
Abstract
Background:
Traditionally, clinical protocols for the treatment of young children who require a knee prosthesis have favored stability, with the prosthetic knee locked into full extension until after the child has learned to walk. Recently, an Early Knee protocol has been investigated, in which children receive an articulating knee in their first prosthesis and use it while learning to crawl and walk.
Objectives:
This study investigated the presence of swing phase clearance adaptations in the walking gait of seven young children aged 18–92 months, who had been fitted according to the Early Knee protocol.
Study design:
Before-and-after experimental design.
Methods:
Each subject completed walking trials with the knee freely flexing and trials with the knee locked into full extension to mimic a traditional knee protocol.
Results:
Subjects utilized the articulating knee in walking, with an average of 70.4° of peak swing phase knee flexion. Some clearance adaptations were present with the flexing knee; more were present and their magnitude was increased when the knee was locked. In particular, there was a statistically significant increase in circumduction.
Conclusions:
These results suggest that the Early Knee protocol can reduce the adoption of clearance adaptations while walking is developing.
Clinical relevance
Treatment of young children who require a knee prosthesis is inconsistent. Traditionally, no knee is provided until independent walking is achieved. A newer Early Knee protocol provides an articulating knee in the first prosthesis. This study found that children use the articulating knee in walking and develop fewer clearance adaptations.
Background
Young children with limb loss who require a prosthetic knee joint present a unique rehabilitation challenge to clinicians. Historically, clinical protocols have placed the goal of stability over the goal of neuromotor development. The most stable knee is one that is locked into full extension at all times. However, this stability comes with a price. A knee locked in full extension is a substantial hindrance during crawling, walking, and age-appropriate functional activities. Nonetheless, standard practice does not provide children with a flexing knee joint until they reach 4 or 5 years of age, after they have learned to walk independently without assistive devices.1–8 Watts 7 has stated, “A one-year-old who can barely toddle on two normal legs can’t be expected to manipulate prosthesis with an articulated knee joint.” No data exist to support this conviction. In fact, no research references in the Physical Therapy or Prosthetic and Orthopedic texts and journals support these statements, yet the writings have guided the practice of pediatric prosthetics for years. 9 This conventional wisdom has remained unchallenged until recently.
In a few clinics, some practitioners have begun fitting children with a working prosthetic knee at a very young age. Anecdotal evidence has been highly favorable, with infants and toddlers crawling or toddlers and young children walking successfully on passively flexing prosthetic knees. Infants who learn to crawl with a working prosthetic knee may be able to participate in more age-appropriate motor activities than those without a flexible knee, and in so doing may develop muscular strength and neuromotor control that would otherwise be delayed. In addition, children who transition to walking with a working prosthetic knee may avoid the development of deleterious clearance adaptations in the swing phase of gait. These adaptations include vaulting (contralateral ankle plantarflexion), hip hiking (ipsilateral upward pelvic obliquity), and circumduction (ipsilateral hip abduction during flexion).
A few studies have shown that young children with limb loss can have gait patterns that parallel those of their able-bodied peers when provided with an articulating knee.10,11 Wilk et al. 11 studied the effects of transitioning young children from extended knees to articulating knees on clearance adaptations in gait. Geil and Coulter-O’Berry 10 investigated the effects on crawling of an “early knee protocol,” in which children were provided with an articulating knee in their first prosthesis. The present study addresses the implications of this protocol in young children who have transitioned to walking.
Motor learning/control research forms the theoretical basis for this analysis of movement patterns in young children. In 2000, Adolph and Avolio 12 studied motor strategies in 24 healthy walking infants on adjustable steep and shallow sloping surfaces wearing either a featherweight or lead weighted vest. The infants safely negotiated the steep and shallow slopes in the lightweight vest but were cautious or even changed their motor strategies in the heavy vest on the same slope. On the same slopes that presented little problem in the lightweight vests, some infants altered the movement and even refused to proceed when wearing the heavy vest. Adolph’s study looked at infants’ perceptual skills and ability to anticipate the environment, the slope. It was thought that the heavier vests made it more difficult for infants to move with greater fear of falling because they posed greater threats. Infants adapt on many different levels: behavioral, kinematic, and muscular. Adolph and Avolio’s research may be generalized to this study such that infants and toddlers may perceive an unnaturally locked leg as a threat, which limits their ability to discover new motor skills through crawling, walking, environmental exploration, and play.
It is important to distinguish the clearance adaptations associated with swing phase foot–ground clearance in the presence of an obstacle or, in this case, an immobilized knee from the natural variability present in a developing child. The theory of neuronal group selection provides a foundation for and further expansion of the Dynamic Systems Theory. 13 Neuronal group selection is constrained by genes and influenced by experience. The theory focuses on the developing brain and the ability of the brain to respond to environmental change. Adaptations and changes occur within the individual and between the interactions of the individual with the environment by the building, grouping, refining, and balancing of neural networks. The writings of Sporns and Edelman 14 and Edelman 15 focus on neural connections that change as the individual develops favorable patterns that are successful in the environment as a function of growth and maturation, current context, and past experiences. In early locomotion, this environment can include ground obstacles and varied surfaces. Foot–ground clearance is a variable in development of gait, as the interaction with the environment is refined.
Dominici et al. 16 and Forssberg 17 identified marked differences in the swing phase path of the foot between toddlers and adults and older children. These differences include increased foot–ground clearance and flat-foot initial contact. This study design does not address the process of the natural development of mature gait, but it recognizes that a prosthesis that is less biomimetic may cause changes in that process and have implications on the timing and quality of gait development.
The objective of this study is to follow recently conducted research on infants crawling with locked and unlocked knees to determine the impact of the knee following the transition to walking. The first question to address was whether or not children flex the knee during swing phase in the unlocked condition, and the following hypothesis was tested: Children with transfemoral (TF) or knee disarticulation (KD) limb loss will flex a prosthetic knee in swing phase when it is unlocked. This question seems fairly obvious but has not been established in the literature in children of this age, and the possibility exists that children might adopt a gait pattern that maintains full knee extension due to either of the following: (1) the inability to flex and extend a passive knee through hip flexor/extensor muscle firing or (2) the desire to adopt a hyper-stable gait. The implications of flexing the knee on overall gait were tested in this hypothesis: Children with TF or KD limb loss will show an increase in one or more of three gait adaptations, specifically circumduction, hip hiking, or vaulting when the prosthetic knee is locked into full extension.
Methods
Following approval from relevant institutional review boards, healthy children with unilateral TF amputation or KD (≤7 years old) were recruited. Children were able to walk safely unassisted and without an assistive device. Each child had been provided prosthetic components following the “early knee protocol,” in which an articulating prosthetic knee was provided with the first prosthesis at or about the time when the child had achieved pull-to-stand. The same certified prosthetist provided treatment for all the children in the study, and each child was tested in his or her current prosthesis.
Once informed consent was obtained, anthropometric data were recorded and 15 8-mm retroreflective markers were attached to the following anatomical landmarks: sacrum, right and left anterior superior iliac spine (ASIS), mid-femur, lateral femoral condyle, mid-tibia, lateral malleolus, heel, and second metatarsal head. Each participant was encouraged to walk along a level 10-m walkway. Each participant completed three trials with the normally flexing prosthetic knee (Unlocked, or U) and then three with the knee mechanically locked into full extension (Locked, or L). A seven-camera motion analysis system (ViconPeak, Englewood, CO) tracked the motion at 120 Hz.
Kinematic data were filtered using a fourth-order zero lab Butterworth filter. 18 Dependent variables were peak swing phase knee flexion and kinematic measures associated with gait adaptations for clearance in swing phase. Hip hiking was determined by vertical excursion of the prosthetic side ASIS marker. This was the z-coordinate in our global coordinate system, with the x-axis along the line of progression and the y-axis along the medial-lateral direction. In some gait patterns, it might be possible to identify whether or not hip hiking is occurring, particularly when the hip joint reaches a peak flexion angle during mid-swing and maintains that angle through the rest of swing phase. 19 In that case, a local maximum might indicate hip hiking. However, in pediatric gait, such a local maximum is often present even in normal hip flexion/extension graphs, 20 and vertical excursion of the hip varies considerably with age. 21 Consequently, hip hiking was assessed by the relative height of the peak ASIS z-coordinate during swing with respect to the z-coordinate of the same marker at the onset of swing. Circumduction was determined by the angle of the ipsilateral femur segment in the frontal plane, based on the inverse tangent of the difference in z-coordinates of the hip and knee joint centers divided by the difference in y-coordinates. 22 The maximum swing phase value for each parameter was recorded for each trial. Vaulting was determined by contralateral ankle plantarflexion angle during swing phase. On the plot of the contralateral ankle angle from opposite toe off to opposite initial contact, vaulting was evident by a period of plantarflexion during the expected second rocker dorsiflexion. When the plantarflexion formed a local maximum, vaulting was quantified as the plantarflexion peak minus the previous local minimum. In some cases, the vault did not form a local maximum, but an inflection change in the curve back toward dorsiflexion was evident. In these cases, the peak plantarflexion value for vaulting was identified at the point of inflection, based on the second derivative.
The trials were averaged for each participant and compared between conditions using paired t-tests with an α-level of 0.05. We expected significant differences in at least one of the dependent variables between the U and L conditions.
Results
Seven children with unilateral KD or TF amputation participated in the study (Table 1). All subjects were able to complete the required number of trials in each condition. Postprocessing revealed some missing data due to the inability of the motion analysis system to track the small markers. This resulted in an uneven number of useful trials in some conditions.
Characteristics of subjects.
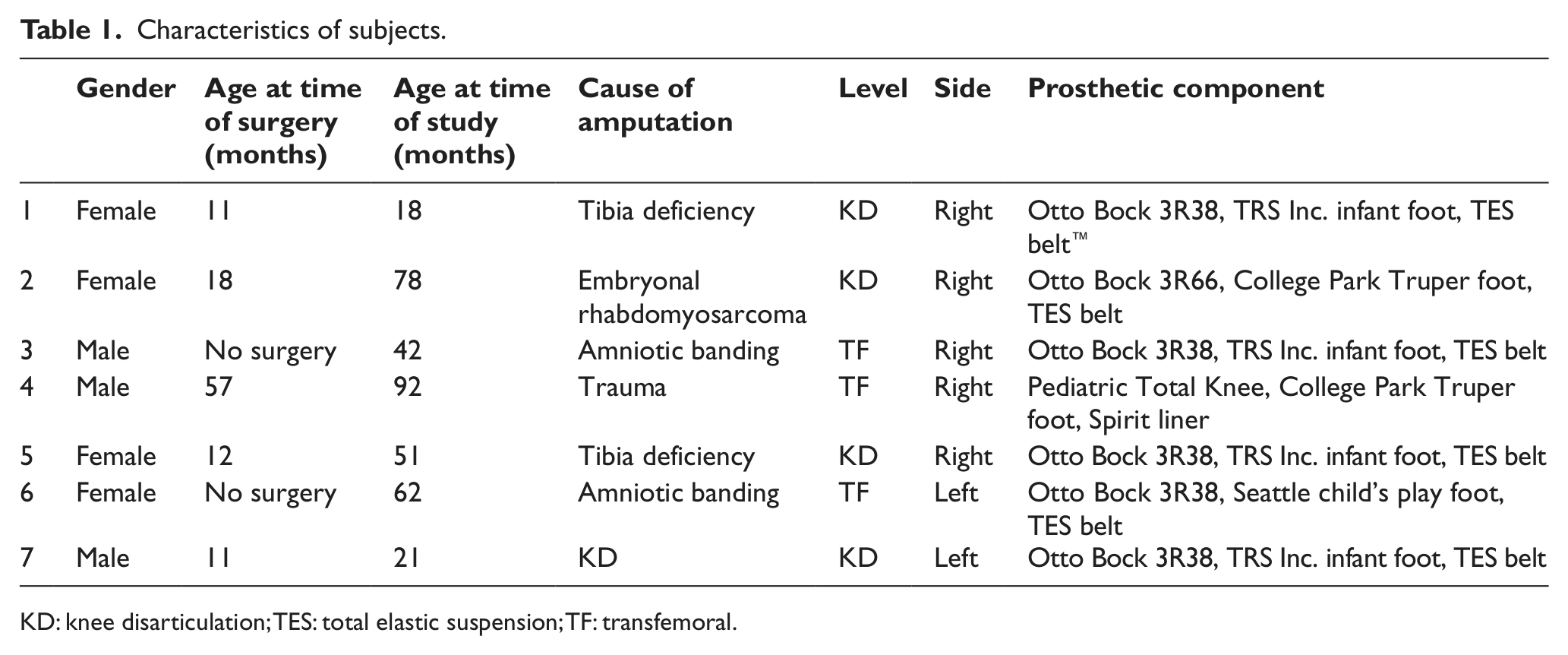
KD: knee disarticulation; TES: total elastic suspension; TF: transfemoral.
All subjects flexed the knee in the unlocked condition. Peak knee flexion ranged from a minimum of 27.0° in Subject 7, who showed consistently less knee flexion than the other subjects (Figure 1), to 90.0° in Subject 6, with an average of 70.4° across all subjects. Some subjects were particularly consistent with peak knee flexion values; for example, knee flexion in Subject 6 ranged from 88.8° to 90.0° across all unlocked trials. No children stumbled or fell in either condition, and no unlocked knees buckled in weight bearing.
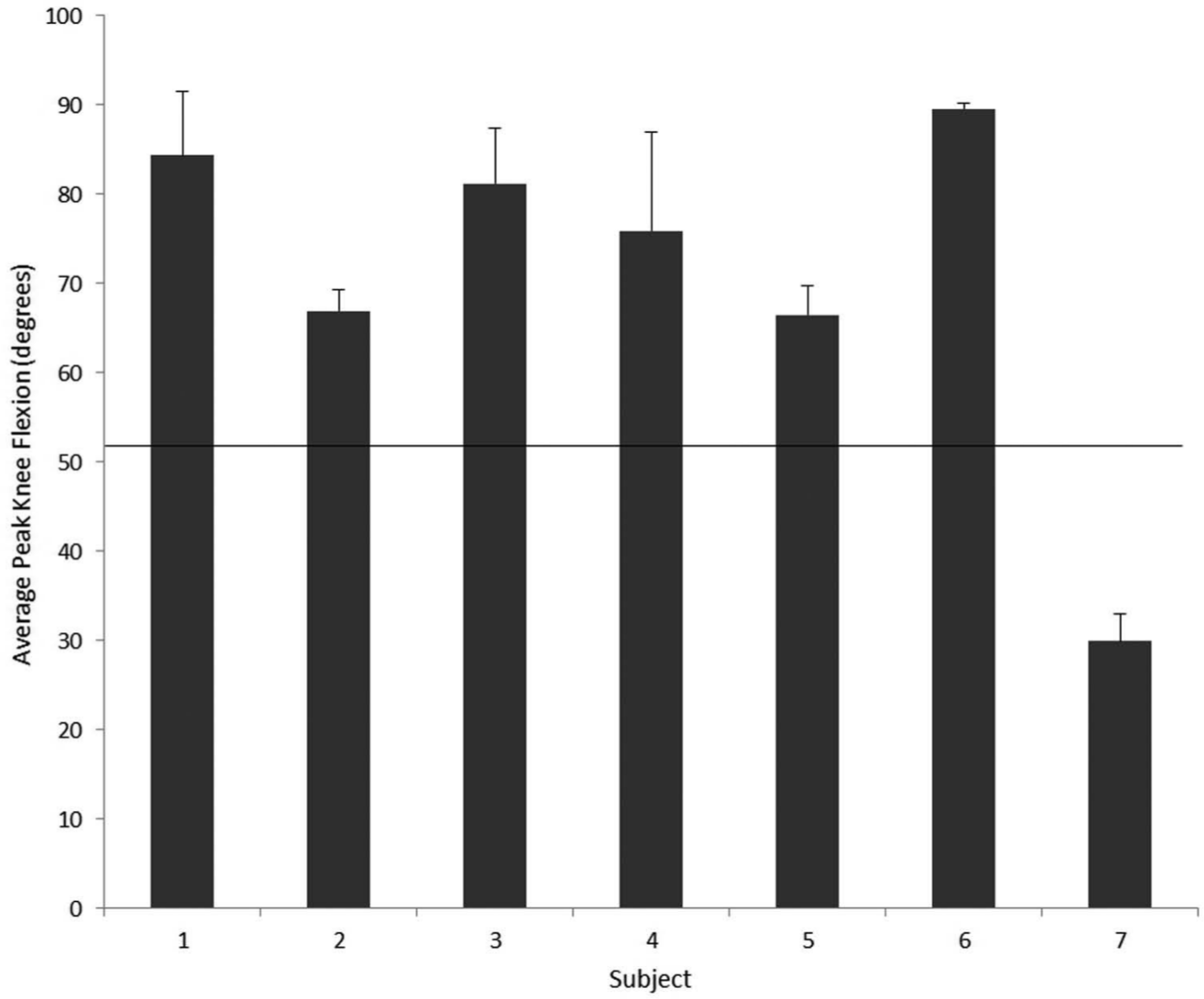
Average of peak swing phase knee flexion angle for each subject with standard deviations. Horizontal line represents a peak knee flexion value for a dataset for typically developing young children, 52.3°.
Data for all three outcome variables (hip hiking, circumduction, and vaulting) were found to be normally distributed. As a whole, the subjects did not demonstrate a statistically significant increase in hip hiking. (p = 0.85) Mean increase in ASIS marker height across all subjects for the unlocked condition was 59 mm, while the mean for the locked condition increased to 63 mm. Analysis of individual subjects shows that six of the seven increased hip hiking from condition U to condition L, with Subject 3 as the exception (Table 2). Of the six who increased hip hiking, Subjects 1 and 4 showed the greatest increase, raising the ipsilateral hemipelvis 17 mm more during swing in the locked condition.
Ipsilateral ASIS marker height increase (mm) during swing to indicate hip hiking. Subject 4 only had one useful locked trial, and so there is no standard deviation.
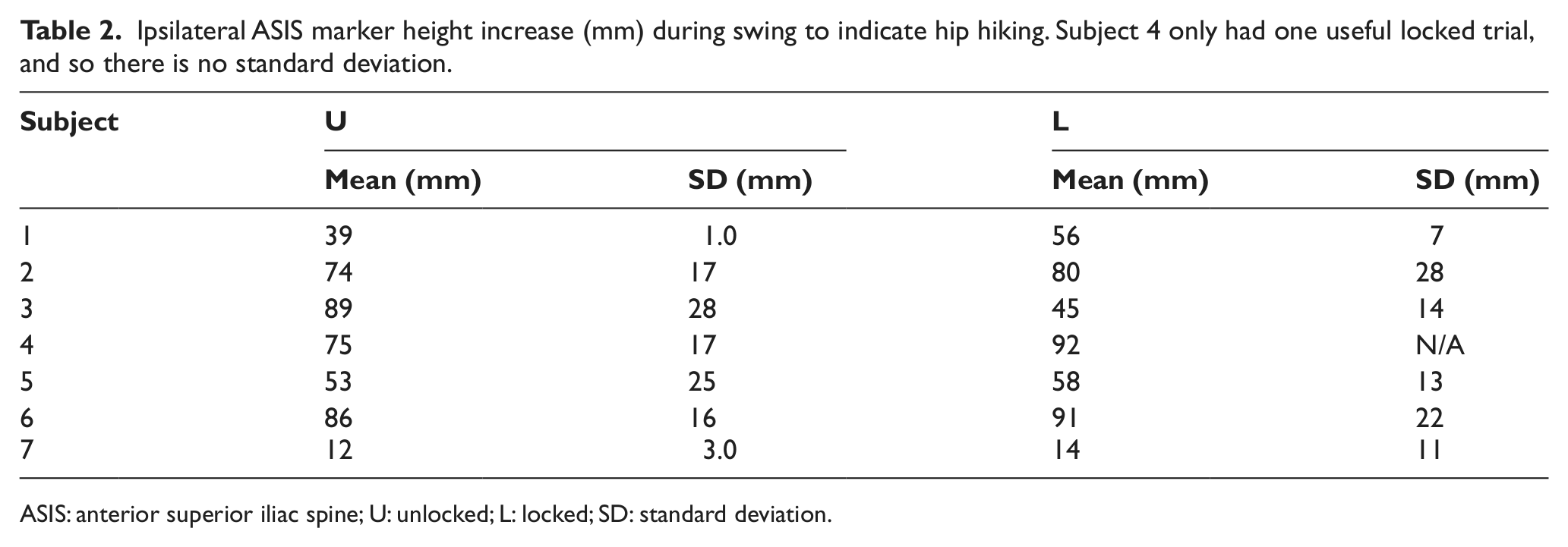
ASIS: anterior superior iliac spine; U: unlocked; L: locked; SD: standard deviation.
Statistical significance was found in circumduction results across subjects. Circumduction angle increased significantly (p = 0.038) between U and L. Individually, all subjects increased circumduction between U and L (Table 3). Several subjects revealed a wide base of support characteristic of early walkers, so some baseline angle of the femoral segment away from vertical is to be expected and may not indicate circumduction in swing. One subject in particular, Subject 7, adopted a very wide base of support and a large femoral segment angle in all trials and all conditions (Figure 2).
Circumduction: angle (in degrees) of ipsilateral femur segment in frontal plane from vertical. Subject 4 only had one useful locked trial, and so there is no standard deviation.
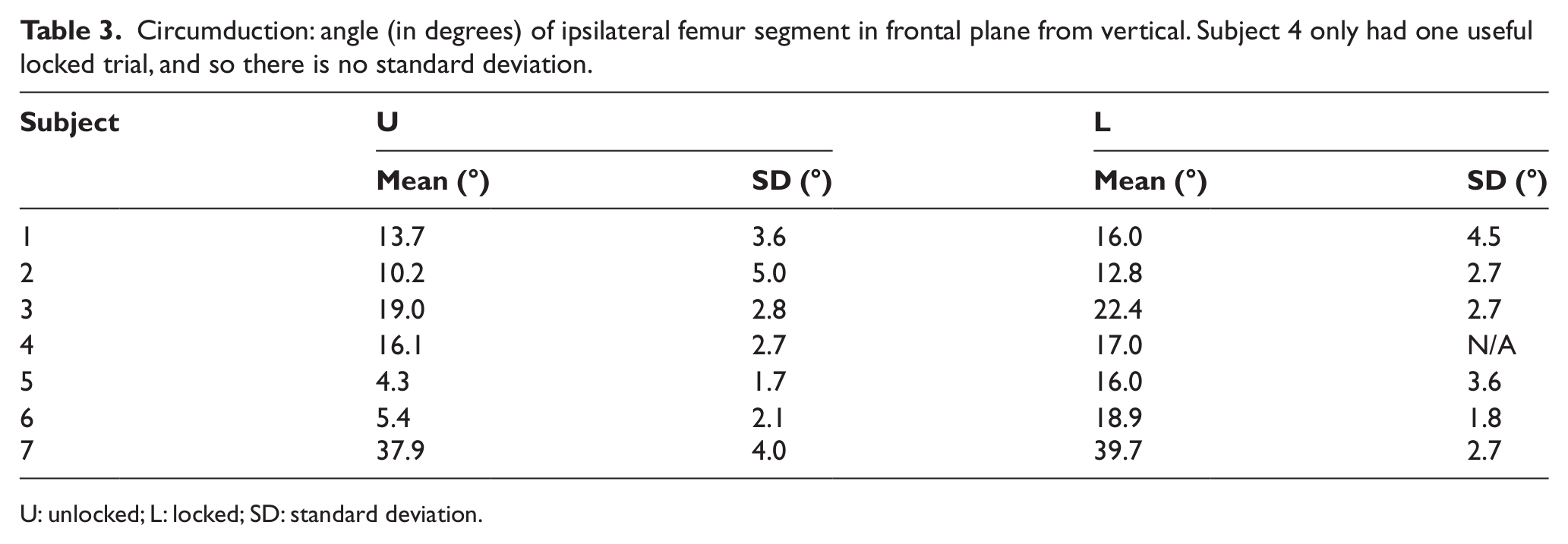
U: unlocked; L: locked; SD: standard deviation.
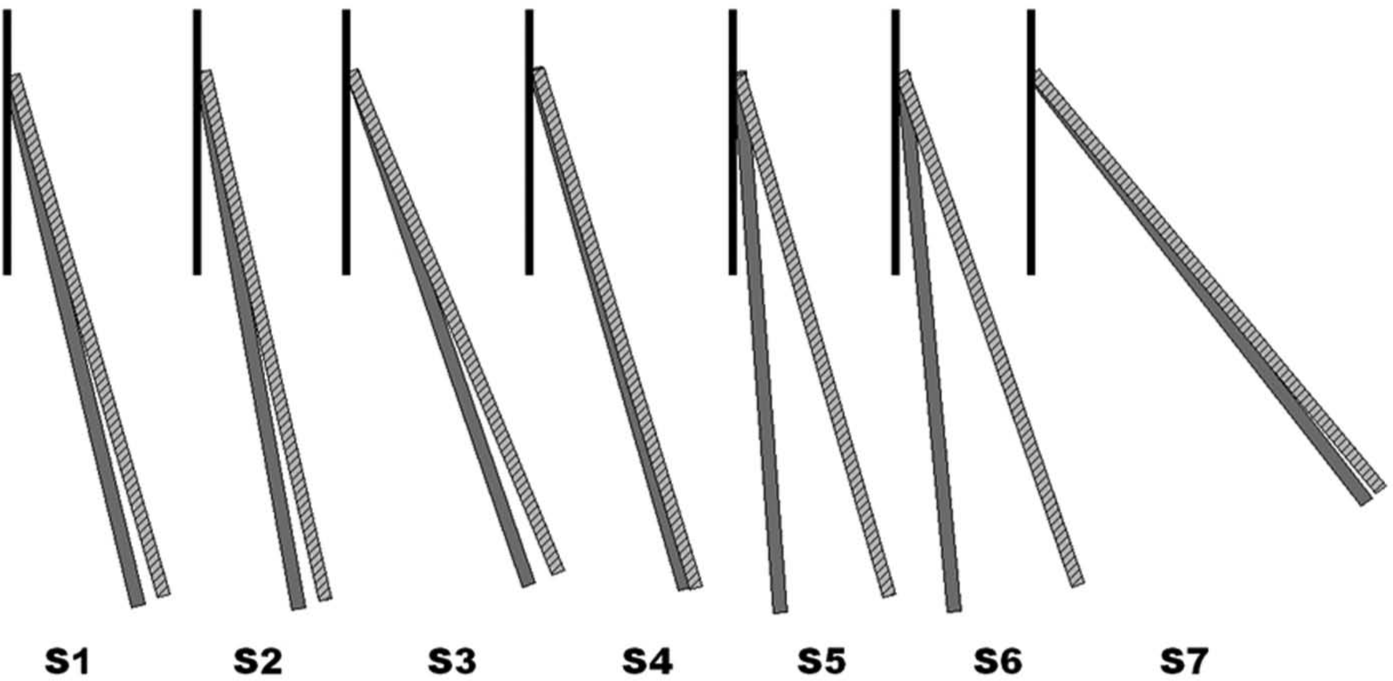
Graphic depiction of circumduction angles versus a vertical reference. Solid bar represents mean results within each subject for U condition. Striped bar represents mean results within each subject for L condition. Each subject demonstrated increased circumduction in the locked condition.
Vaulting results were highly variable (Table 4). Three subjects increased vaulting when the knee was locked, one was unchanged, and three decreased vaulting when the knee was locked. Differences across all subjects were therefore not significant (p = 0.641).
Vaulting: degrees of ankle plantarflexion motion during contralateral swing phase–average across all trials for each subject, each condition. Local maximum minus local minimum or point of inflection as determined by second derivative minus previous minimum. High standard deviations in some cases result from averaging trials of no vaulting (0) with trials containing a vaulting angle.
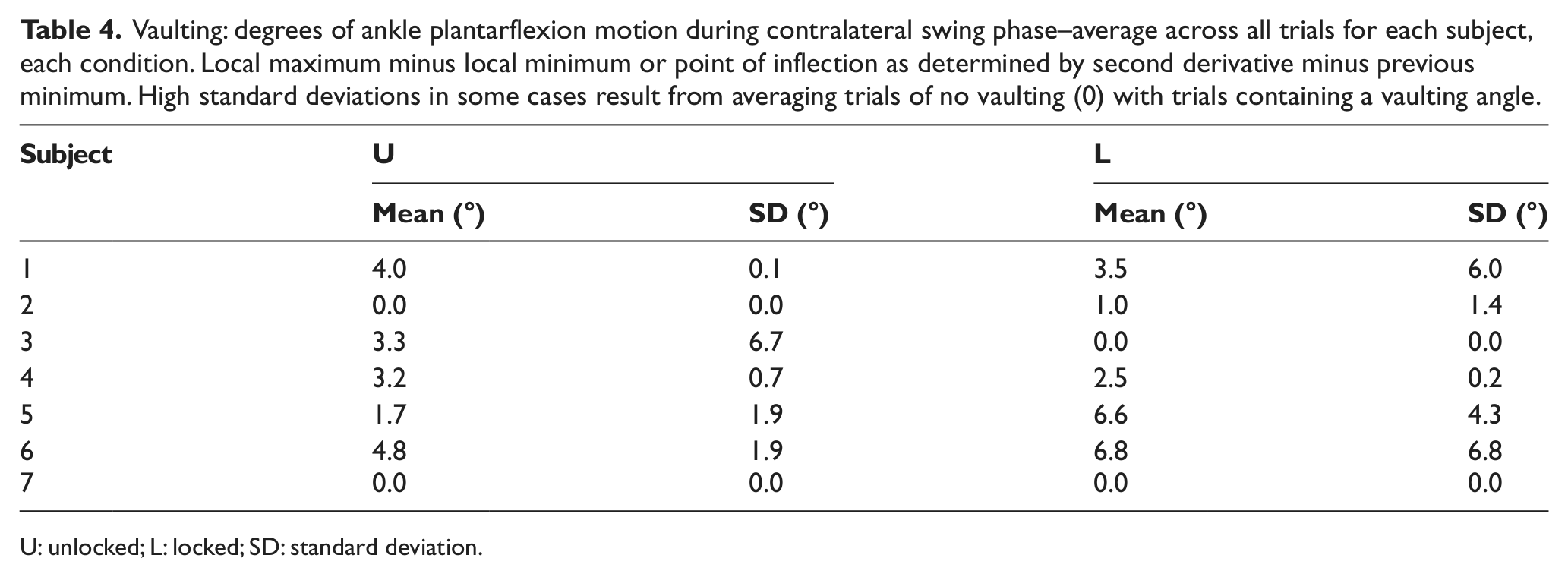
U: unlocked; L: locked; SD: standard deviation.
Individual subjects used different strategies when faced with a locked knee. Figure 3 shows individual subject percent change ((locked condition–unlocked condition)/(unlocked condition)) for each clearance adaptation. Positive values indicate that the clearance adaptation increased in the locked condition. Some subjects (1 and 5) increased all three possible clearance adaptations. Subject 7 increased hip hiking and circumduction with no change in vaulting. Subjects 2, 3, and 6 increased two adaptations but decreased one. Subject 3 was an exception, increasing circumduction while decreasing hip hiking by more than 50%, and eliminating the vaulting strategy that was present in the unlocked condition.
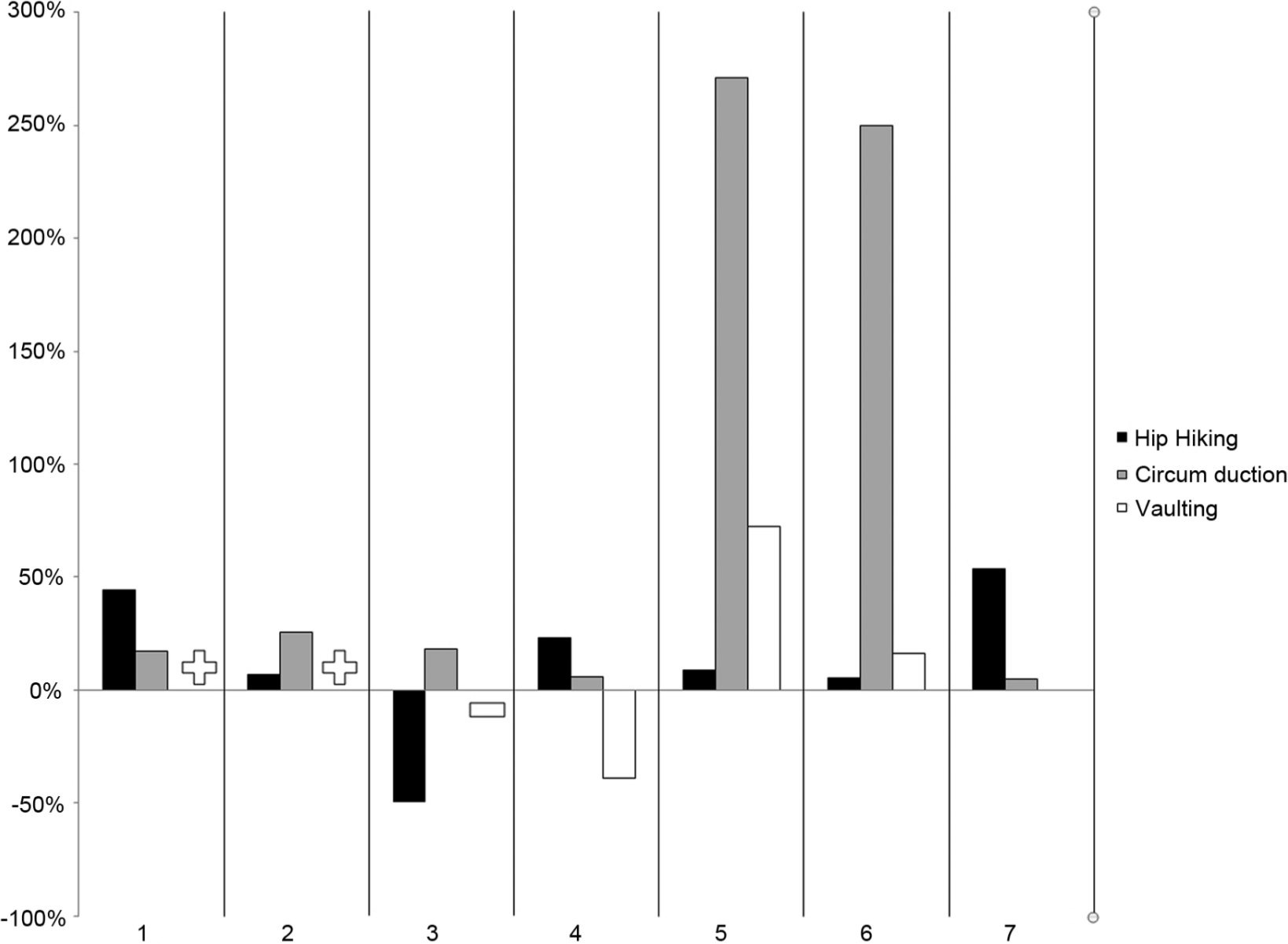
Individual subject percent change ((locked condition–unlocked condition)/(unlocked condition)) for each clearance adaptation. Plus signs represent two vaulting results in which subjects increased from zero (no vaulting) to some amount of vaulting. A minus sign indicates a subject who eliminated vaulting completely.
Discussion
The purpose of this study was to determine the impact of an articulating prosthetic knee following the transition to walking. First, the study established that children who receive an articulating knee in their first prosthesis according to the Early Knee prescription protocol actually utilize the knee during gait. Average peak knee flexion was 70.4°. Typically developing children flex the knee to approximately 52° in swing phase, according to a normative database from Selber and De Godoy. 20 Although the subjects in the study by Wilk et al. 11 were older children than those in the present study, they also demonstrated swing phase flexion using an articulated knee, averaging 49° in swing phase. In our study, knee flexion exceeded average values for typically developing children. This might be due to the amount of flexion resistance in the knee or the desire of the children to obtain excessive clearance as part of gait development. The abnormally low values of knee flexion in Subject 7 are most likely related to that same subject’s abnormally high circumduction values.
The study tested the following hypothesis related to swing phase clearance adaptations: Children with TF or KD limb loss will show an increase in one or more of three gait adaptations, specifically circumduction, hip hiking, or vaulting when the prosthetic knee is locked into full extension.
Each of the seven subjects showed at least some measure of increase in one or more clearance adaptations. Although some adopted two or three of the three possible clearance adaptations, each subject had a single predominant clearance adaptation. The “clinical significance” of these increases is difficult to determine, but some differences were certainly larger than others. Subjects 5 and 6 had increases of 11.7° and 13.5° in circumduction, respectively. Subjects 1 and 4 had increases of 1.7 cm of hip hiking each.
It is important to note that these subjects were not entirely free of clearance adaptations in the baseline condition. Although each subject had been treated with an Early Knee protocol, 10 there was still evidence of gait adaptations in the operation of the articulating knee. Nonetheless, the data suggest that these adaptations would have been more profound had the children been treated with the conventional knee prescription protocol. Six of seven subjects increased hip hiking when the knees were locked. All seven increased circumduction, some profoundly so. Three of seven increased vaulting or added a vaulting strategy when one was not previously present. Consequently, the second hypothesis was supported in all subjects except Subject 3. Although this subject did increase circumduction by 11%, which would support the hypothesis, a surprising decrease in hip hiking and elimination of a vault in the locked condition suggest otherwise.
Across all subjects, statistical significance was found in circumduction, but not in hip hiking and vaulting. This is not unexpected, since three clearance adaptations are available to each subject, and each ultimately accomplishes the same purpose. For example, Subject 6 adopted a vault of as much as 16.1° in the locked condition along with circumduction ranging from 17.4° to 21.1°, but showed no change in hip hiking. In the aggregate, these individual changes in different adaptations tend to wash out.
Reduction or elimination of clearance adaptations may have multiple benefits in a child with limb loss, who is developing walking gait. Developing normal strategies to clear the ground in swing produces a more stable gait pattern and improves the child’s ability to use articulating knees in both weight-bearing and non-weight-bearing conditions. Furthermore, elimination of clearance adaptations can increase gait efficiency in an already energetically challenging scenario.
Analysis was limited by the small sample size and the need to establish a method for quantifying vaulting, since none could be found in the literature. These were young walkers, so the fact that motor control is rapidly developing in even typically developing children at this age introduces variability in the data. Indeed, ground clearance is a variable associated with gait development, so the study population had inherent variability. The within-subjects comparison of unlocked and locked conditions helps ameliorate this concern. Anecdotally, we recognize this population as useful in the study of locomotor development. Dominici et al. 23 sought to study the kinematic patterns of unsupported toddlers while stepping over obstacles, but found that in all trials, the toddlers stopped before the obstacle and did not step over it. This indicates that the study of clearance adaptations based on functional leg length discrepancy may be more practical. Because these children received articulating knees in their first prostheses, the locked condition represented an acute perturbation. Ethical concerns did not permit extended accommodation to the locked condition.
Conclusion
All subjects in the study adopted one or more clearance adaptations when their prosthetic knee was locked into full extension. Subjects who had a clearance adaptation with a flexing knee reduced that adaptation when the knee was permitted to flex and extend. These results, combined with favorable results during crawling, 10 suggest that an Early Knee prescription protocol might encourage more typical motor development that reduces clearance adaptations.
Footnotes
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding
This research was funded by a Research Initiation Grant from Georgia State University, Atlanta, Georgia, USA.