
Abstract
Background:
Two persons presented with severe stump pain following transfemoral amputation.
Case description and methods:
A 21-year-old female and a 31-year-old male with transfemoral amputation were ambulatory with prostheses and suffered from severe stump pain caused by the presence of masses around the tip of the bone stump. From the clinical courses, imaging studies, and the intraoperative findings, the masses were diagnosed as a relatively rare condition known as chronic expanding hematoma.
Findings and outcome:
The two patients were treated successfully with surgical resection. The hematomas were soft cystic masses with a thick capsule containing old blood clots and serous fluid. There were no pathological signs of malignancy. After surgical treatment, the patients achieved walking without stump pain.
Conclusion:
Although chronic expanding hematoma is a rare condition, it should be considered as a possible cause of stump pain.
Clinical relevance
Stump pain is caused by many conditions. Although chronic expanding hematoma is a rare condition, it should be considered as a possible cause of stump pain.
Keywords
Background
Following lower extremity amputation, patients are prone to a variety of problems related to function, to fitting and alignment of the prosthesis, and problems common to all persons following amputation, including dermatologic and medical complications secondary to prosthetic use. 1 It is essential to diagnose the cause of problems that hamper walking and activities promptly. Stump pain may be a valuable sign of those problems. Stump pain is caused by many conditions, such as aggressive bone edges, heterotopic ossification, osteomyelitis, cancer and tumor, cellulitis, neuroma, stress fracture, and bone bruises. 2 The reported incidence of stump pain can be as high as 68% 3 to 74%. 4 Here, we report two cases in which patients suffered stump pain following transfemoral amputation due to chronic hematoma at the tip of the bone stump. Most hematomas subside without causing any serious clinical problems. However, some persist for long periods and appear clinically as slowly expanding lesions in soft tissues simulating neoplastic growth. These hematomas are called chronic expanding hematomas (CEHs). CEHs were reported initially by Friedlander and Bump 5 in 1968 and were well defined with pathological considerations by Reid et al. 6 in 1980. The pathogenesis of these lesions is similar to those of chronic subdural hematomas, pseudotumors in hemophilia, hemorrhagic neuropathy, and rectus sheath hematoma. 7 From imaging studies and intraoperative findings, we diagnosed the hematomas observed in two cases following transfemoral amputation as CEH.
Case description and methods
During the course of follow-up at the outpatient prosthetic clinic of the institution, two patients who suffered from stump pain following transfemoral amputation were noted to present with CEH. The institutional review board does not require additional approval for retrospective case studies, and informed consent to use their data was obtained from the patients.
Case 1
A 21-year-old female with a history of bipolar disorder was amputated at her left thigh because of necrosis due to compartment syndrome after being in a kneeling position for 20 h due to overdosing hypnotics. After 4 months of rehabilitation, although she was not able to walk in difficult conditions, such as steep slopes or stairs, she was able to walk outside with a cane and the prosthesis. The prosthesis consisted of a total surface bearing socket with an Icelandic roll on silicone socket (ICEROSS) silicone liner (Ossür ICEROSS Trans Femoral™), a pin lock suspension system, polycentric knee joint (Ossür Total Knee 2000™), and an energy storing foot (Freedom Innovations RS2000™). A total of 16 months after the amputation and due to weight loss, she complained of loosening in the proximal socket and slight piston motion inside the socket. The complaint was addressed by narrowing the inside diameter of the socket without difficulty at that time, and she proceeded using the prosthesis. A total of 18 months after the amputation, without any history of an injury to the stump, she began having severe pain in the lateral tip of her stump that made walking difficult. Physical examination revealed a soft mass with tenderness beside the lateral tip of her bone stump. X-ray imaging showed a sharp ossification on her bone stump. Magnetic resonance imaging (MRI) revealed a T1 iso-high, T2 high, fat suppression (short inversion time inversion recovery (STIR)) high mass of a maximum diameter of 30 mm. Computed tomography (CT) angiography revealed a mass rimmed with a high-density capsule without contrast effect in the center, surrounded with abnormal vascularity from the deep femoral artery (Figure 1). Laboratory findings, including a coagulation profile and platelet counts, were within normal range. From the clinical course and the imaging studies, a diagnosis of CEH was made.
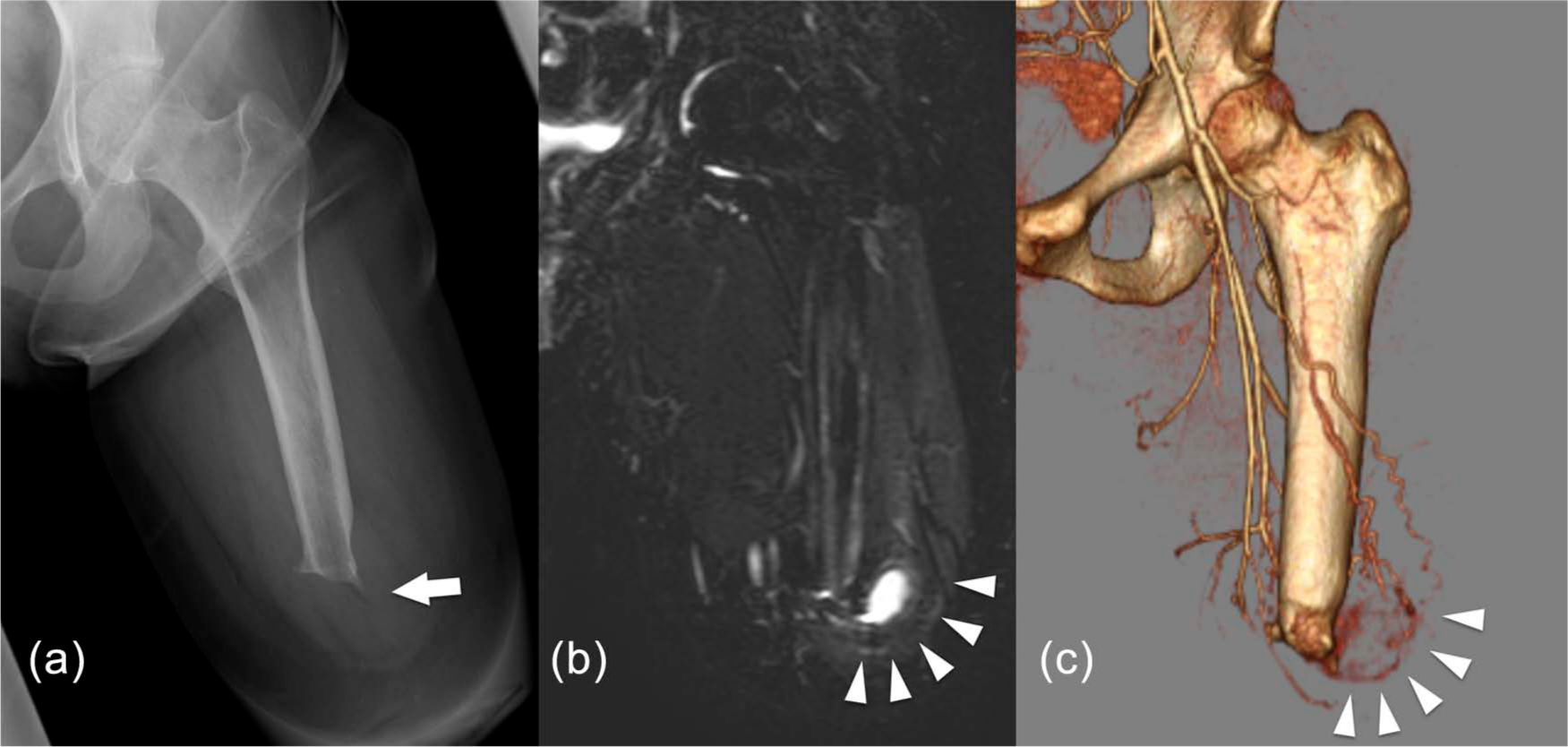
Coronal views of the stump. (a) simple X-ray showing sharp ossification on the tip of the bone stump (arrow), (b) MRI fat suppression (STIR) image shows high-intensity mass of maximum diameter of 30 mm (arrowheads), and (c) CT angiography shows mass surrounded with the abnormal vascularity from the deep femoral artery (arrowheads).
Case 2
A 31-year-old male was amputated at his right thigh because of the necrosis due to open fracture of his right lower leg caused by a motorcycle accident. After 6 months of rehabilitation, he was able to walk with a prosthesis, which consisted of total surface bearing socket with an ICEROSS silicone liner (Ossür ICEROSS Trans Femoral), a pin lock suspension system, polycentric knee joint (Ottobock 3R20™), and solid ankle cushion heel (SACH) foot (Ottobock Dynamic Foot1D10™). He showed a tendency toward obesity due to immobility after the amputation. His height was 160 cm, and his weight was 71 kg, thus gaining 10 kg during the 6 months after the amputation. Although adjustments of liner and socket fitting were difficult, after two revisions the socket fitting became steady. A total of 6 months after the amputation, he was able to walk more than 1 km with his prosthesis and a crutch. A total of 8 months after the amputation, without any history of injury to the stump, he reported tenderness in the lateral tip of the bone stump that caused difficulty in walking. Physical examination revealed tenderness beside the lateral tip of his bone stump. X-ray imaging showed a blunt ossification on his bone stump. MRI showed a mass of a maximum diameter of 25 mm with T1 high, T2 high STIR high intensity (Figure 2). Laboratory findings, including a coagulation profile and platelet counts, were within normal range. From the physical examination and the imaging studies, a diagnosis of CEH was made.

Coronal MRI T1 image shows a mass with a maximum diameter of 25 mm with high intensity inside (arrow).
Findings and outcomes
Case 1
After the diagnosis of CEH, the 21-year-old female patient was admitted to hospital. Complete excision of the mass was performed by skilled plastic surgeons who were well versed in amputation and stump care. At operation, a skin incision was made along the former operation scar. The mass was located between the vastus lateralis and biceps femoris muscles, and the deepest portion of the mass was attached to the lateral tip of the bone stump. Intraoperative findings were a cystic mass with a yellowish thick capsule, containing 4 mL of serous fluid (Figure 3). The mass was surgically resected, and the sharp ossification was trimmed to prevent recurrence. Histological findings were a cystic lesion covered with fibrous connective tissue with mild hyperplasia of microvasculature. There was no histological finding of neoplasm. A total of 3 weeks after the operation, the socket was newly made for a better fit with the stump after the operation. After 6 months of rehabilitation as an outpatient, she resumed walking without stump pain. At that time, she was able to walk more than 1 km with the prosthesis and a cane. There was no postoperative complication, and there was no sign of recurrence at the 2-year follow-up.

Intraoperative findings: serous fluid was aspirated from the cystic mass.
Case 2
After the diagnosis of CEH, the 31-year-old male patient was admitted to hospital, and complete excision was performed by skilled plastic surgeons. At operation, a skin incision was made along the former operation scar. The mass was located around the point where the adductor muscles were sewn up to the bone stump. The deepest portion of the mass was attached to the lateral tip of the bone stump. The mass was surgically resected, and the bone edge was trimmed to prevent recurrence. Intraoperative findings were of a soft cystic mass with thick capsule containing an old blood clot and serous fluid (Figure 4). Histological findings were connective tissue, including hyperplasia of microvasculature and fibrin, compatible with the wall of hematoma. There were no histological findings of neoplasms. A total of 8 weeks after the operation, a new socket was built to fit the stump after the operation. With 10 more months of rehabilitation and nutrition counseling at outpatient clinic, he resumed walking without stump pain. Finally, he could walk more than 1 km without a cane, and he could also walk mild slopes. There was no postoperative complication, and there was no sign of recurrence at the 1-year follow-up.

Dissected soft cystic mass with a thick capsule and an old clot inside.
Discussion
In previous reports, CEH was shown to occur in many locations, such as the calf, 5 thigh,7–10 knee, 11 buttocks, 12 abdomen, 6 pelvis, 13 thorax, 14 and breast, 15 and often simulated neoplasms. It is thought that the initial hemorrhage is caused by trauma due to surgery,6,8,13,15 minor blunt trauma,7,11 or gunshot wound. 5 Sometimes, patients do not remember any history of an antecedent traumatic event.10,12 CEH expands chronically. In previous reports, hematoma was detected from 2 weeks 11 to 46 years 13 after the initial trauma. Although CEH has been reported in many anatomic locations, to the best of our knowledge, CEH occurring at an amputation stump edge has not been reported.
Pathologically, CEH has a central mass of fresh and old blood, a wall of granulation tissue, and dense fibrous tissue at the surrounding peripheral wall. Microscopically, the outer zone is a dense, collagenous tissue with deposits of hemosiderin and many clusters of iron-laden macrophages. 6 The self-perpetuating expanding nature appears to be due to the irritant effects of erythrocytes, hemoglobin, leukocytes, and other blood elements. These irritant factors are thought to induce mild inflammation, which increases vascular wall permeability and bleeding from dilated capillaries in the granulation tissue beneath the capsular wall, resulting in expansion of the hematoma. 13
Simple X-ray is not sufficient for the diagnosis of CEH and CEH is often diagnosed with CT10,12 or MRI.10–13 In particular, diffusion-weighted images can detect the pathological feature of fresh and old blood component as is seen in the central mass of the CEH. 13 Angiography10,11 or CT angiography can depict abnormal vascularity around the cystic lesion as is seen in our Case 1. For differential diagnoses from soft tissue neoplasms such as sarcomas, 99m Tc–methylene diphosphonate (MDP) bone scan is also useful. 11
After the amputation, heterotopic ossification around the bone edge is a common complication, and sometimes, it grows sharp as was seen in Case 1. In these two cases, after the surgical resection of CEH with trimming of the sharp bone edges, and with the newly made sockets and months of rehabilitation, both patients gained ambulation without stump pain and without recurrence of hematomas. Therefore, we speculate that initial hemorrhages were caused by a minor trauma around the sharp bone edge. In addition, the change of liner and socket fittings may trigger the initial hematoma. Persons following amputation are vulnerable to weight change due to immobility and psychological problems after the amputation. As was observed in Case 1, the loose fit of the socket might have caused weight bearing at the stump end, which might cause hemorrhage around the bone stump. Also, the liner fit may loosen more than was intended. However, in Case 2, tight fitting of the liner and socket may cause high pressure around the bone stump resulting in hemorrhage around the bone edge. After the initial hemorrhage, prosthetic use may have caused the repetitive shearing force around the bone stump, which results in repetitive hemorrhage around the bone edges. The soft tissue around the bone stump may have been dragged by the pin lock suspension system with the negative pressure between stump surface and the silicone liner. We suggest that this repetitive mechanical stress favors the growth of hematomas.
Conclusion
In the two cases discussed in this report, both patients presented with stump pain following transfemoral amputation. From the clinical courses, imaging studies, and intraoperative findings, the hematomas were diagnosed as CEH. The patients were treated successfully with surgical resection with trimming of sharp bone edges. Although CEH is a rare condition, it should be considered as a possible cause of stump pain in amputees.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.