
Abstract
Background and aim:
To our knowledge, the technique of molding orthoses to the non-load-bearing foot is still not widely investigated. The aim of this work is, therefore, first, to describe an off-loading custom-made technique and, second, to explain how it can be specifically adapted to treat Sever’s disease.
Techniques:
A technique of directly molding orthoses to the non-load-bearing foot by vacuum forming an insole to the foot fabricated with a combination of polyvinyl chloride and polyester resins, 30 Shore A hardness and 148 kg/m3 density polyethylene–ethylene-vinyl-alcohol, and a cushioning heel cup of 22 Shore A polyurethane, using a directly molding orthoses technique to the non-load-bearing foot by vacuum.
Discussion:
Results show that this new technique could be a good alternative to traditional insoles in the management of Sever’s disease pain.
Clinical relevance
Manufacturing the insole directly on the patient’s foot could lead to a better individual adaptation in general, and to manage Sever’s pain disease in particular.
Background and aim
Different techniques for manufacturing foot orthoses can be divided into two groups: prefabricated and custom-made. Although current studies did not found significant differences,1,2 individualized prescription is recognized to be a gold standard. 3
One of the custom-made orthoses is a directly molding orthoses technique (DMOT) to the non-load-bearing foot by vacuum. An insole is formed using this vacuum system using a combination of polyvinyl chloride (PVC) and polyester resins. DMOT has often been used clinically in athletes because their great flexibility allows an excellent individual adaptation. 4 The technique has also been used in the treatment of neurological foot disorders 5 and of other pathologies such as fasciitis. 6 However, there is a lack of investigations that can conclude on the effects of this technique in different foot disorders, and more information about the manufacturing process is needed.
Calcaneal apophysitis (Sever’s disease) is an overuse syndrome thought to be caused by repetitive microtrauma due to increased traction of the Achilles tendon on the calcaneal apophysis.7,8 It affects children in whom this epiphysis is still growing, generally at ages from 7–15 years in boys and 5–13 years in girls. 9
The importance of correcting misalignment, predominantly pronation, is stressed by some authors.10,11 Molded Plastazote® insoles, a heel cup to align pronation, or a heel wedge to reduce shear stress to the apophysis are included in most recommendations for heel pain.8,12-15 Non-load-bearing orthosis, with the lower limb immobilized in a short leg cast or a removable ankle orthosis worn during daytime, has been recommended in the management of Sever’s disease.8,16,17
Although there is evidence that different devices described above have shown good results in the management of patients with heel pain in general, to our knowledge, there is a lack of information on how this novel technique could be adapted and applied to patients with Sever’s disease.
The aim of this work is, therefore, to describe an off-loading custom-made technique and, second, to discuss how it can be specifically adapted to treat Sever’s disease.
Technique
Foot orthoses custom-made technique by vacuum forming on the non-load-bearing foot is discussed in this section. First, the perimeter of the foot is drawn on paper, marking the projection of the talus–navicular joint to use as the highest point of plantar support. Then the base pattern is drawn as a template to cut out the different materials (Figure 1). The materials used to make the orthoses are as follows: polyester resins with a combination of 1.2 mm Podiaflex® and 1.2 mm Podiaflux® for the rearfoot and midfoot and 0.8 mm Podiaflex for the forefoot and, as shell, a 30 Shore A and 148 kg/m3 density polyethylene–ethylene-vinyl-alcohol (PE-EVA) combination to which a 22 Shore A polyurethane cushioning element is glued onto the heel area (Figure 2).
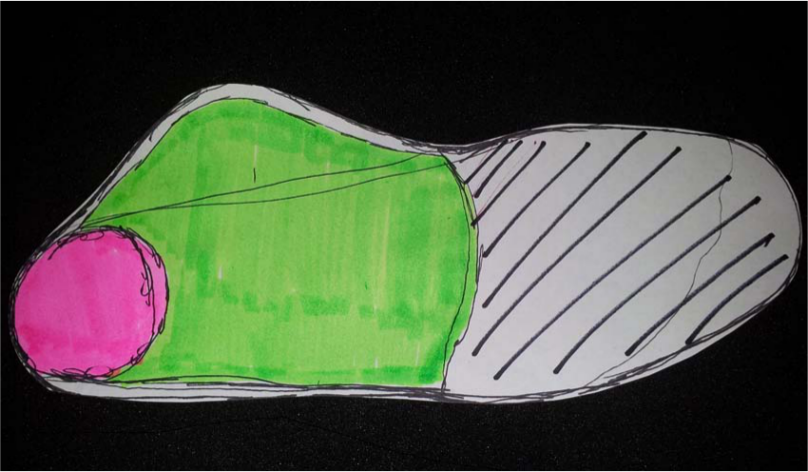
Pattern of the different elements to be cut out of the raw materials.
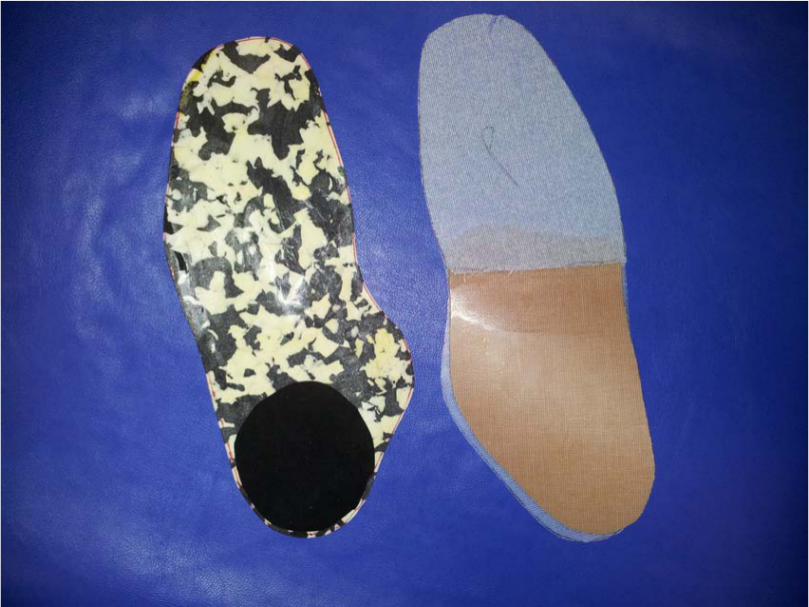
Orthoses made of PVC and PE-EVA resins.
The polyester resins are thermally fused at 105 °C for 3 min in a thermal vacuum machine. With this process, these resins keep adhered, giving more flexibility and consistence to the insole. Once resins are cooled, a new increase of temperature between 80 °C and 90 °C is given in order to glue the heel cup and the lining to the insole. Once insole is manufactured, it is applied directly to the patient, who is wearing a sock and a tubigrip to prevent burning. The patient’s foot and the insole are covered by a plastic bag that is closed by a grip and vacuum packed. Then, the insole is molded directly onto the non-load-bearing foot to form the insole. With the patient’s leg at an angle of 90°, hamstrings in total relaxation through bending the knee, the subtalar joint in neutral position, and the toes in slight extension after having been correctly aligned (Figure 3).

Technique of vacuum molding directly onto the patient’s non-load-bearing foot.
Before the patient is leaving with the insole, the definitive adjustment to the foot is made, and the patient is asked to walk with it for a few minutes so as to report any discomfort or incidence. After any further necessary adjustments, and once the patient states that he or she feels comfortable, the orthotic fit is taken as being concluded.
Study design
Eighteen male children with heel pain, ages 9.94 ± 0.8 years, participated in the study. They had presented at two podiatry private clinics in Malaga and Granada, Spain, for consultation in the period from September 2010 to June 2012. They were considered suitable candidates for orthotic intervention if they presented heel pain with a minimum of 6-week evolution and were diagnosed radiologically with calcaneal osteochondritis. 18
The exclusion criteria were having suffered some trauma in the past 2 months, having used orthoses, presenting neurological or cognitive impairment, having taken anti-inflammatory drugs, or received physical treatment for pain in the past 3 months.
The study protocol was in accordance with standard ethical and human research principles. Written informed consent for participation and publication was given by a parent of each participant, including the publication of photographs. The study was approved by the Research Ethics Committee of the University of Malaga, Spain.
The subject was asked to score on a 100 mm visual analogue scale (VAS) the pain perceived at that moment (baseline measurement). This was immediately followed by the fabrication of the orthosis and the initiation of its use.
The participant was asked to return after 15 and after 30 days of use and then score the pain level he had perceived during the previous 3 days on the same VAS.
Data were analyzed with the IBM SPSS19® (SPSS Science, Chicago, IL). The Shapiro–Wilk test applied to the data showed the distribution to be normal in the first (baseline) and second (M1) pain measurements but not in the third (M2). It was therefore decided to use Student’s t-test for paired samples to compare baseline and M1 and the nonparametric Wilcoxon signed-rank test to compare M2 with baseline and M1. Differences were considered to be statistically significant if p < 0.05.
Results
The descriptive statistics of the Sever’s disease pain VAS scores for the three measurements (baseline–M1–M2) are given. Table 1 lists the p-values for each of the comparisons. The differences were significant in all three comparisons, and the effect sizes of the changes were “large,” especially that between baseline and M1.
Descriptive data of the pain perceived by the participants and statistical significance of the comparisons and the corresponding effect sizes.
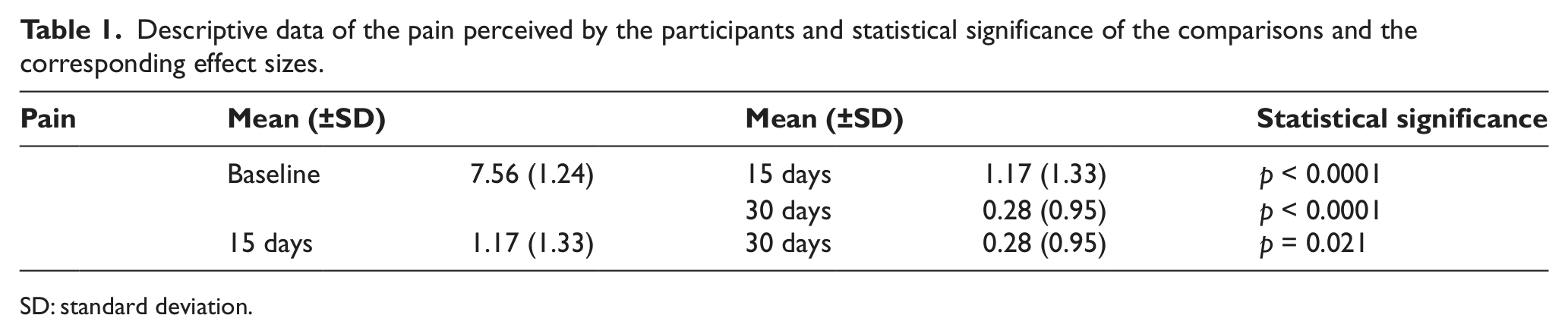
SD: standard deviation.
Discussion
The aim of this work was to describe an off-loading custom-made foot orthoses technique in general and how could be specifically adapted to treat Sever’s disease.
First, these orthoses could be an alternative to traditional custom-made and prefabricated orthoses used to treat foot misalignments. One of the advantages using this off-loading custom-made technique compared with prefabricated devices is that this technique combines a double correction in one device: a heel cup and a plantar arch support. In comparison with other custom-made orthoses, time used to manufacture them can be reduced. It can be supposed that manufacturing the insole directly on patient’s foot could lead to a better individual adaptation. However, time spent in manufacturing these orthoses is higher than in prefabricated devices, and also associated costs, so these disadvantages should be taken into account.
Second, this unloading custom-made orthosis showed good results in decreasing pain in patients suffering from Sever’s disease. Results suggested that using these orthoses could be an alternative in traditional treatments for Sever’s disease. Nevertheless, a control group was not included in the study, so the generalizability of the results should be interpreted with caution. Furthermore, we cannot conclude on whether this novel technique presents better results than prefabricated devices or other custom-made orthoses, so more investigations are needed.
Possible mechanisms by which the technique works can only be speculated. The relaxation of the Achilles–plantar-calcaneal system due to low-hardness heel raise reduces both the traction exerted by the Achilles tendon on its insertion onto the calcaneus and the plantar fascia tension, 13 which are implicated in the etiology of the disorder. 9 Indeed, various authors recommend this type of treatment exclusively.12,19,20
This same orthotic element also provides cushioning, reducing the impact on the calcaneus of heel strike forces. 12 Furthermore, the manufactured insole increases the foot’s contact surface (which is of interest since Sever’s disease has been associated with pes cavus 21 ) and acts to control the patient’s pronation (which has also been linked to the disease 22 ). Indeed, the non-load-bearing molding used to make the orthosis allows greater control of pronation since, before the midfoot structures collapse in the total stance phase of gait, the action is buffered by the smaller accelerations that the structures are subject to,23,24 thereby reducing the stress on the tissues and obviating their becoming damaged.
This is a preliminary study on DMOT to the non-load-bearing foot by vacuum in general and on its clinical application in Sever’s disease. This study could lead further investigations in this novel technique that should be focused on the inclusion of a control group and to compare the technique with other techniques that have shown good results in the decrease of Sever’s disease pain, such as heel cup plantar support, as well as a cost–benefit study.
Key points
Custom-made foot orthoses, fabricated with PVC and polyester resins combined with a 22 Shore A polyurethane heel cup, can reduce Sever’s disease pain.
This technique combines a double correction in one device: a heel cup and a plantar arch support and can lead to a better individual adaptation.
It means a reduction in time compared to other custom-made orthoses.
Footnotes
Conflict of interest
The authors declare that there exists no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.