentary lifestyle increasing the risk of OA. 4 An earlier report that analyzed data from a radiographic analysis of 44 British male Second World War veterans found that the incidence of OA in the amputated side was 61% compared to 23% on the non-amputated side (based on Kellgren and Lawrence grade of >2). 5 Using a minimum joint space threshold of below 2.5 mm, the incidence was 55% on the amputation side of the limb versus 18% on the non-amputated side. A threefold increased risk of OA was observed with above-knee compared to a below-knee amputation. The findings revealed a 3- to 6-fold increase in OA of both the amputated and intact hips compared with age-matched veterans without amputation, and a threefold increase of OA was found for transfemoral compared with transtibial amputation.
Arthroplasties in amputated limbs
Total knee arthroplasty
Total knee arthroplasty (TKA) is a successful, safe, and cost-effective treatment that alleviates pain in addition to improving function, thereby improving the quality of life in patients with debilitating arthritis. 6 According to a report from the Agency for Healthcare Research and Quality, more than 200,000 knee replacements are performed each year in the United States. 7
Case reports of TKAs in patients with ipsilateral amputation have been described in the past few decades. Using modifications to the surgical techniques and rehabilitation program, as described by the authors, all the cases seem to have had positive outcomes with respect to range of movement (ROM) and mobility. Four such cases are described, and each had a variation in their management approach.
An account of a right transtibial amputation for chronic osteomyelitis was described, in which TKA was performed with excellent outcome for OA in the same limb. 8 The patient had developed disabling OA of his right amputated limb, and cemented TKA was offered as a final option. The history pointed to posttraumatic complications, and as a result had to undergo right transtibial amputation as a young adult aged 23 years. For nearly half a century, he had no complications despite having to change the type of prosthesis. As symptoms of OA began, and with decreased walking distances, the patient agreed for a TKA. The case report offers no specifics regarding surgical approach used, but describes the patient’s post TKA rehabilitation in fair detail. The surgeons however concluded that the length of the patient’s preoperative residual limb should be more than 10–12 cm to hold the tibia1 component of the total knee prosthesis when TKA is being considered among ipsilateral amputees. Preoperatively, the patient was prepared with a patellar tendon-bearing total contact socket, endoskeleton shank, SACH (solid ankle cushion heel) foot, and supracondylar strap with waist belt suspension temporary prosthesis and stockings to combat postoperative edema. Immediately after TKA, the patient was placed in a modified knee orthosis locked in full extension to avoid the formation of a flexion contracture that was used during his rest periods. Rehabilitation was continued with physical therapy that included quadriceps and gluteal isometric strengthening, active-assisted straight leg raises, and short-arc leg extension exercises. There were no immediate postoperative complications, and on day 4, weight-bearing walking was commenced. In less than 2 weeks, he had obtained full knee extension and 80° active-assisted knee flexion. He was discharged on postoperative day 16, with an ambulation distance of 225 feet with his prosthesis and axillary crutches. With continued physiotherapy, mobility of the patient increased despite one episode of infection that subsided with a course of antibiotics. The final prosthesis was fitted at 6 weeks postoperatively. It was a “patellar tendon-bearing total contact socket with a supracondylar strap and waist belt suspension, an endoskeleta1 shank, and a Seattle Light foot.” By this time, he had achieved full active extension and 105° flexion and was able to walk unassisted within his house.
Another case achieving similar favorable outcome was that of a 75-year-old woman who developed worsening OA of the ipsilateral knee following a below-knee amputation for chronic venous disease. 9 A TKA had been performed in the contralateral limb 4 years earlier. A TKA performed in the amputated limb helped in successfully mobilizing her and alleviating her pain. In this particular case, intraoperatively, the knee was maintained in full flexion with the help of a sterile polystyrene packaging box. Despite limited insertion, an intramedullary guide rod was utilized to align the tibial cut. This patient had had only 12.5 cm of proximal tibia, although intramedullary alignment is more accurate with longer stumps. As per routine total knee replacement (TKR), physiotherapy was commenced on the first postoperative day with routine exercises. On the fifth postoperative day, the patient had achieved between 15° and 90° of flexion and discharged wheelchair-free, but with continuing physical therapy. The patient was followed up for 8 months and found to be pain-free, with the Knee Society Score having improved from 53 to 85, the function score increased from 0 to 40, ROM of her right knee being 10°–115° of flexion. The authors were of the opinion that rather than using a temporary prosthesis for immediate weight bearing postoperatively described earlier, 8 a delayed limb fitting can be organized once the wound has healed and the postoperative edema has settled.
A third case that has been described is that of a man in his fourth decade of life who had sustained an open tibial fracture that subsequently got infected in the non-united tibia and had to undergo a below-knee amputation. 10 He developed arthritis with ROM of 0°–123° for which he underwent a left posterior-stabilized cemented TKA. A modified, sterilized, plaster prosthesis, according to the stump, was used intraoperatively to support the amputation stump with the rod aligned at exactly a right angle to the socket. After the arthrotomy and patellar eversion, the sterilized prosthesis was placed on the distal stump, and the knee was fully flexed with the prosthesis supporting the stump. An extramedullary jig was aligned to the prosthesis 10 mm off the high side for the tibial cut. The tibial length in this patient was 17 cm. Postoperatively, physical therapy followed with the patient reaching 10°–62° of flexion by sixth day (postoperatively). Weight bearing in the adjusted prosthesis was done at 3 weeks only after wound healing, and the Knee Society Score improved from 44 to 80, and function score had improved from 10 to 40.
All these cases suggest that by modifications to the surgical technique depending on the tibial length available and by changes in existing rehabilitation protocols as compared to normal TKAs, a TKR can salvage degenerative OA limbs in below-knee amputees. As is evident from the first two cases, in their approach to the tibial cut, a proximal tibial stump between 10 and 12.5 cm can provide optimal tibial alignment. In shorter stumps, intramedullary guide may be of help. Furthermore, a sterilized custom prosthesis in the third case report stabilizes limb positioning and may prevent infection. Postoperative rehabilitation, although to be taken immediately after surgery, can vary from patient to patient and institute to institute. Precaution is advised for postoperative edema. While a temporary prosthesis may be used, positive outcomes with respect to ambulation and ROM can be done by later placement of prosthesis once postoperative edema has fully resolved. Complete weight bearing during rehabilitation is best done after the wound has completely healed. A similar change in rehabilitation protocol from normal TKA was described much earlier and deserves mention here. No surgical details were provided for a TKA in the left amputated knee in a patient whose preoperative ROM was 10° extension and 105° flexion at the knee joint. 2 Postoperatively, the use of a posterior splint was found useful, with regular physical therapy for muscle strengthening during the day. Exercises with a lightweight suspension stump prosthesis was started by 3 weeks postoperatively, and the patient was discharged using a cane. His ROM finally was a healthy 90° flexion and 5° extension at the left knee joint. A brief summary of the cases described above is detailed in Table 1 (placed in chronological order).
Brief summary of total knee arthroplasties (TKAs) done in ipsilateral below-knee amputees (placed in chronological order).
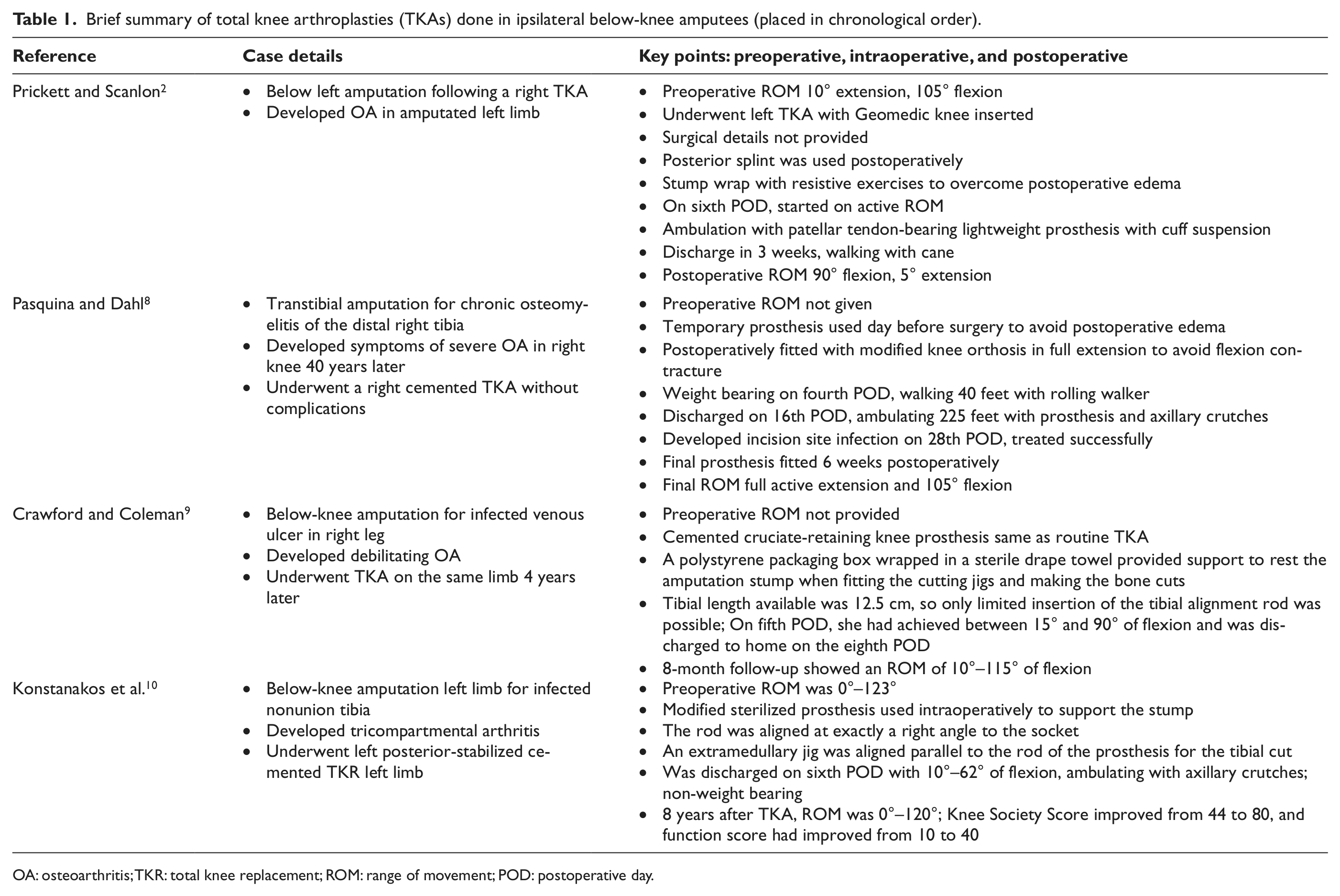
OA: osteoarthritis; TKR: total knee replacement; ROM: range of movement; POD: postoperative day.
THA
THA, or surgical replacement of the hip joint with an artificial prosthesis, is a reconstructive procedure that has improved the management of diseases of the hip joint. Usually, THA becomes a therapeutic option when conventional medical therapy fails. THAs have also found success in amputated limbs. An incidence of 5%–12% of ipsilateral or contralateral hip OA in 41 patients who had above- or below-knee amputation after a minimum of 5-year follow-up has been noted. 11 Despite surgical success, patients can have issues with prosthesis that might need modifications to accommodate the stump. The surgery results in change in alignment and lower extremity positional changes. With repeated fittings and modifications to the prosthesis, patients can achieve maximum ROM. 2
An early report published in 1953 described patients with hip OA who were successful with metallic prosthesis and THA in the ipsilateral side of the amputation. 12 The surgeons describe five such cases, details of which are provided in Table 2. Although no preoperative ROMs are provided by the authors, they used a plaster spica postoperatively on the stump for 3 weeks and suggested that after suture removal (3 weeks), and with 2 weeks of exercises, the patients may be fit to use their prosthetic limb. The outcome in all the cases was relief of osteoarthritic pain. The ROMs achieved postoperatively were not provided, but all patients were ambulatory. Another isolated case report described that preoperative rehabilitation may be required in case of hip joint instability preoperatively. 2 The surgeons had used a posterior approach for the THA for a case with transcervical fracture of the femur. In this patient, preoperative gluteal and quadriceps muscle exercises were begun that continued postoperatively. This patient could not use the stump prosthesis until the third postoperative day, after which she could ambulate with a walker. With continued physical therapy, the distance of ambulation increased. However, the THA had lengthened the limb by 1.2 cm, and hence, new fittings for a new prosthesis were required. Nine weeks after surgery, her ROM was 105° flexion, 30° abduction, and 0° extension.
Brief summary of total hip arthroplasties (THAs) done in ipsilateral amputees (placed in chronological order).
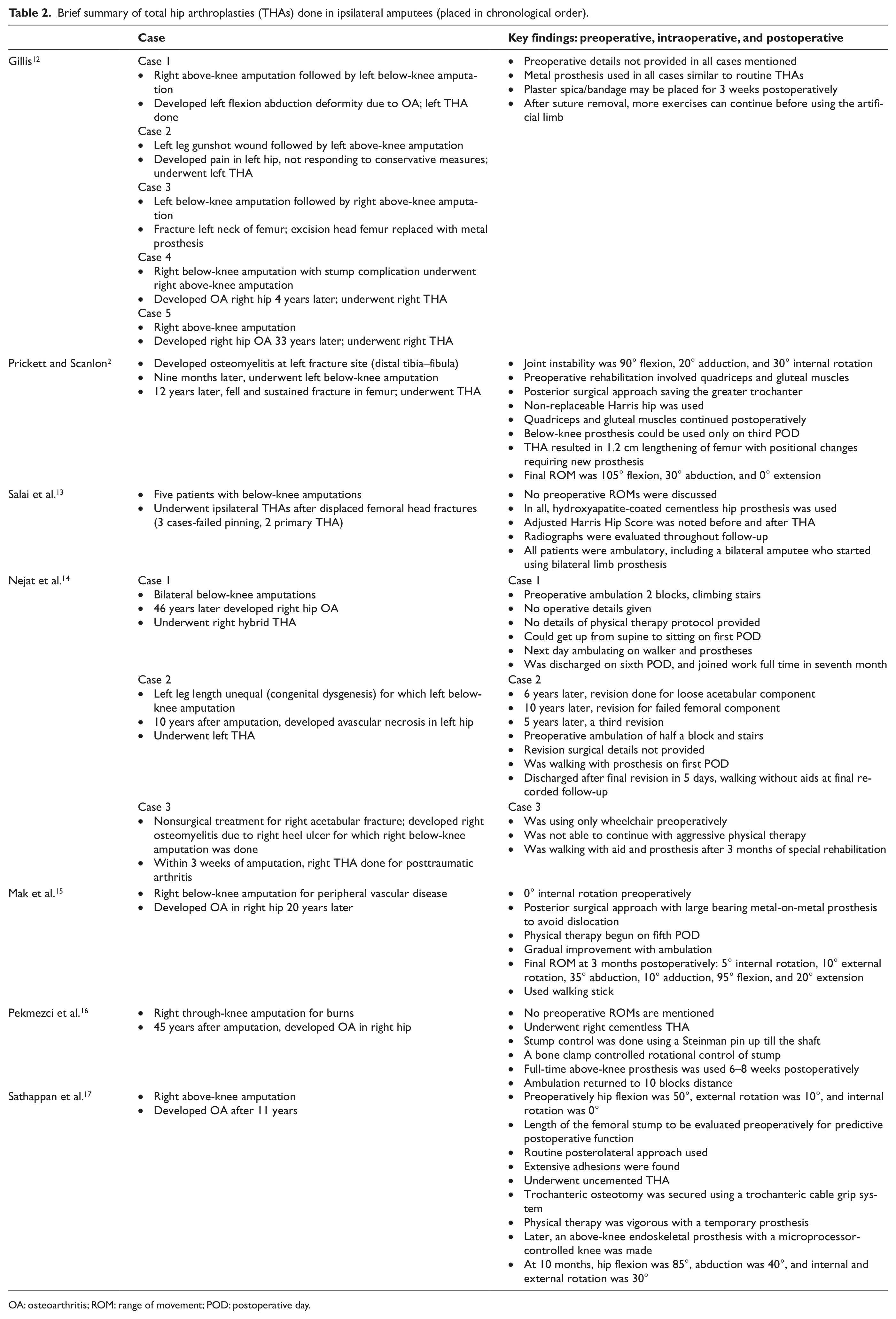
OA: osteoarthritis; ROM: range of movement; POD: postoperative day.
Much later, a series of five patients were treated after a displaced, subcapital femoral head fracture in patients had a below-knee amputation in the same extremity with “excellent” to “good”(as evaluated by adjusted Harris Hip Scores to prefracture status) results. 13 All patients were evaluated by radiographs postoperatively. This study concluded that displaced subcapital femoral fractures in adult amputees should be treated primarily by either hemiarthroplasty, preferably bipolar, or THA.
In fact, above-knee amputees with hip OA also benefit from THA. This was demonstrated in an above-knee amputee who developed hip OA in the ipsilateral limb and who underwent successful THA through a standard posterolateral approach. 17 The patient had a preoperative hip flexion of 50°, external rotation of 10°, and internal rotation of 0°, with an above-knee femoral stump of sufficient length to accommodate a standard diaphyseal locking uncemented femoral stem. The surgeons had to use a trochanteric cable grip system to the osteotomy. The capsule was firmly adherent, and upon release, uncemented THA was done. Postoperatively, once edema subsided, a temporary prosthesis was used to provide practice for weight bearing. After following the regular postoperative rehabilitation exercises including ROM exercises, isometric hip abductor strengthening, progressive ambulation with a walker, and then crutches were initiated. An above-knee endoskeletal prosthesis that had a microprocessor-controlled knee was fitted that resulted in the patient being very comfortable. After 10 months, his hip flexion was 85°, abduction was 40°, internal and external rotation was 30°, and Harris Hip Score was 90. The surgeons in the above-knee THA conclude that such patients are more prone to hip OA in the ipsilateral limb, and outcomes are better than below-knee cases. However, vascular comorbidity, residual limb length, extent of contractures, and type of implants used are prognostic factors. The authors suggested that trials with different types of components may have to be done even intraoperatively to confirm stability.
A through-knee amputee, who developed secondary to burns at the age of 6 years, developed hip OA at the age of 51 years in the ipsilateral side. 16 Since positioning the stump is important, the surgeons used a 5-mm Steinman traction pin in the distal femur through the distal shaft, following which a standard horseshoe traction apparatus was attached. The hip joint was exposed through a standard posterolateral approach, and the traction pin and the addition of a bone clamp further helped in securing the cementless acetabular and femoral components in the appropriate position. At 18 months, with his above-knee prosthesis, he remained pain-free.
Peripheral vascular disease leading to a right below-knee amputation and subsequently resulting in pain and radiodiagnosis of hip OA has also been reported. 15 The patient had 0° internal rotation and was given muscle strengthening exercises prior to surgery after medical management failed. Using a posterior approach, a large metal-on-metal prosthesis was used. Physical therapy commenced only on the fifth postoperative day and prosthesis use on eighth postoperative day, and within a month, the patient was able to leave hospital. At the 3-month follow-up, internal rotation of 5°, external rotation of 10°, abduction of 35°, adduction of 10°, flexion of 95°, and extension of 20° were observed.
The role of physical therapy and rehabilitation has been stressed in a retrospective study that included patients who had ipsilateral THAs to the amputated limb at their center. 14 The study highlighted ambulation success achieved in three such patients whose details are provided in Table 2. Surgical details and physical therapy protocol undertaken by the patients were not described; however, the authors go on to note that compared to the non-amputees in their center who needed only an average of 1.2 days for ambulation with a walker, amputees with THA needed an average of 5.5 days. They also suggested that 6 weeks of postoperative period with aggressive physical therapy is vital among amputees with THAs to avoid dislocation.
THAs can provide favorable outcomes despite the cause for the development of osteoarthritic changes in the ipsilateral amputated limb. The goal for THA remains the same as for non-amputees, that is, alleviate pain and increase mobility and joint function. In all the cases reviewed above, it is apparent that modifications to routine THA is imminent in each case, whether THA is done for below-knee, above-knee, or even through-knee amputees. When surgical approach may be possible as routine THAs, postoperative rehabilitation, discharge times, and ROM outcomes are dependent on type of knee amputation with respect to ambulation with prosthesis after surgery. A brief summary of the cases described above is detailed in Table 2 (in chronological order).
In conclusion, total joint arthroplasties can offer patients with amputations and disabling ipsilateral OA of the hip and knee joints alleviation from pain and increased ambulation with slight modifications during surgery with adjustments in existing rehabilitation protocols as compared to normal patients. A proper fit of the prosthesis to accommodate the postsurgical limb is key to achieving maximum success. However, a detailed preoperative evaluation must be added that includes cause and history of osteoarthritic pain, comorbidity if any, and ROM status, followed by planning for the surgical approach and method, type of implant, and an individualized physical therapy protocol, which can lead to successful outcomes.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.