
Abstract
Background:
The assessment of the maximum ankle dorsiflexion angle is an important clinical examination procedure. Evidence shows that the traditional goniometer is highly unreliable, and various designs of goniometers to measure the maximum ankle dorsiflexion angle rely on the application of a known force to obtain reliable results. Hence, an innovative ankle dorsiflexion measurement device was designed to make this measurement more reliable by holding the foot in a selected posture without the application of a known moment.
Objectives:
To report on the comprehensive validity and reliability testing carried out on the new device.
Methods:
Following validity testing, four different trials to test reliability of the ankle dorsiflexion measurement device were performed. These trials included inter-rater and intra-rater testings with a controlled moment, intra-rater reliability testing with knees flexed and extended without a controlled moment, intra-rater testing with a patient population, and inter-rater reliability testing between four raters of varying experience without controlling moment. All raters were blinded.
Study Design:
A series of trials to test intra-rater and inter-rater reliabilities.
Results:
Intra-rater reliability intraclass correlation coefficient was 0.98 and inter-rater reliability intraclass correlation coefficient (2,1) was 0.953 with a controlled moment. With uncontrolled moment, very high reliability for intra-tester was also achieved (intraclass correlation coefficient = 0.94 with knees extended and intraclass correlation coefficient = 0.95 with knees flexed). For the trial investigating test–retest reliability with actual patients, intraclass correlation coefficient of 0.99 was obtained. In the trial investigating four different raters with uncontrolled moment, intraclass correlation coefficient of 0.91 was achieved.
Conclusions:
The new ankle dorsiflexion measurement device is a valid and reliable device for measuring ankle dorsiflexion in both healthy subjects and patients, with both controlled and uncontrolled moments, even by multiple raters of varying experience when the foot is dorsiflexed to its end of range of motion.
Clinical relevance
An ankle dorsiflexion measuring device has been designed to increase the reliability of ankle dorsiflexion measurement and replace the traditional goniometer. While the majority of similar devices rely on application of a known moment to perform this measurement, it has been shown that this is not required with the new ankle dorsiflexion measurement device and, rather, foot posture should be taken into consideration as this affects the maximum ankle dorsiflexion angle.
Introduction
Proper ankle function, especially the dorsiflexion component, is essential for normal gait. 1 When there is limitation of ankle dorsiflexion, important clinical manifestations occur, with repercussions ranging from mild musculoskeletal symptoms, such as metatarsalgia, heel pain, and nerve entrapment, to gross deformity requiring surgical intervention. The effects of limited ankle dorsiflexion, or in more severe cases, ankle equinus, are well documented in the various patient populations, including diabetics 2 and adolescent athletes. 3
A diagnosis of ankle equinus or limited ankle dorsiflexion is arrived at after measuring the dorsiflexion angle. From this, important clinical decisions, such as prescription of functional foot orthoses or whether to intervene surgically, are reached. Notwithstanding this, however, there are clear issues regarding the reliability of techniques used to measure ankle dorsiflexion. Although, traditionally, ankle dorsiflexion is measured with a goniometer, there is overwhelming evidence that this technique’s inter-rater and intra-rater reliability is very poor,4–8 without increasing with rater experience. 9 For this reason, various types of goniometers have been designed to overcome the range of problems associated with this measurement.10–16 A number of factors that may affect the ankle dorsiflexion angle measurement has been identified, including foot posture and the amount of torque (or moment) applied to the forefoot to dorsiflex the foot. 17 Hence, it must be determined whether these factors, which form the basis for the design criteria of an ankle dorsiflexion measurement (ADM) device, have been addressed by these devices.
One has to differentiate between “ankle dorsiflexion” and “foot dorsiflexion,” as the latter involves the dorsiflexion at ankle, subtalar joint, and midtarsal joint. 17 Midtarsal joint movement has been shown to be quite significant, often averaging more than ankle joint movement itself; 18 measurement results arising from this situation would clearly lead to a misdiagnosis in which limited ankle dorsiflexion could be masked by midtarsal joint movement.
In a kinematic analysis of sagittal foot segment movement during passive dorsiflexion, it was reported that there is always more forefoot movement than hindfoot movement, that the forefoot to hindfoot angle increases as the moment increases on the forefoot, and that forefoot movement cannot be eliminated completely irrespective whether the foot is placed in the neutral, supinated, or pronated position. The theory has been put forth that those devices measuring across the forefoot (such as the traditional goniometer and those devices using a foot plate) are actually measuring the summation of ankle and forefoot movement (“foot dorsiflexion”) and not ankle joint dorsiflexion. 19
It is imperative that during ankle dorsiflexion angle measurement, due importance is given to foot posture as there is a significant difference between the three postures. Three studies have shown that the pronated foot results in significantly more dorsiflexion (8°–10°) than the other postures.19–21 On the other hand, research has shown that the clinical significance of the difference between the neutral and supinated postures may be quite low, ranging between 2.5° 19 and 3.5°. 20 Doubts as to whether this difference would affect a clinical decision or whether it would be even detectable using normal clinical goniometric measurements have been presented. 19 Even though foot posture may have a profound effect on the maximum foot dorsiflexion angle, a number of trials investigating reliability of new goniometer designs do not take foot posture in consideration at all.
The application of a known moment is another important factor. Goniometers designed to measure ankle dorsiflexion have controlled the amount of moment applied to the forefoot, which ranged from 10 to 25 N m.10–12,14–16,22,23 This has in fact made it easier for the goniometers to produce similar results when repeatability was investigated. However, during clinical measurement, it is doubtful how many practitioners carry a force gauge with them, so this solution is clearly impractical. Research has demonstrated that it is possible to get results with no significant differences without using a force gauge but with measurements taken at a slightly supinated position. 24 It has been postulated that since there is no clinical significant difference between the neutral and supinated postures, with the difference amounting to just 2.5°, this test can be performed at this position, thus circumventing issues with reliability of establishing subtalar joint neutral position that is notoriously difficult to achieve for many clinicians, especially those of little experience, as originally recommended. 20
Since foot posture affects the maximum dorsiflexion angle to such an extent, clinical implications include an inability to compare results between practitioners and between preinterventional and postinterventional measurements once foot posture is not taken into consideration.
A new ankle dorsiflexion measurement device
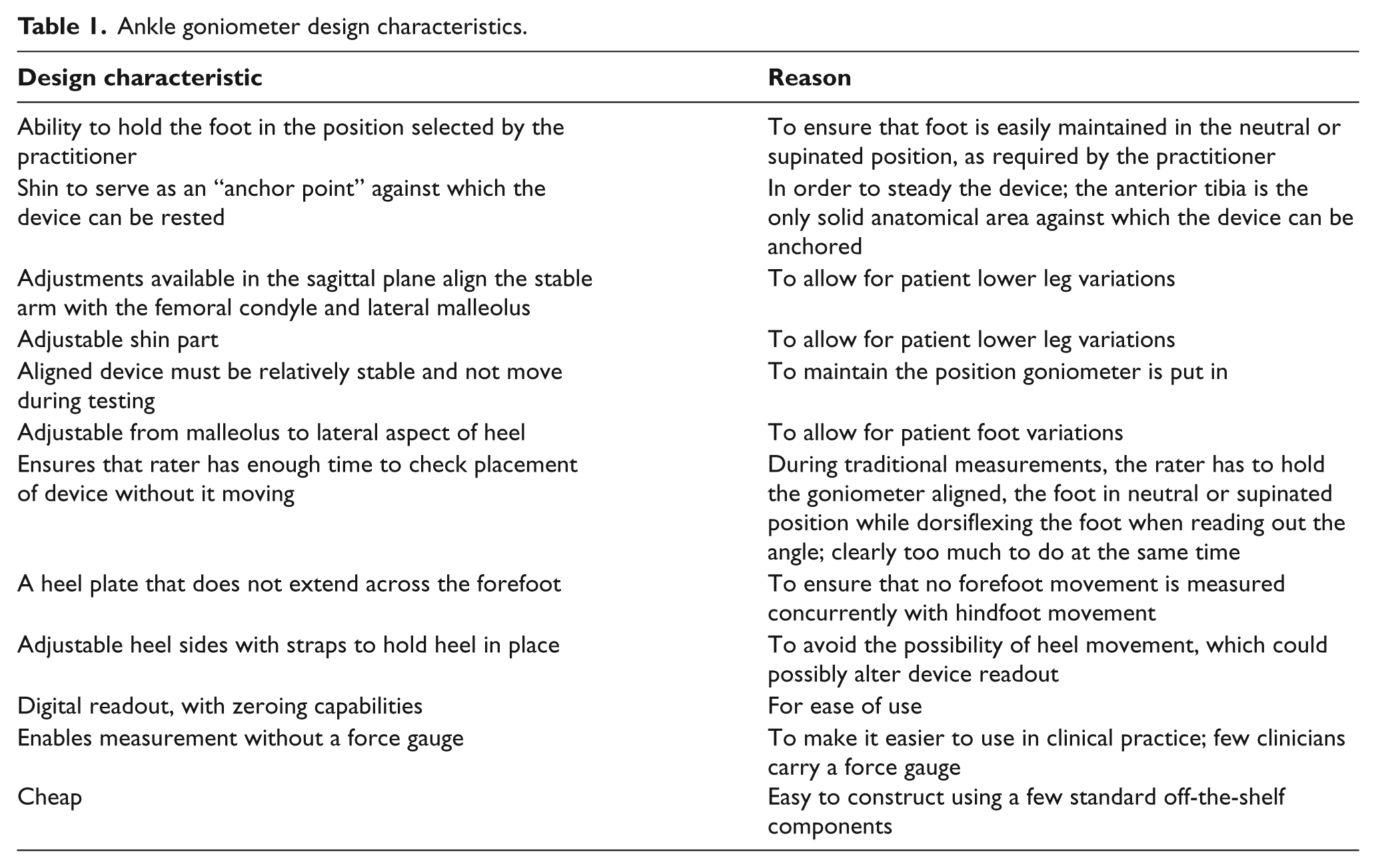
The need for a new ADM device (Figure 1(a) and (b); Table 1) becomes apparent when one considers the lack of regard to these factors given by many goniometer designs. Thus, the aim of this final product was to produce a goniometric device designed specifically to measure ankle dorsiflexion in a reliable manner, achieved using a technique that would be available to every clinician. When set up and aligned with the lateral condyle of the fibula and lateral malleolus, its axis placed in line with the axis of the ankle joint and the foot locked in the required position (whether subtalar joint neutral or supinated, as required by the practitioner), the rater only has to apply a dorsiflexing force against the forefoot without the device moving out of position. Thus, important features of this device, besides being relatively cheap to produce, include the ability to lock the foot in a predetermined posture, to hold the heel tightly in an adjustable, padded heel cup, and to enable adjustment in any plane as may be necessary in order to align the device with the various anatomical landmarks.

(a) Schematics for the ankle goniometer and (b) the ankle goniometer in place.
Ankle goniometer design characteristics.
Reliability
Any new diagnostic device requires reliability testing to be performed. Reliability has been defined as “the consistency or reproducibility of a measure.” 5 Test–retest, inter-rater and intra-rater reliability testing are required when evaluating new apparatuses designed to measure ankle dorsiflexion. The majority of trials assessing reliability of ankle dorsiflexion devices have used this type of testing, with test–retest designs being the preferred method of assessment, further statistically analyzed by intraclass correlation coefficient (ICC). 17
A quality methodological assessment on 10 devices designed to measure ankle dorsiflexion has reported quite poor scoring of some of these devices because of a number of factors, including small convenience samples, lack of use of actual patient populations to test out the devices, lack of randomization reporting, and lack of comparison to a “Reference Standard,” that is, comparison to a test that is known to produce valid results. It is, however, recognized that this gold standard may be x-rays and the authors may encounter problems obtaining ethical approval purely for research purposes. 17 Wilken et al. 12 have circumvented this problem using an optoelectronic motion analysis system to simultaneously evaluate 12 participants together with their Iowa Ankle Range of Motion (IAROM) device. 12
Methods
Validity and reliability testing for the ADM Device spanned a number of different phases. Ethical approval was granted by the University Ethics Committee.
Validity testing
Validity testing (comparing to a reference standard) was carried out simultaneously with an eight-camera Vicon optoelectronic motion capture system (Oxford Metrics, UK), sampling at 100 Hz. As the ADM device has an optical digital readout (liquid crystal display (LCD) screen) and could not be synchronized directly to the Vicon system, it was initially coupled and calibrated with an electrogoniometer (MIE Medical Research Ltd, Leeds, United Kingdom), so that the two devices readout the same angle. The electrogoniometer in turn was interfaced with the Vicon system through a Tekscan (Boston, MA, USA) triggering box. A hindfoot model was constructed in Visual 3D (C-Motion, Germantown, PA, USA), and reflective markers were placed on the hindfoot (Figure 2). The subject was instructed to dorsiflex his foot in 5° stages, which angle could be read from the laptop screen of the electrogoniometer interface, simultaneously capturing data with the Vicon system. Five trials were carried out. Readouts from the two devices are reproduced in Figure 3. Statistical analysis produced a Pearson’s coefficient of 0.996, with correlation being significant at the 0.01 level (two-tailed), p = 0.000.
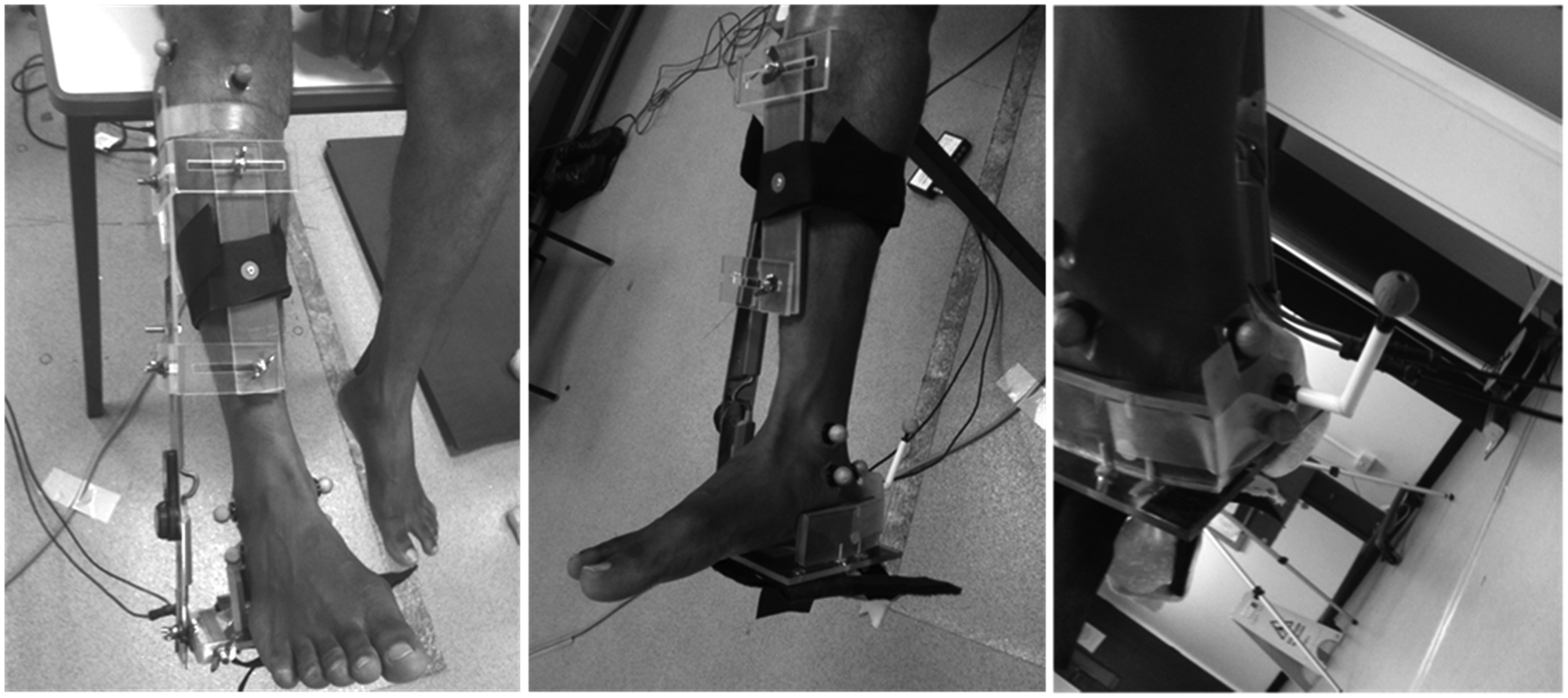
Ankle goniometer and reflective marker placement.
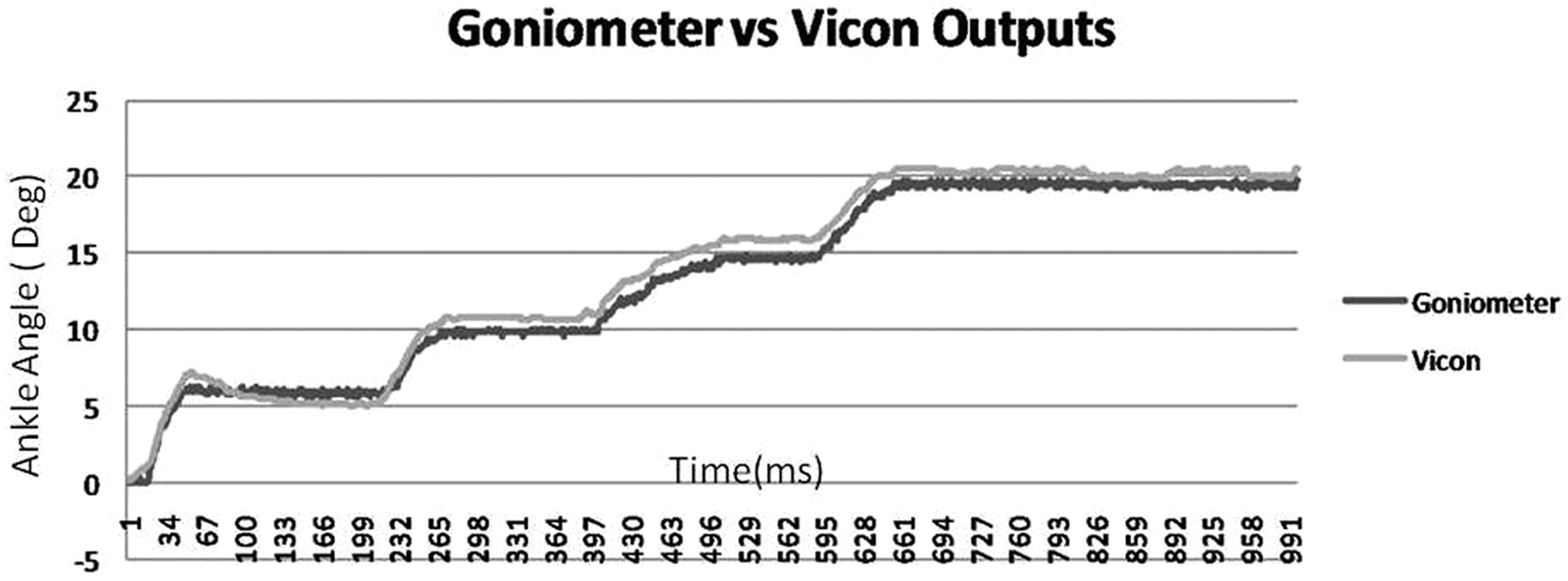
Comparison between goniometer and Vicon outputs.
Reliability testing
In order to establish whether the ADM device was suitable for clinical and research uses, comprehensive reliability testing was performed. This testing took the form of various trials in order to encompass as large a subject variation as possible, with both participants and raters being blinded and an independent observer taking down the angles output by the ADM device. Power calculation revealed a minimum sample size requirement of 34 participants (actual power = 0.808).
Trial 1: inter-rater and intra-rater test–retest reliability using a known moment
A convenience sample of 10 healthy adults (mean age = 18.9 years, range = 18–20 years) were assessed by two raters. Both raters were experienced clinicians, however with very little clinical experience in the use of the specific ADM device. Rater 2 had just 15 min acclimatization with the instrument after its layout and technique for use were explained by Rater 1.
All measurements were performed with the participants in a supine position. Rater 1 applied the goniometer to the participant, aligning the lateral arm to the femoral condyle and lateral malleolus, the pivot point of the instrument in line with the malleolus and firmly clasped the heel in the adjustable heel portion of the device. The foot was then placed in a slightly supinated position using the talonavicular congruency method. The talar head was palpated with index finger and thumb of the rater’s right hand until subtalar joint neutral position was identified by feeling equally the medial and lateral heads of the talus, then supinating slightly so that only the lateral aspect of the talar head was palpable. This position, previously recommended in the literature, 20 was chosen as previous research had indicated a nonclinical difference between the neutral and supinated positions of only 2.5°, 19 thus bypassing issues regarding consistent finding of subtalar joint neutral. The rater then applied 20 N m of force to the forefoot through a calibrated force gauge to dorsiflex the foot maximally for 3 s and then released the applied force. A reporter recorded the maximum ankle angle when the rater announced that 20 N m was applied.
This procedure was repeated five times, for all participants, by both raters (inter-rater reliability assessment). Rater 1 then repeated the whole performance after 1 h (intra-tester reliability). Same day repeatability was chosen in order to exclude any factors that could influence the maximum dorsiflexion angle, such as soft tissue stretchability factors of the triceps surae.
Trial 2: intra-tester, test–retest reliability with uncontrolled force
10 healthy adults (four males, six females, mean age = 40.3 years (33–48 years); mean weight = 77.8 kg, mean height = 167.9 cm) were recruited in order to undergo intra-rater reliability testing without the use of an applied controlled moment. Rater 1 assessed all participants, who were lying supine. As previously done, a dorsiflexing force was applied to the forefoot until the maximum dorsiflexion angle was attained, at which point the angle was recorded by an independent observer, keeping both rater and participant blinded. Following five dorsiflexion measurements, the knee was flexed by approximately 20°, to eliminate the effect of the gastrocnemius muscle, and then the routine was repeated. For test–retest reliability purposes, the whole procedure was repeated after 1 h.
Trial 3: intra-tester, test–retest reliability with uncontrolled force on a patient population
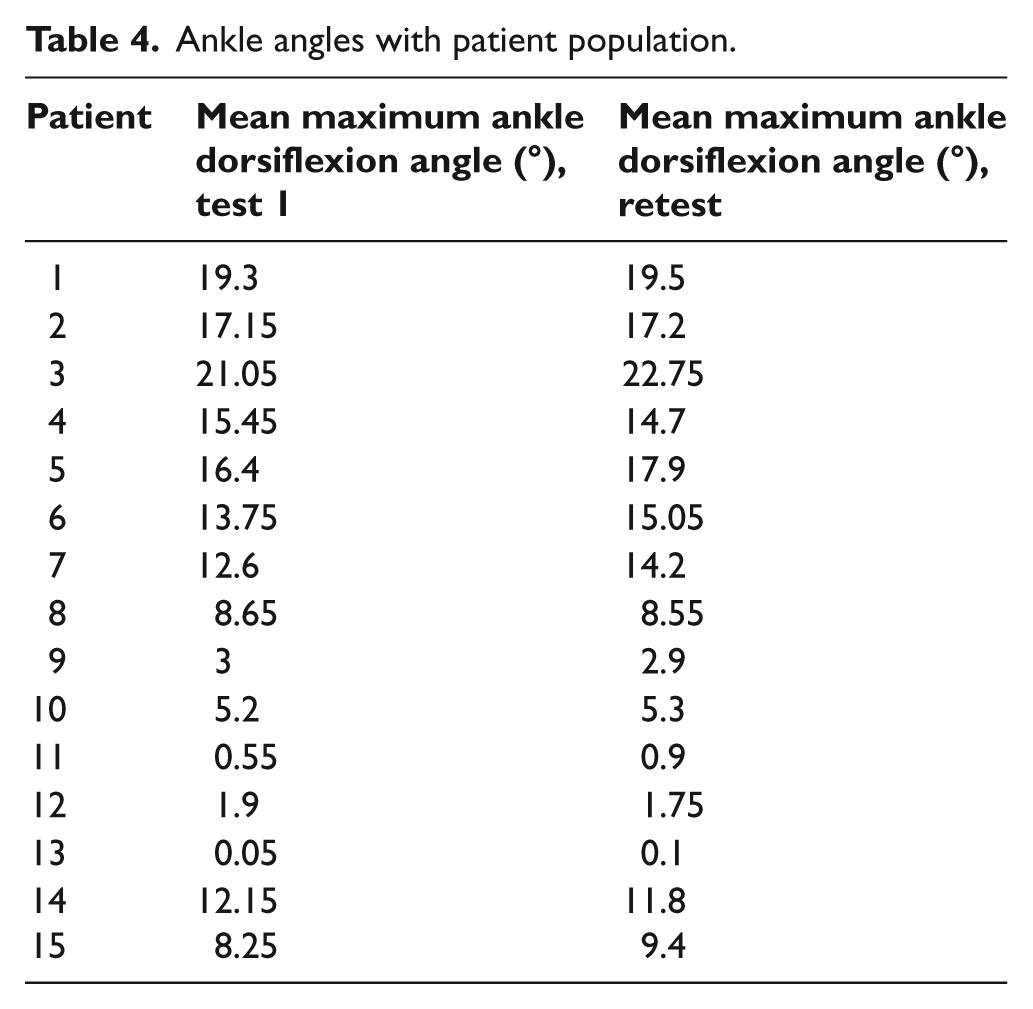
The first 15 patients (10 females, 5 males, mean age = 46.6 years (19–72 years), mean height = 166.4 (158–185 cm)) attending a musculoskeletal clinic were invited to participate. The main criterion was a foot condition that could be possibly related to altered ankle function, or that could possibly alter ankle function (Table 2 for subject demographics). Following the previous protocol, a single rater assessed maximum ankle dorsiflexion on all participants. This time, however, the number of repetitions was reduced to just 2 instead of 5 so as not to cause any undue pain to the participants. The second ratings were done after 1 h.
Participant demographics.
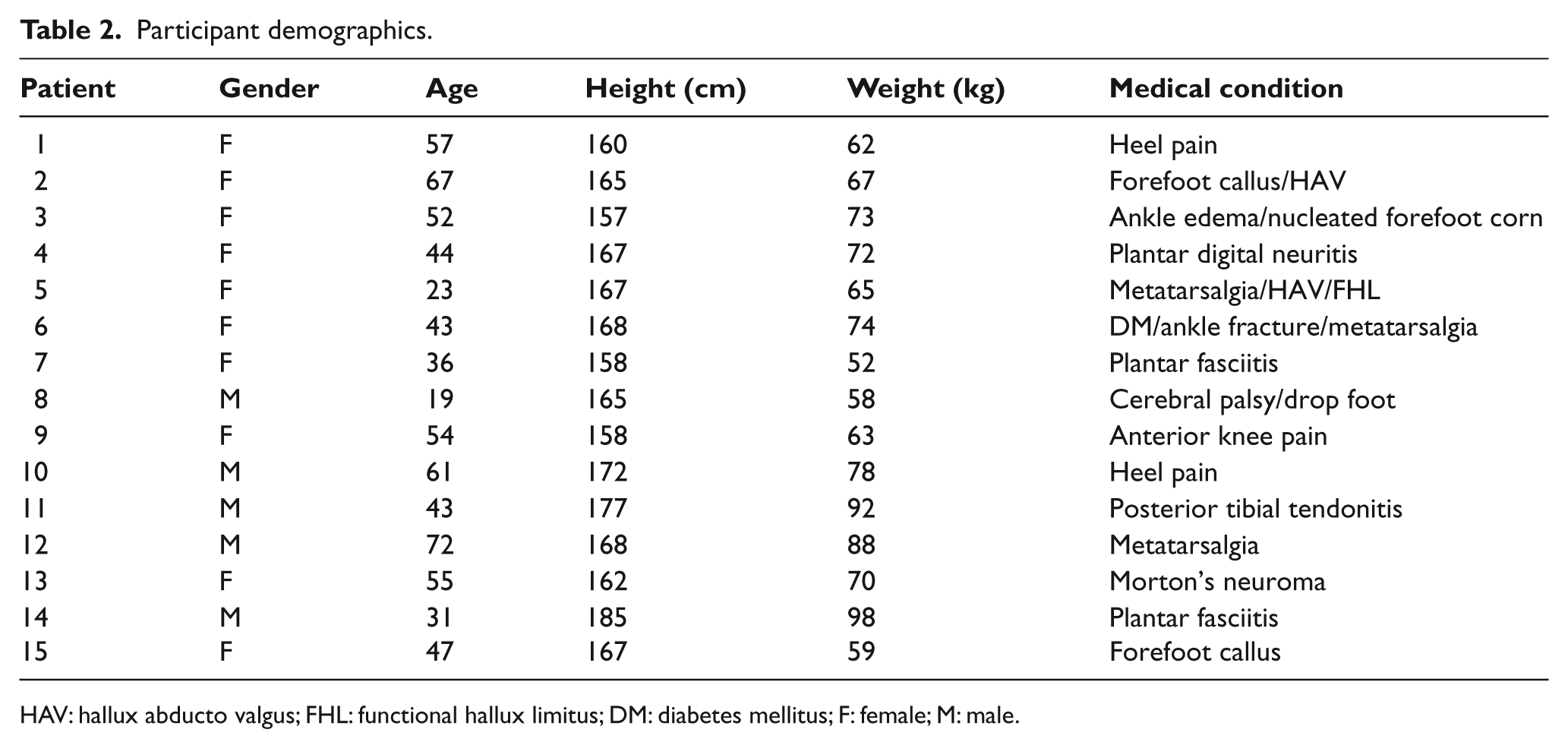
HAV: hallux abducto valgus; FHL: functional hallux limitus; DM: diabetes mellitus; F: female; M: male.
Trial 4: reliability with multiple raters with uncontrolled moment
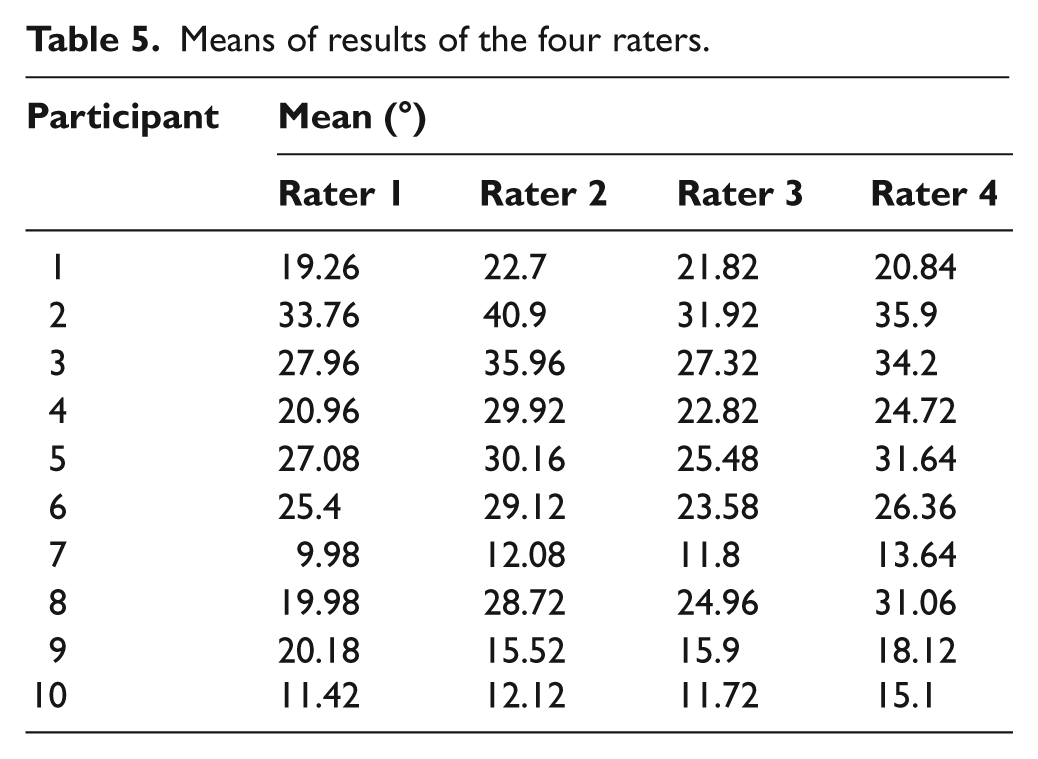
Two female and two male practitioners with varying experience in the use of the ADM device assessed a convenience sample of 10 adults (five males, five females, mean age = 36.4 years (26–51 years)) using the previously validated ADM device. Two of the practitioners had never used this type of goniometer before and were instructed about its various characteristics and usage by the first practitioner. Each participant lay supine and told to relax, following which the goniometer was applied to the right foot, which was established in a slightly supine posture using the talonavicular congruency method. At this position, the head of the talus on the lateral aspect could be palpated while the medial head could not. A moment was applied at the ball of the foot until the foot was dorsiflexed maximally. An observer noted the angle on the digital scale of the goniometer. All raters and participants were blinded to the resultant angle. Five iterations were performed by each practitioner, with a 30 s pause in between. Participants were not removed from the goniometer, 25 since the aim was to assess the consistency of the angle produced. Each participant was then rated by a different rater until all raters had performed the required measurements. The order of raters was determined randomly by the observer so that the practitioner sequence differed with each participant.
There were no inclusion or exclusion criteria, since this device is meant to be utilized as a diagnostic tool. However, all participants were healthy consenting adults with no systemic disease and no apparent deformities of the feet.
At the end of the whole trial, the independent observer handed in the final readings in an excel spreadsheet. Data were then analyzed with SPSS 19.0.
Results
Trial 1
The maximum ankle angles as output by the ADM device are presented in Table 3. Rater 1 (test) and Rater 1 (2) (retest) were compared for intra-rater reliability, while Rater 1 and Rater 2 angles were utilized for statistical analysis of inter-tester reliability. Intra-rater reliability, which is the test applied to assess consistency or reproducibility of quantitative measurements made by different observers measuring the same quantity, resulted in an ICC (2,1) of 0.98 (p = 0.000). ICC (2,1) implies a two-way random effects model where both people effects and measures effects are random.
Rater 1 (test–retest) and Rater 2 maximum ankle dorsiflexion angles.
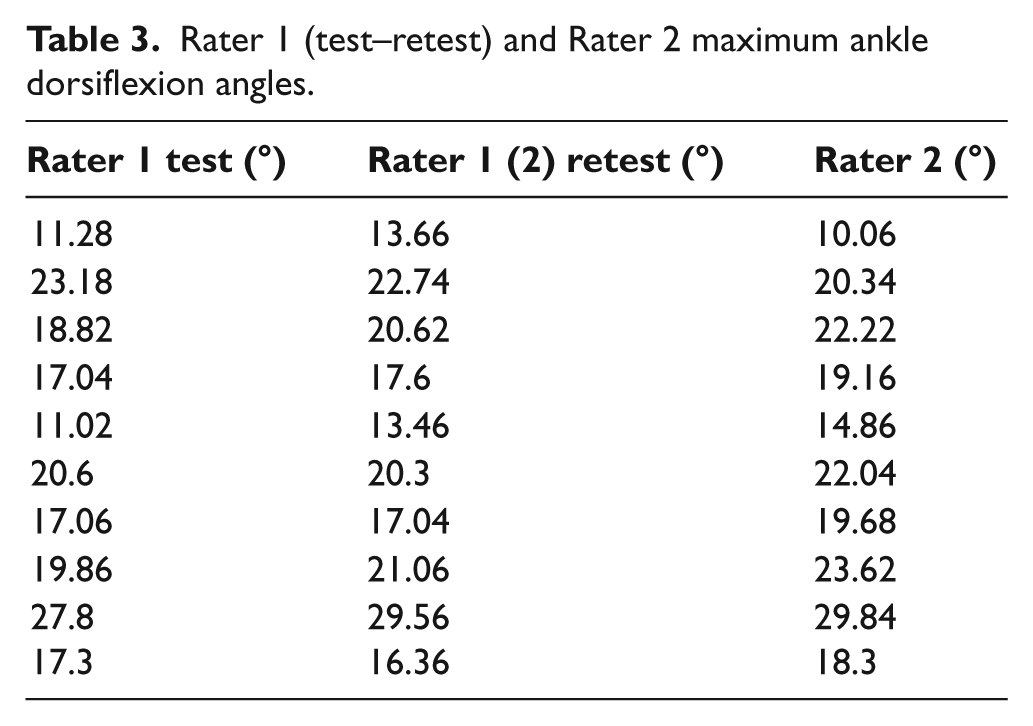
Inter-rater reliability, that is, reliability between Rater 1 and Rater 2, ICC (2,1) was 0.953, with angular means <2°, demonstrating very high reliability between the two raters. Statistical significance of 0.000 was also achieved.
Trial 2
Even though moment was not controlled in this trial, very high reliability for intra-tester was achieved (ICC = 0.94 with knees extended and ICC = 0.95 with knees flexed).
Trial 3
For this trial investigating test–retest reliability with actual patients, ICC of 0.99 was achieved (p = 0.000) (actual angle results in Table 4).
Ankle angles with patient population.
Trial 4
The mean maximum ankle angles by the four raters are presented in Table 5. An ICC of 0.91 was achieved.
Means of results of the four raters.
Discussion
Although the ankle dorsiflexion angle is such an important component of the clinical examination of the foot, there is still a lack of a standardized method of assessing this angle. Lack of reliability of the normal goniometer has been established through various trials, to such an extent that it clearly should not be utilized for clinical and research uses. This consequently creates a need for the development of a suitable device to replace the traditional goniometer (or tractograph); a challenge taken up by various specifically designed appliances that, however, seem not to suitably address some of the important issues involved in this apparently simple act of measuring ankle dorsiflexion, which are foot posture and the amount of moment applied to dorsiflex the foot.
If, as quoted in the majority of studies relating to goniometric measurement of ankle dorsiflexion, the amount of moment applied is such a determinant factor on the ankle angle produced, this assessment procedure would have poor inter-tester reliability if moment is not controlled, since different practitioners are likely to induce different amounts of force during this procedure. It would thus be quite difficult to investigate treatment effectiveness in a preintervention and postintervention scenario, for example, or to compare results between different practitioners or different trials. Using an optoelectronic motion analysis system, it has been demonstrated that the maximum ankle angle can be quite reliably assessed by the same practitioner (intra-tester reliability). Although the application of a known moment produced reliable inter-rater results, it has also been shown that the same rater can produce reliable results when not controlling for moment.
Yet, although foot posture affects this angle, the amount of force applied to dorsiflex the foot does not affect, provided that end of range of motion is achieved. Notwithstanding this, in various trials that investigate maximum ankle dorsiflexion, the applied moment is given more attention than foot posture.
Although moment is important for the calculation of a passive torque versus angular displacement curve, 15 it has been postulated that since maximum ankle dorsiflexion is an end of range of motion assessment determined by the stretching characteristics of the triceps surae, applying more force beyond the stretching limit would cause tendon damage. Consequently, further application of force beyond this limit should be avoided. 24
All the testing of the ADM device was carried out with the foot in a slightly supinated posture to reduce possible errors associated with finding subtalar joint neutral since it has been reported that there is a clinically insignificant difference in the angles between the two postures.
The ADM device is an inexpensive device aimed at increasing the reliability of ankle angular measurements, an aim that has been clearly achieved following extensive validity and reliability testing. Its reliability stems from various factors, including exclusion of the forefoot in the measurement procedure by shortening the foot plate into a heel plate, by its ability to be held securely, by proper alignment to various easily evident lower limb landmarks, by locking the foot into the posture it is placed in, and by holding the heel tightly with an adjustable heel part.
It has been shown that the ADM device and a kinematic hindfoot model based on an eight-camera optoelectronic motion capture system produce similar results for the range of passive ankle dorsiflexion. Clearly, the advantages of using such a device over the motion capture system are various, especially where expense and expertise required to use the two systems are concerned; the latter involves a whole infrastructure for its use, including a specialized lab, specialized personnel, a significant amount of time for calibration, marker placement, and data collection and interpretation. On the other hand, the ADM device can be easily used in any clinical/research situations once set up.
Findings from the various trials imply that the new ADM device can be used with no difference in reliability with controlled and uncontrolled moment.
Conclusions
The ADM device is a valid and reliable device for measuring ankle dorsiflexion in both healthy participants and patients, even by multiple raters of varying experience when the foot is dorsiflexed to its end of range of motion. Testing with uncontrolled moment is as reliable as when moment is controlled; thus, there is no need to use a force gauge when measuring the maximum ankle dorsiflexion angle. The angles output by the device are comparable to those output by an eight-camera optoelectronic motion capturing system. Thus, the ADM device can be reliably used for both clinical and research purposes.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.