
Abstract
Background:
Most posture problems encountered in persons who use wheelchairs in a seated posture for extended periods are related to sacral sitting due to posterior pelvic tilt. Posterior pelvic tilt places pressure and shearing force on the sacrococcygeal area that can lead to pressure ulcers, but the relationship between pelvic tilt and force applied to the sacrococcygeal and ischial tuberosity areas has not yet been investigated.
Objective:
To investigate the relationships of posterior pelvic tilt in a seated posture with vertical force and horizontal force on the sacrococcygeal and ischial tuberosity areas.
Study Design:
Repeated measures design.
Methods:
Thirty male and female subjects aged ≥60 years sat in a measurement chair at varying pelvic tilt angles, and force on the sacrococcygeal and ischial tuberosity areas was measured.
Results:
The pressure on the sacrococcygeal area increased with pelvic tilt in all subjects, with vertical force averaging 19% of the body weight at a pelvic tilt angle of 30°. The horizontal force on the sacrococcygeal area increased in 93% of the subjects, with an average increase equal to 3% of the body weight.
Conclusions:
We confirmed changes in vertical and horizontal forces on the sacrococcygeal and ischial tuberosity areas with a change in seated posture (pelvic tilt).
Clinical relevance:
We propose guidelines for rehabilitation practitioners working with wheelchair users to suggest improved ways of sitting in wheelchairs that avoid pelvic tilt angles that might promote pressure ulcers on the buttocks.
Background
Most posture problems in persons who use wheelchairs in a seated posture for extended periods are related to sacral sitting and pelvic inclination. 1 Of these, the most commonly encountered is sacral sitting due to posterior pelvic tilt. In comparison with the ischial tuberosity region, which features a considerable amount of surface soft tissue to support body weight loading, the sacral area, by nature, is not pressure resistant, and body weight loading can lead to pressure ulcer development. 2
There is currently disagreement between researchers regarding specific threshold values at which pressure presents the risk of pressure ulcer development, 3 but Drummond et al. 4 suggest that there is pressure ulcer risk when pressure on the sacrococcygeal area exceeds 11% of the body weight, based on sitting pressure distributions in 16 patients with paraplegia (9 with pressure ulcer and 6 without).
Collins 5 has shown that posterior pelvic tilt generates friction and shearing force on the sacral area. The National Pressure Ulcer Advisory Panel (NPUAP) defines “shear” as “an action or stress resulting from applied forces which causes or tends to cause two contiguous internal parts of the body to deform in the transverse plane.” 6 Such forces in combination with pressure can result in decreased blood flow and pressure ulcer development.7 –10
Furthermore, Lahmann et al. 11 investigated the causes of pressure ulcer in 17,666 residents of 234 long-term care facilities and found that “the existence of ‘friction and shear’ as a potential and especially as a manifest problem has had the strongest association with pressure ulcer prevalence.” In other words, pelvic tilt that causes pressure and shearing force on the sacrococcygeal area in seated posture is closely associated with pressure ulcer development.
NPUAP guidelines 12 recommend that consideration be given to seated posture to prevent pressure ulcer formation, but there remains a need for discovering a seated posture that reduces pressure and shearing forces, thereby reducing the risk. Goossens et al. 13 has reported on the relationship between seat cushion tilt and the shearing force that results at the bearing surface, but the relationship between posture and shearing force on the buttocks remains unclear. Although the importance of a safe and comfortable seated posture is widely recognized, such general recognition has resulted in relatively little quantitative research on posture.
There have been several reports from Koo et al. 14 and Burke et al. 15 on pelvic inclination in the frontal plane. In research on the relationship between posture and shearing force in the sagittal plane, Hobson 16 considered nine posture changes in 12 participants with spinal cord injury and 10 participants without disabilities to examine how such changes affect pressure and shearing force. However, shearing force measurements were performed between seat cushions and wheelchairs, and measurements taken closer to the body are likely needed. Aissaoui et al. 17 reported on changes in the pressure and sliding in 10 participants without disability when tilt and reclining angles were altered among 12 positions. Note that here, shear was reported not as force but as distance.
It is important that therapists and caregivers use pelvis alignment as a guideline when evaluating the seated posture of wheelchair users in hospitals and clinics. Knowledge of how pelvis alignment is related to pressure and shearing force is therefore vital for proposing a safe seated posture.
This study aims to articulate how pressure and shearing force on the ischial tuberosity and sacrococcygeal areas change with pelvic tilt in a seated posture and to test the following hypothesis: Changes in seated posture (posterior pelvic tilt) are accompanied by changes in the level of pressure and shearing force on the ischial tuberosity and sacrococcygeal areas.
In the ischial tuberosity and sacrococcygeal areas, which are sites prone to pressure ulcer development in seated postures, there are likely differences in the pressure and shearing force that occur due to posture. It is therefore preferable to measure pressure and shearing force separately as well as simultaneously in those areas. A system for simultaneous measurement of pressure and shearing force has been reported, 16 but the reported method does not allow for separate measurement of the ischial tuberosity and sacrococcygeal areas. Accordingly, we have developed a customized measurement device.
Methods
Force sensors
An ischial tuberosity area plate and sacrococcygeal area plate were used as sensors for measuring the vertical force and horizontal force in those areas. Previous pressure measurements in wheelchairs have used sensor sheets, 18 but we developed a new measurement apparatus because (1) pressure sheets do not allow for separate measurement of the ischial tuberosity and sacrococcygeal areas, (2) the presence of a foreign object between the cushion and the patient could result in decreased measurement accuracy, and (3) hard objects are more appropriate for measurement. 19 Figure 1(a) and (b) shows a schematic of the force plates and sensor placement, respectively. Figure 2(a) to (c) shows the photographs of an actual sensor unit.
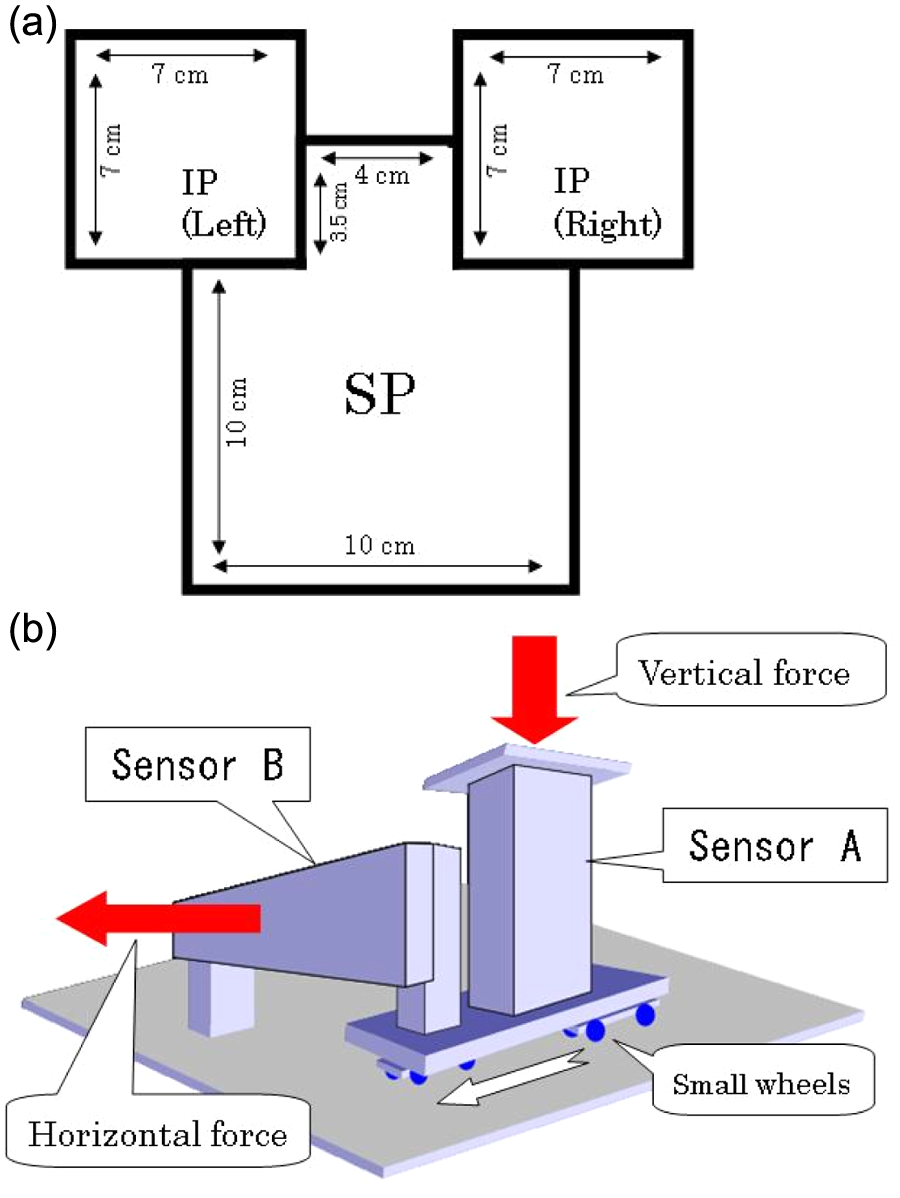
(a) Design of the SP and IP. (b) Sensor placement. The vertical force sensor (sensor A) was a load cell (LC1122-K050; A&D Company Ltd., Tokyo, Japan) rated for 500 N (51 kgf), with system accuracy of 0.04% rated output. When vertical force is applied to the plate, small wheels affixed below the sensor make contact with a floor plate, and vertical force is measured. The horizontal force sensor (sensor B) is a load cell (C2G1-30K-A; Minebea Co. Ltd., Nagano. Japan) rated for 294 N (30 kgf), with system accuracy of 0.03% rated output. One side of sensor B is affixed to a floor plate via a strut, and the opposing side is connected via a strut to the wheels supporting sensor A. When forward or rearward horizontal force is applied to the IPs and SP, the wheels supporting sensor A move and sensor B bends to measure the horizontal force.
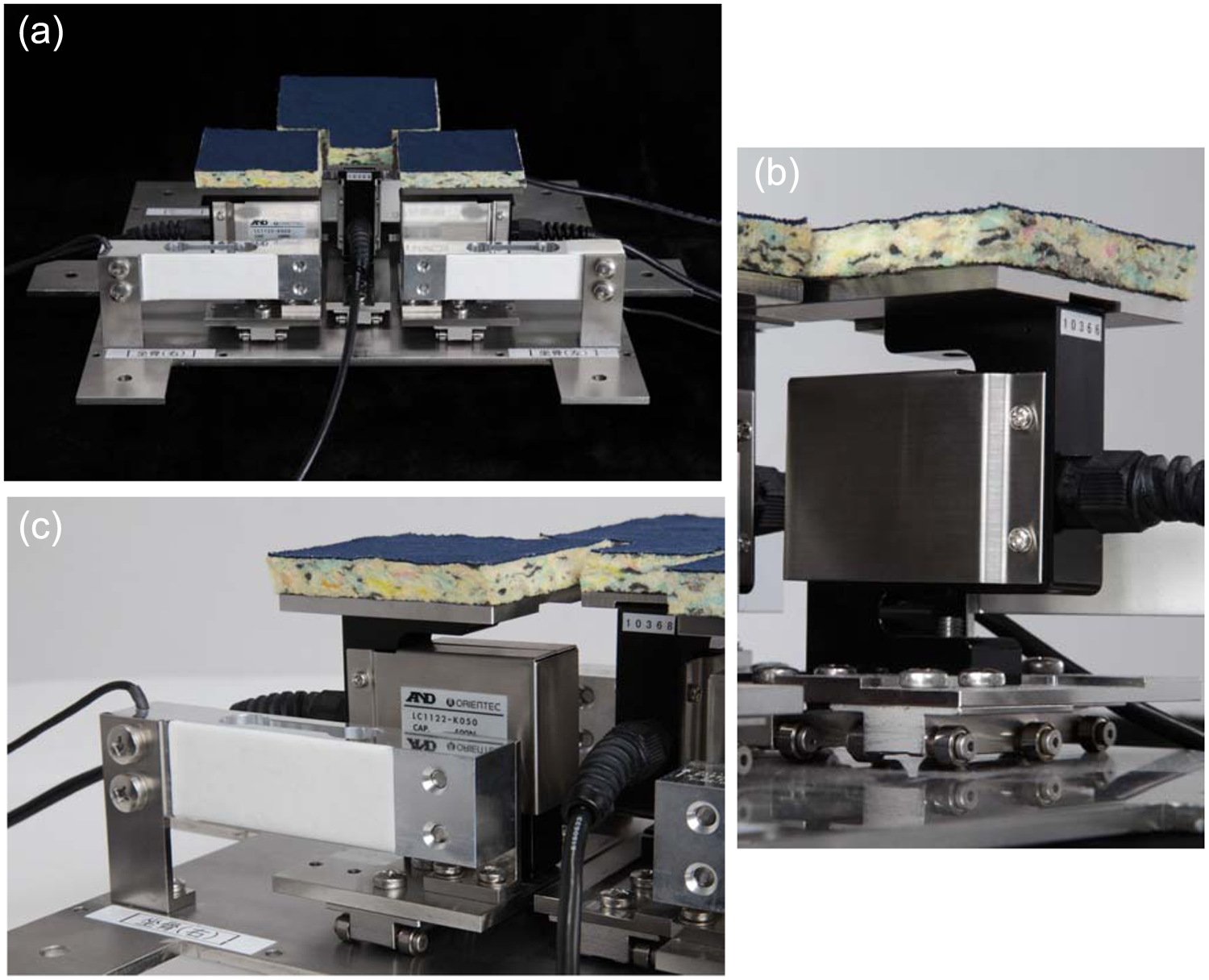
(a) Sensor configuration (inner view of sensor unit), (b) sensor A (right ischial plate), and (c) sensor B (right ischial tuberosity plate).
The sacrococcygeal area plate size was determined from measurements of 55 sacrum bone specimens. Measured specimens were 10.7 ± 1.1 cm tall and 10.4 ± 0.7 cm wide. The sacrococcygeal plate, therefore, covered a 3.5 × 4-cm coccyx region measurement area and a 10 × 10-cm sacrum bone measurement area, sandwiched between the left and right ischial tuberosity plates to form a convex shape.
To determine the appropriate size for ischial plates, we used 11 cadavers (3 males and 8 females, average age 79.1 ± 10.9 years) used for anatomical studies at Iwate Medical University to make 22 width measurements of ischial tuberosity nodes. Measurement results were 28.1 ± 1.4 mm, so we took the width of ischial tuberosity nodes as 3 cm, and the spacing between left and right ischial tuberosities as 7 cm2 to accommodate participants between 8 and 15 cm. The sacrococcygeal and ischial plates can move freely and are separated by 5 mm to prevent mutual interference.
We covered the surface of the seat containing the sacrococcygeal and ischial tuberosity plates with a 1-cm-thick urethane sponge of medium hardness to simulate as closely as possible an actual cushion. The urethane sponge was split and affixed to the sacrococcygeal and ischial tuberosity plates to prevent interference with free movement. After assembling the sensors and plates of the measurement apparatus, we performed validity testing to confirm measurement accuracy. Weights were used to place vertical and horizontal force on the left and right sacrococcygeal and ischial tuberosity plates, and measurement apparatus precision was calculated according to the coefficient of correlation between the ratio of measurement values (values measured by the measurement apparatus) and actual values (values measured according to the weights).
Vertical force values were verified by using 0, 0.5, 1, 5, 10, 15, and 20 kg weights. Horizontal force values were verified by using 0, 0.5, 1, 2, 3, and 5 kg weights. The measurements were performed by hanging weights from a small pulley. The results indicated a coefficient of correlation of 1.0 (at 1% significance) for all measurements in the vertical and horizontal directions, confirming the validity of the developed measurement apparatus.
Force measurements
Participants
Participants were 15 men and 15 women (age: 71.8 ± 5.7 years, height: 154.0 ± 8.4 cm, and weight: 53.6 ± 9.5 kg) who had been admitted to hospital for limb fracture, stroke, or treatment for illness. The participants were selected following simple interviews and palpations according to the following criteria: the participants were at least 60 years old and had the ability to maintain a stable seated posture in a wheelchair without arm supports. Furthermore, the participants were required to have no apparent cognitive disorder that would hinder understanding of verbal instructions related to maintaining a posture at a specified pelvic angle when the measurement was performed. Exclusion criteria were ailments that could be exacerbated by participation in the experiment, sensory disorder of the buttocks, cognitive impairment, and poor pelvic mobility.
This study was approved by the 2009 ethics committee of Iwate Medical University School of Medicine, and written consent was obtained from the participants. In the experiment, the participants received verbal explanation of actions to be performed based on a written script.
Testing method
The participants sat on a chair in which the sensors were embedded, and after manual confirmation that the ischial tuberosities were in contact with the left and right ischial tuberosity plates, the position of the chair depth and back support were adjusted. Pelvic tilt angles were set by using a HORIZON posture measurement instrument (KS08010; Yuki Trading Co. Ltd, Tokyo, Japan; Figure 3) to 0°, 5°, 10°, 15°, 20°, 25°, and 30° in turn, and the measurements were performed at each angle. Pelvic tilt was measured by using the anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS) as landmarks, following the ISO 16840 standard for wheelchair seating. 20 The HORIZON device’s arm tip was placed in contact with participants’ right ASIS and PSIS, and the tilt angle of the pelvis was measured with respect to the horizontal. The measurements were performed three times for each pelvic angle, and the average of those measurements was taken as the measurement value.
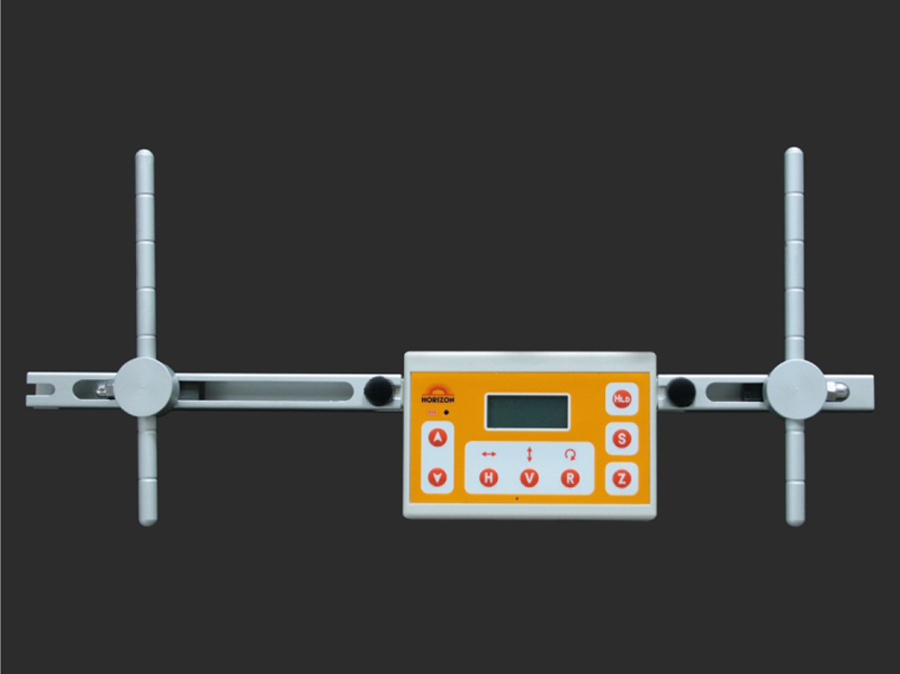
HORIZON posture measurement instrument. The HORIZON instrument allows measurement of tilt angles in relation to the direction of gravity or rotation in space using two arbitrary points (e.g. rotation of the trunk with respect to the pelvis) by placing the tips of the right and left arms on body landmarks. Tilt angle measurements are performed using a piezoresistive three-axis acceleration sensor. A gyroscope allows measurement of the rotation angle in the horizontal plane.
The chair used for measurements had a structure allowing for depth and height adjustment to conform to the participant’s body dimensions. Furthermore, the back support included a tension-type adjustment mechanism that allows the participant’s back to gradually tilt back when the pelvis tilts back. To prevent effects on measurement results from a participant exerting force on the floor through the soles of the feet, feet were placed on a wheeled board (30 cm × 30 cm).
The participants, of course, have various body weights, so measurement values cannot be simply compared. Therefore, we normalized measurement values from the apparatus according to the participant’s weight and represented values as a percentage of the body weight.
Statistical analysis
We calculated the Pearson product–moment correlation coefficient to verify the relationship between the pelvic tilt and the vertical/horizontal force on the sacrococcygeal region. The statistical analysis software SPSS 15.0J (IBM Japan Ltd, Tokyo, Japan) was used to calculate the correlation coefficient.
Results
Vertical force
We first compared the results for the ischial and sacrococcygeal plates. Starting at 15° tilt, the ischial tuberosity area values declined and sacrococcygeal area values showed a sharp increase. The sacrococcygeal and ischial tuberosity area values were approximately the same at 25° tilt, and sacrococcygeal area values exceeded ischial tuberosity area values at 30°. The sacrococcygeal plate measurement values increased between pelvic tilt angles of 0° and 30° in all 30 participants. The coefficient of correlation between posterior pelvic tilt and vertical force on the sacrococcygeal plate was as high as 0.96 (1% significance) (Figure 4(a)).
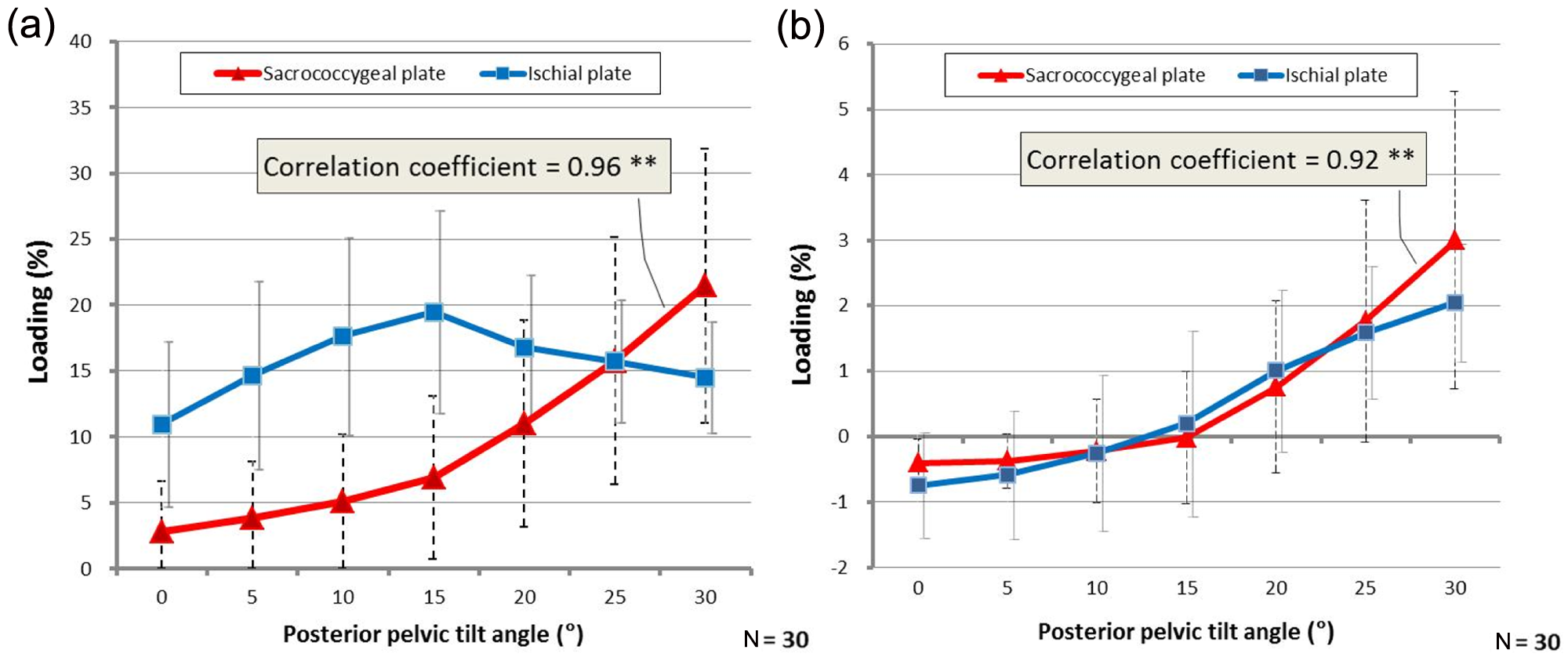
(a) Vertical force measurement results and (b) horizontal force measurement results. The vertical axis shows the measurement values for each plate, and the horizontal axis shows the pelvic tilt angle. Measurement values are normalized by body weight and displayed as a percentage. Ischial tuberosity plate measurement values are expressed as left and right values. In (b), positive values indicate forward-sliding force and negative values indicate rearward-sliding force. Dotted lines show the standard deviation of sacrococcygeal plate measurement values, and solid lines show the standard deviation of sacrococcygeal and ischial plate measurement values. “*” and “**” indicate 5% and 1% significance levels for Pearson product–moment correlation coefficients, respectively.
Horizontal force
Both ischial tuberosity and sacrococcygeal areas started with negative values at a posterior pelvic tilt of 0°. As posterior pelvic tilt angle was increased, the values for both areas became positive at a tilt angle of approximately 15°. At 25°, where vertical force was the same for the sacrococcygeal and ischial tuberosity areas, the horizontal force on the sacrococcygeal area became larger than that on the ischial tuberosity area. For the sacrococcygeal plate measurement results, 28 of the 30 participants showed increased values between pelvic tilt angles of 0° and 30°. The coefficient of correlation between posterior pelvic tilt and horizontal force on the sacrococcygeal plate was as high as 0.92 (1% significance) (Figure 4(b)).
Discussion
This study has shown for the first time that in older patients, pressure and the resulting shearing force on the ischial tuberosity and sacrococcygeal areas increase with increasing posterior pelvic tilt. We next compare these findings with previous research related to the balance of pressure between the ischial tuberosity and sacrococcygeal areas. A study of 15 participants without disabilities found that 18% of the average body weight acts on each ischial tuberosity, while 21% of the loading is on the right and left thighs, and 5% is on the sacral area. 21 That study does not give details related to posture at the time of measurement, whereas this study found that ischial tuberosity values are similar at a 10° posterior pelvic tilt. We observed 17.6% loading on ischial tuberosity areas and 5.1% on the sacrococcygeal area. This study involved an older and lighter population, but taking a 10° posterior pelvic tilt as a comfortable posture for an individual without disabilities, our measurement results seem to be in approximate agreement with the previous results.
Vertical force on the ischial and sacrococcygeal plates increased up to 15° tilt. This is likely because body weight supported by the thighs shifted rearward in the first half of the phase, increasing the force. Starting at 15° tilt, ischial plate values decreased and sacrococcygeal plate values rapidly increased. This might occur because the body weight load is shifted from the ischial tuberosity area to the sacrococcygeal area as pelvic tilt increases and the tip of the coccyx comes into contact with the seat surface. Given that Postacchini and Massobrio 22 have reported the four types of coccyx curvatures with individual differences, there is a possibility that the point of the body weight load shifting from the ischial tuberosity to the sacrococcygeal area is influenced by the coccyx shape and the relative position of the ischial tuberosity and the sacrococcygeum.
Given that there is a risk of ulceration when pressure on the sacrococcygeal area exceeds 11%, 4 the pressure resulting from 15° tilt (where loading is 6.89%) appears to present little risk of ulceration, whereas there is such risk starting at 20° tilt (where loading is 11%). If horizontal force on the ischial tuberosity and sacrococcygeal areas causes pressure ulcer development, then such risk will be minimized at a posterior pelvic tilt angle of 15°, where horizontal force on the ischial tuberosity and sacrococcygeal areas is near 0 (0.2% on the ischial tuberosity area and 0% on the sacrococcygeal area).
The ischial tuberosity and sacrococcygeal areas are connected by bone and ligaments, so we expected that during forward sliding, these areas would slide along the seat surface with the same force. However, approximately the same values for horizontal force were seen up to only 25°, beyond which pressure was greater on the sacrococcygeal area. This indicates a slightly greater shearing force on the sacral bone at such times.
The measurement results indicate that there are individual differences in both vertical and horizontal forces, as reflected by their standard deviations. With regard to those differences, Garber and Krouskop 23 has reported that a slim body build results in a tendency for concentrated loading on bone protrusions, and differences in contact area over the seat surface resulting from body build likely affect the force distribution in the ischial tuberosity and sacrococcygeal areas. Thus, it may be difficult to apply the measurement results presented in this study to the general population, but even if actual measurement values vary, average values can be used to find general trends related to the hypothesis presented.
Posterior pelvic tilt itself has long been vaguely indicated as a risk factor for pressure ulcer development, but more specific seated posture recommendations are needed. We look forward to improved recommendations, such as specific tilt angles that present large or small risks. There remains a need for research on pressure ulcer development for final verification of posterior pelvic tilt angle thresholds at which the pressure ulcer risk arises.
Study limitations
This study takes pelvic angle as its sole factor, but seated posture is composed of many aspects, from head to foot. A more comprehensive study that considers additional factors such as trunk and head alignment remains necessary. This study, furthermore, used values measured from plates to represent forces on the sacrococcygeal and ischial tuberosity areas, resulting in a single measurement of the balance and change between three separate areas. We note that this meaning of “pressure” differs from measurements that use area units, such as contact pressure. Future studies that include additional conditions such as the effects of coccyx shape and body shape should result in more accurate measurement values.
Conclusion
We used 30 male and female participants aged 60 years and older to verify the changes in vertical and horizontal forces on the ischial tuberosity and sacrococcygeal areas with varying posterior tilt. Increased vertical force on the sacrococcygeal area was seen in all 30 participants between posterior pelvic tilt angles of 0°–30°, and a high coefficient of correlation of 0.96 (1% significance) was found for posterior pelvic tilt and vertical force on the sacrococcygeal plate. Similarly, increased horizontal force on the sacrococcygeal area was seen in 28 of the 30 participants between posterior pelvic tilt angles of 0° and 30°, and a high coefficient of correlation of 0.92 (1% significance) was verified for posterior pelvic tilt and horizontal force on the sacrococcygeal plate. This indicates that posterior pelvic tilt induces increased pressure and shear on the sacrococcygeal area.
This article has, for the first time, shown the changes in pressure and shear on the sacrococcygeal and ischial tuberosity areas that accompany changes in seated posture (pelvic tilt) and has verified the following hypothesis: Changes in seated posture (posterior pelvic tilt) are accompanied by changes in the level of pressure and shearing force on the ischial tuberosity and sacrococcygeal areas.
Footnotes
Acknowledgements
The authors thank Takashi Handa and Koji Niisato of the Saitama Industrial Technology Center for engineering assistance in preparing the sensors and measurement devices used in this study. The authors also thank Kunizo Hiraga of Hiraga Orthopedic Co., Ltd, for technical assistance in creating the measurement chair used in this study. Yuki Trading Company is acknowledged for providing the HORIZON posture measurement instrument used in this study.
Conflict of interest
One of the article’s authors, Taro Kemmoku, is a patent holder for ‘HORIZON’, the digital posture measurement instrument used in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-profit sectors.