
Abstract
Background:
This study aimed to evaluate the effect of total hip arthroplasty (THA) on sagittal pelvic parameters and to evaluate the effect of sagittal pelvic parameters on acetabular cup orientation.
Methods:
The study included 86 patients who underwent THA for a diagnosis of unilateral coxarthrosis between 2011 and 2015. Measurements were taken of the preoperative and postoperative acetabular cup inclination (ACI), anteversion, and sagittal pelvic parameters. The effect of THA on sagittal pelvic parameters and the effects of the sagittal pelvic parameters on acetabular cup orientation were investigated.
Results:
The sagittal pelvic tilt values calculated were mean 9.7° ± 6.3° (2°; 23°) preoperatively and 11.0° ± 6.1° (2°; 25°) postoperatively. The increase in postoperative pelvic incidence (PI) values was determined to be statistically significant (p < 0.05). The preoperative PI values had no significant effect on ACI, but in cases with high preoperative PI values, a tendency to high anteversion values was determined. The mean inclination values were found to be 40.2° ± 11.0° in the low PI group, 41.7° ± 7.4° in the normal PI group, and 44.1° ± 8.3° in the high PI group. As no increase in inclination values was observed with an increase in PI values, no statistical correlation was determined (p = 0.343). Average of anteversion values in the low PI group was 9.2° ± 13.7°, in the normal PI group 19.3° ± 10.5°, and in the high PI group 21.1° ± 12.5°. The difference between the groups was statistically significant (p = 0.001).
Conclusion:
Evaluating the results of this study, it can be concluded that varying PI values do affect the acetabular cup anterversion in THA. So, preoperative assessment of PI values is important in preventing postoperative acetabular cup malposition.
Introduction
Total hip arthroplasty (THA) is a surgical method with successful results which is being increasingly used in throughout the world in the elimination of hip problems which cannot be resolved with medical treatment. However, it must not be forgotten that the success of THA depends on appropriate patient selection, proper preoperative planning, the selection of an implant appropriate to the indications, and effective rehabilitation applied postoperatively.
Inclination and anteversion of the acetabular cup in THA are associated with the postoperative range of movement, postoperative dislocation risk, increased risk of polyethylene wear, and thereby increased risk of osteolysis and implant loosening. 1 –3 With the appropriate orientation of the acetabular cup, dislocation rates are low, and it is essential in respect of reducing the risk of insert wear. 4 –8 Dislocation rates after THA are estimated to be 1–5%. 9 –11 A lower incidence of all types of dislocations has been shown in cases where the acetabular cup inclination and acetabular cup anteversion (ACA) are within acceptable limits, 1,6 while there is an increased risk of anterior dislocation in cups with excessive anteversion and cups with over-retroversion increase the risk of posterior dislocation. 1,5,11
Pelvic incidence (PI) is an anatomic parameter first described by Duval-Beaupere et al. 12 Sagittal pelvic tilt (SPT) is a positional parameter related to the sacral slope (SS) of an individual and the position of the vertebrae and it has been shown to have an effect on acetabular cup orientation. 1,13 PI is a nonpositional morphological parameter and is independent of the individual and vertebrae positions. PI can be easily measured in daily practice using direct radiographs. 12 –16 The SPT and SS angles are directly related to the PI angle. The PI angle is the arithmetic total of the SPT and SS angles. 13,15,17 Sagittal postural balance varies from patient to patient. Variations in the PI are consistent with the sacral tilt and the arch of the sacrum between the iliac wings. There may be a significant relationship between PI and three-dimensional orientation of the acetabular cavity during THA.
This study aimed to evaluate the effect of THA on sagittal pelvic parameters and to evaluate the effect of sagittal pelvic parameters on acetabular cup orientation.
Materials and method
One hundred twenty-three underwent THA as surgical treatment for a diagnosis of unilateral coxarthrosis between March 2011 and March 2015 in our department. The Local Clinical Research Ethics Committee approved the study. Prospective collective data were evaluated retrospectively. To obtain homogenization in the groups, patients were excluded if there was a diagnosis of bilateral coxarthrosis (16 patients), if arthroplasty or other surgical procedure had been applied to the contralateral hip (8 patients), if there was a history of any vertebral surgery (5 patients), if the patient had fixed flexion contractures of the hip (1 patient), or if coxarthrosis had developed on the basis of acetabular dysplasia or acetabular fracture (7 patients). Eighty-six patients who met the inclusion criteria were included in the study. All patients were operated on by the same surgical team using a posterolateral incision with the patient in a lateral decubitus position. The Harris Hip Scoring (HHS) system was used for the clinical evaluation of the patients.
Radiographic measurements
At the final follow-up examination of the patients applied with THA in this study, standard pelvis anterior–posterior radiographs were taken with the patient supine and both lower extremities in 15° internal rotation and the cassette below the hip and the light focusing on the symphysis pubis from a height of 115 cm. Standing pelvis lateral radiographs were also taken including the lumbar vertebrae, pelvis, both femoral heads, and proximal femur. 18 –21
Computed tomography (CT) images were taken at 0.6-mm slice thickness with metal artifact eliminating software (256 slices multidetector scanner; Siemens®, Erlangen, Germany). Each CT image of the patients was examined by radiologists experienced in musculoskeletal system radiology with Leonardo Dr/Dsa Va30a software (Siemens). To reduce interobserver and intraobserver errors, the images of the patients were evaluated double-blind by three different orthopedic surgeons. Measurements were made to a sensitivity of 1/10 mm. The highest tolerance between all the measurements was determined as 0.7°.
Definitions
Acetabular cup inclination
As described by Woo and Morrey, 22 this is defined as the measurement taken on the standard pelvis anterior–posterior radiograph of the angle between the line passing over both edges of the acetabular cup and the line joining the lowest points of both ischial tuberosities (the transischial line; Figure 1).

Measurement of ACI angle. ACI: acetabular cup inclination.
Acetabular cup anteversion
The measurements of the acetabular cup version were taken on the postoperative CT images. On the pelvis CT axial slices, the most anterior and posterior points of the acetabular cup were marked, and a straight line was drawn between these two points. The angle between this line and the sagittal plane of the body was measured as the acetabular version. If this angle was angulated toward the anterior side of the pelvis, the acetabular cup was defined as in anteversion, and if angulated toward the posterior of the pelvis, it was defined as in retroversion. When the acetabular cup was in anteversion, the measurements were stated as positive numbers, and when in retroversion, the measurements were stated as negative numbers 23,24 (Figure 2).
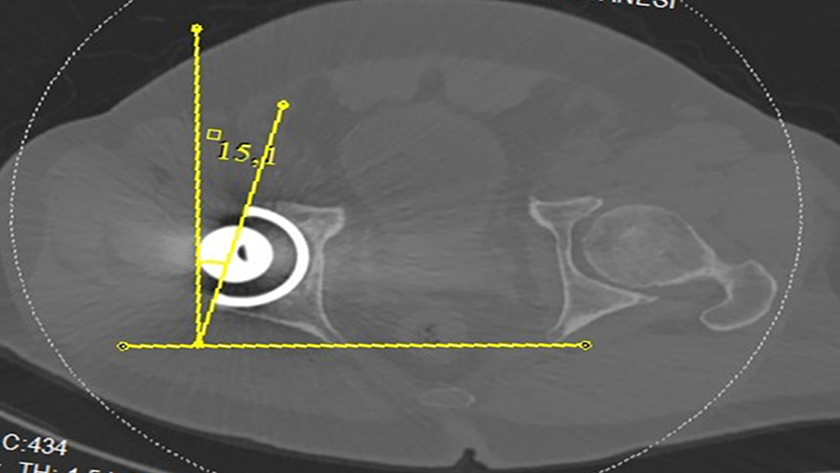
Measurement of ACA angle. ACI: acetabular cup inclination.
Sacral slope
This is defined as the angle between the sacral plateau and the horizontal plane and is a positional parameter (Figure 3).

Preoperative and postoperative measurements of sagittal pelvic parameters.
The angle changes in different positions of the individual. If there is a low SS angle, it indicates a vertical sacrum, and if there is a high SS angle, it indicates a horizontal sacrum.
Sagittal pelvic tilt
This is the angle between the line drawn from the midpoint of the line joining both femoral head centers to the midpoint of the sacral plateau and the vertical plane 25 (Figure 3).
If the line joining the sacral plateau and both femoral head centers are toward the posterior, the pelvic tilt is expressed in positive values, and if toward the anterior, the pelvic tilt is expressed in negative values.
Pelvic incidence
This is defined as the angle between the vertical line drawn to the midpoint of the sacral plateau and the line drawn from the midpoint of both femoral head centers to the midpoint of the sacral plateau 14 (Figure 3).
PI is a morphological parameter which is not positional and is independent of the position of the individual and the vertebrae. PI can be easily measured in daily practice using direct radiographs. 12 –16

Safe limits of acetabular cup orientation were defined by Lewinnek et al. 1 The inclination and anteversion values of the acetabular cup separated into three categories of low, normal, and high. For the inclination angle, the normal range was defined as 30–50, <30° as low, and >50° as high. For the anteversion angle, the normal range was defined as 5°–25°, <5° as low, and>25° as high.
Statistical analysis
Conformity to a normal distribution of the variables obtained in the study was evaluated visually and with the Shapiro–Wilk test. Variables showing normal distribution were stated as mean ± standard deviation and those not showing normal distribution as median (minimum–maximum) values. For the comparison of preoperative and postoperative HHS, SS, SPT, and PI variable values, the Wilcoxon signed-rank test was used. In the examination of whether or not any difference was seen in the distribution between the groups of categorical variables, the Pearson’s χ 2 test and Yates’ corrected χ 2 tests were used as appropriate. Kruskal–Wallis nonparametric variance analysis was applied to evaluate differences in the preoperative PI groups. Relationships between the preoperative PI groups and anteversion groups were examined with the Gamma statistic. The statistical analyses and calculations were applied using International Business Machines (IBM) SPSS Statistics 21.0 (IBM SPSS Statistics for Windows, released 2012, version 21.0; IBM Corporation, Armonk, New York, USA) and MS Excel 2007 software. A value of p < 0.05 was accepted as statistically significant.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Results
The study included a total of 86 patients, comprising 37 (43%) males and 48 (57%) females with a mean age of 56.2 ± 12.2 years (range, 31–75 years). Mean body mass index was 28.0 ± 3.7 and the median follow-up period was 32.0 months (range, 12–60 months). The diagnosis was left-side coxarthrosis in 44 (51.2%) cases and right-side coxarthrosis in 42 (48.8%) cases. The mean HHS was determined as 45.3 ± 6.4 (range, 32–59) preoperatively and 92.2 ± 5.4 (range, 73–99) postoperatively. The postoperative increase in HHS was found to be statistically significant (p < 0.001). In the preoperative evaluation, none of the patients had hip deformity, spinal deformity, and flexion contracture in the hip. We did not have any dislocated hips.
According to categories defined by Lewinnek et al., 1 there were no cases in the low category of inclination value, 70.9% of cases were in the normal group, and 29.1% in the high group. Thirty-eight (44.2%) cases were evaluated as having normal anteversion values, 22 (25.6%) cases had low anteversion values, and 26 (30.2%) had high values (Table 1).
Distribution of categorical variables of the patients.

Through evaluation of the inclination and anteversion values together, the patients were then separated into three different groups as those who were within the safe limits defined for both values (inclination: 40° ± 10° and anteversion: 15° ± 10°), those who were outside the limits, and those who were within at least one. In 28 (32.6%) cases, both the inclination and anteversion values were within the defined safe limits, in 15 (17.4%) cases, neither the inclination nor anteversion values were within the defined safe limits, and in 43 cases, only one of the inclination or anteversion value was within the defined safe limits (Figure 4).

Graph showing the distribution of ACI and ACA angle values. ACI: acetabular cup inclination.
The results of the comparison of the sagittal pelvic parameter values (SS, SPT, and PI) measured on the preoperative and postoperative lateral pelvis radiographs are shown (Table 2).
Comparison of the preoperative and postoperative sagittal pelvic parameters.
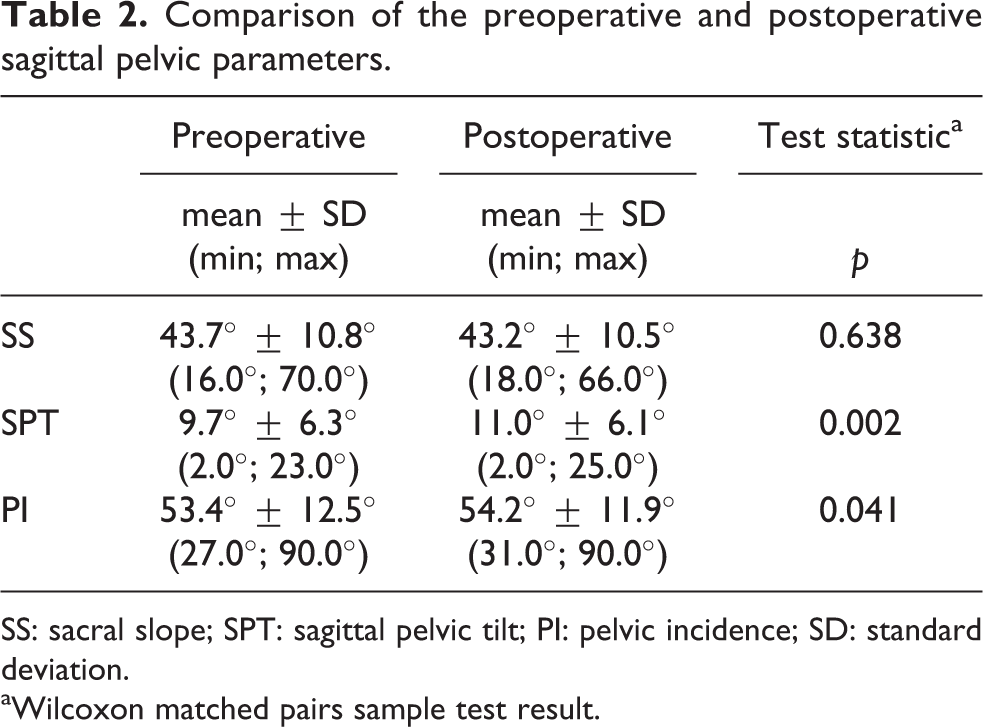
SS: sacral slope; SPT: sagittal pelvic tilt; PI: pelvic incidence; SD: standard deviation.
aWilcoxon matched pairs sample test result.
The SS values calculated in the study were mean 43.7° ± 10.8° (16°; 70°) preoperatively and 43.2° ± 10.5° (18°; 66°) postoperatively. These values were very close, and no statistically significant difference was determined (p = 0.638).
The SPT values calculated were mean 9.7° ± 6.3° (2°; 23°) preoperatively and 11.0° ± 6.1° (2°; 25°) postoperatively. Although there was a slight increase in the postoperative SPT values, this was found to be statistically significant (p = 0.002).
The PI values were calculated as median 52° (min, 27.0°; max, 90.0°) and mean 43.7° ± 10.8° preoperatively and median 55.0° (min, 31.0°; max, 90.0°) and mean 54.2° ± 11.9° postoperatively. The increase in postoperative PI values was determined to be statistically significant (p < 0.05).
To evaluate whether or not the preoperative sagittal pelvic parameter values affect the position of the acetabular cup, comparisons were made of the PI values as PI is a morphological parameter not affected by position. Groups were defined from the values measured on the preoperative radiographs as 50°–60° normal PI, <50° low PI, and >60° high PI. 26 According to these values, 30 (34.9%) patients were evaluated as having PI values in the normal range, 32 (37.2%) in the low PI group, and 24 (27.9%) in the high PI group (Table 3).
Comparison of the inclination and anteversion values of the PI groups.

PI: pelvic incidence; SD: standard deviation.
aKruskal–Wallis test results.
The mean inclination values were found to be 40.2° ± 11.0° in the low PI group, 41.7° ± 7.4° in the normal PI group, and 44.1° ± 8.3° in the high PI group. As no increase in inclination values was observed with an increase in PI values, no statistical correlation was determined (p = 0.343).
The mean anteversion values were found to be 9.2° ± 13.7° in the low PI group, 19.3° ± 10.5° in the normal PI group, and 21.1° ± 12.5° in the high PI group. The increase of the preoperative PI values increased anteversion values. The difference between the groups was statistically significant (p = 0.001) (Figure 5, Table 3).
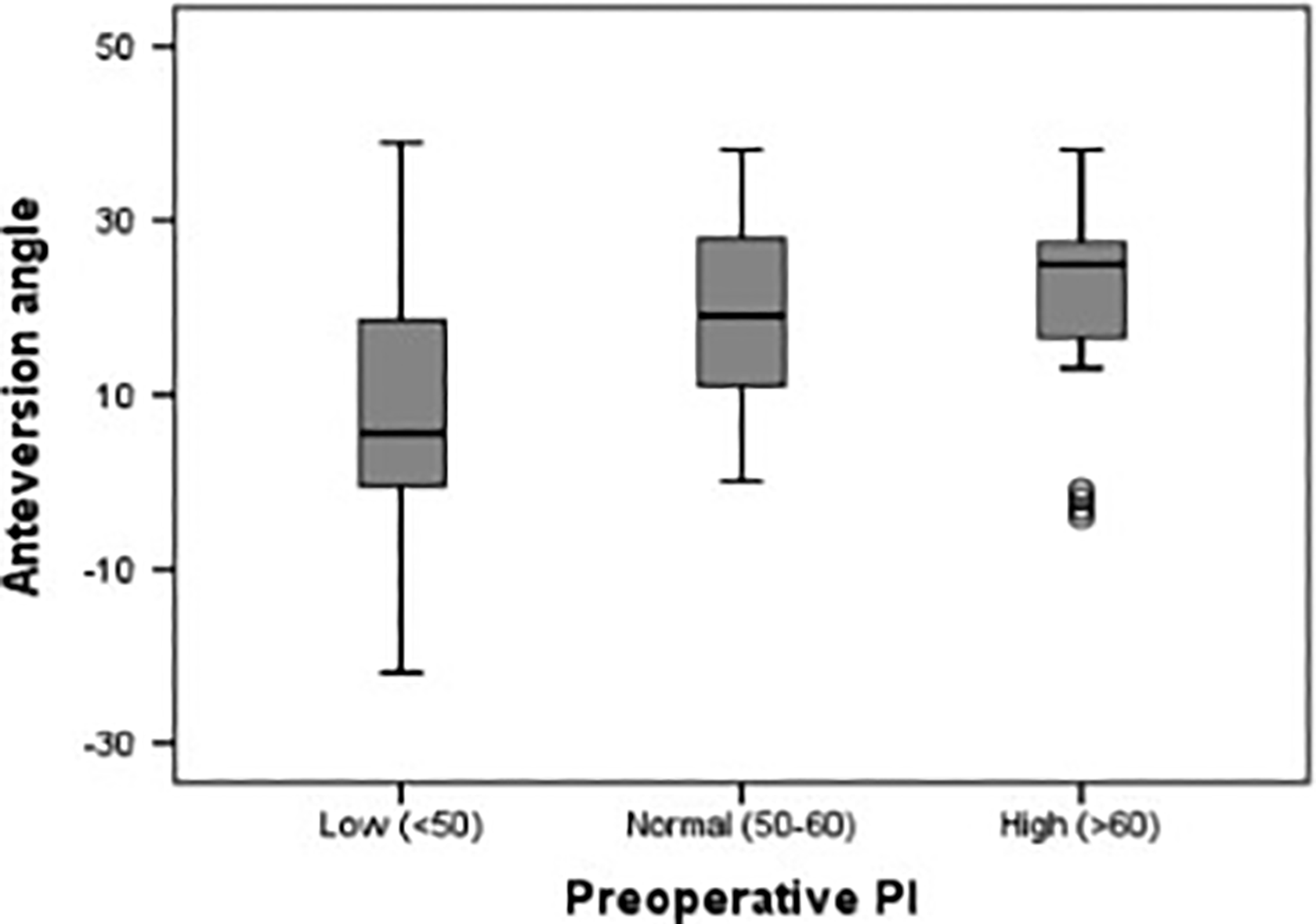
Graph of the distribution of the anteversion mean values in the PI groups. PI: pelvic incidence.
A significant difference was found in the distribution of the individuals in the PI groups and anteversion groups (p < 0.001). Of those with preoperative low PI values, 50% were in the low anteversion group, 6.7% of those with normal PI, and 16.7% of those with high PI (Figure 6, Table 4).

Graph of the percentage distribution of the preoperative PI groups in the anteversion groups. PI: pelvic incidence.
Distribution of the PI groups in the inclination, anteversion, and Inclination × Anteversion Groups.a

PI: pelvic incidence.
aKruskal–Wallis test results.
Discussion
The orientation of the acetabular component is one of the most important factors in the determination of long-term results of THA. 27 –30 That the acetabular cup is in the correct position in a permanent form is very important for the success of THA. 31–32 Malpositioning of the acetabular cup is accepted as a significant cause of dislocation, impingement, loss of range of movement in the joint, and increased and early wear. 33 , 34
The inclination angle of the acetabular cup of the 86 patients in the study was found to be mean 41.8° ± 9.1° (24°; 60°), and the anteversion angle was found to be mean 16.0° ± 13.3° (−22°; 39°). In a study with a large number of patients by Callanan et al., 35 the inclination angle was reported to be mean 42.2° ± 6.8° (21°; 73°), and the anteversion angle was reported to be mean 12.7° ± 7.4° (−17°; 43°). In another study of 1021 patients, the values were reported as mean inclination 45.7° and anteversion mean 10.3°. 36 Similar results can be seen in several studies in the literature with inclination angle as mean 37.5°–49.7° and anteversion angle as mean 10.7°–27.3°. 37 –43
The safe limits defined in the current study were in the range defined by Lewinnek et al., 1 as acceptable limits for acetabular cup rotation (anteversion 5°–25° and inclination 30°–50°). While 70.9% of the current study cases were within the defined safe range for inclination, 44.2% were within the defined safe range for anteversion. This low rate could be related to the posterior approach. It is not surprising to see greater anteversion in the posterior approach, because it is recommended to give greater anteversion as there is an increased risk of dislocation in this approach. 44 THA was applied with a posterior approach to all the patients in the current study. To reduce the risk of posterior dislocation, there was a tendency to apply more anteversion in the posterior approach, and this could have resulted in the low rate of anteversion values within the safe range. This view is supported by the total rate of 74.4% of cases with anteversion within the defined safe range and those with higher than the safe range. When anteversion and inclination were evaluated together, 32.6% of the cases were seen to be within the defined safe range. Literature is unclear about the percentage of cases with both inclination and version at a level which could be acceptable. This rate has been reported as 70.5% by Bosker et al, 37 47% by Callanan et al, 35 41% by Reize et al, 41 and 25.7% by Saxler et al. 42 In the current study, the low percentage of cup anteversion values within the safe range (44.2%) was seen to have reduced the percentage of the group where defined optimal cup position achieved when the inclination and anteversion values were combined.
PI is a morphological parameter which is not positional and is independent of the individual and vertebrae position. In daily practice, PI can be easily measured on direct radiographs. 12 –16 There is a direct relationship between the PI angle and SPT and SS angles. The PI angle value is the arithmetic total of the pelvic tilt and SS values. 17 The mean value of the PI angle is 55° ± 5°, but this mean value does not state anything but defines the pelvis characteristic as this is an anatomic property not affected by the individual and vertebrae position, which is defined at the end of growth and differs from person to person. The PI of an individual cannot be classified as excellent or poor. This angle only defines the anatomic characteristic of the pelvis specific to that person. The smallest value of the SS is 0 as it cannot be a negative value. Thus, it is possible for the maximum retroversion of the pelvis to be parallel with the horizontal plane of the sacral plateau. 26
In the current study, the preoperative SS value was calculated as mean 43.7°, the SPT as mean 9.7°, and PI as mean 53.4°. In a study by Vialle et al. 26 of 300 symptomatic patients, the SS value was reported as mean 13° and the PI value as mean 55°. Raphael et al. 45 compared hips with and without osteoarthritis and reported the mean PI value as 56.5° in those with coxarthrosis and as 57.2° in cases without coxarthrosis and determined no difference between the mean PI values of the two groups. If it is considered that radiographs could have been taken in different positions, that the mean PI values of the current study show a close similarity to findings in the literature is important as this is a parameter not affected by position.
Several studies have reported a minimal change in SPT postoperatively compared to preoperative values. 46 –49 Murphy et al. 49 demonstrated that there could be a minimal change in pelvic tilt after surgery. The preoperative pelvic tilt in supine and standing positions is an indicator for postoperative pelvic tilt. Blondel et al. 46 examined the lateral radiographs of 50 patients and reported a tilt change of <5° in 95% of patients in the third year after THA. In a CT-based study by Nishihara et al., 18 there was seen to be tilt change of <10° in the majority of a series of 74 patients after THA. In the current study, as a result of the comparison of preoperative and postoperative sagittal pelvic parameters, a minimal increase was determined in SPT, which was consistent with the literature.
No significant change was determined in the SS values. As the PI value is the arithmetic total of SS and SPT, there should have been an increase, and in the current study, a significant increase was observed in the postoperative PI compared to the preoperative value. Postoperatively, no change was seen in the SS, there was an increase in the SPT, and the center of the femoral head was seen to have moved more anteriorly. During the placement of the acetabular component, attempting to protect the posterior wall in particular, because of the critical contribution to stabilization could have caused this anterior movement of the center of the femoral head postoperatively. In a study by Blondel et al., 46 which included patients operated on with an anterolateral approach, no significant difference was determined between preoperative and postoperative PI values. In the current study, all the patients were operated on with a posterolateral approach, and the difference may, therefore, have arisen from the different surgical approaches.
In the current study, it was also investigated whether or not the preoperative sagittal pelvic parameters affected the placement of the acetabular cup. The comparison was made from the preoperative PI values, as PI is a morphological parameter not affected by position. 26 It has been shown that PI does not change after the age of 10 years and there is no difference between the genders. 16,50 As a result of the analysis that investigated the effect on the position of the acetabular cup of the PI groups defined as low, high, and normal, no difference was determined in respect of the acetabular inclination values of the PI groups. However, a statistically significant difference was determined in the anteversion values of the PI groups. The lowest anteversion angle mean values were seen in the low PI group and the highest mean anteversion values in the high PI group. It was determined that an increase in preoperative PI value led to an increase in postoperative ACA value and the relationship between these was statistically significant.
In the current study group defined as normal PI (50°–60°), the number of those within the safe limits in respect of anteversion angles was found as significantly higher. The number of those within the defined safe limits for ACA values was determined to be greater in the normal PI group. The risk of placement of the acetabular cup with an inappropriate anteversion angle was determined to be greatest in the low PI group.
When the PI is low, lumbar lordosis decreases and the adaptation gap of the SS is more reduced. Theoretically, in cases of high PI, lumbar lordosis increases and the femoral heads are pushed forward compared to the sacrum 51,52 (Figure 7). The amount of adaptation of the sacrum is more significant. At the stage of providing sagittal balance to protect the lumbar vertebrae from the mechanical stresses which occur associated with the increase in lumbar lordosis, there may be a relationship between the greater adaptation gap and high PI. 53 This posterior tilt of the pelvis reduces coverage of the femoral head by making the articular surface more vertical. 54 –56 In the current study, patients determined with high PI, the tendency for anteversion to be high or in complete contrast and the tendency for low anteversion values in patients with low PI values may have been the reason for the differences in the pelvic slope. In the intraoperative determination of ACA, markers, which are used such as the transverse acetabular ligament, are affected by the pelvic slope.

Schematic view of the lumbosacral region with low and high PI values. PI: pelvic incidence.
We think that preoperative PI values alter the surgeon’s judgment in determining the acetabular anteversions. That is why, in order to eliminate the acetabular anteversion problems, preoperative sagittal pelvic parameters must be carefully evaluated before the surgery.
There are some limitations to this study. The first is that it included 86 patients with a mean follow-up period of 32 months. There is a need for further studies with higher numbers of patients and with a longer follow-up period. The second limitation is that the femoral component rotation was not evaluated. This is important because acetabular cups placed with a version angle outside the acceptable limits may have been placed deliberately compatible with femur rotation. Finally, although there is known to be a close relationship between the sagittal pelvic parameters and vertebrae, no evaluation was made in respect of vertebral morphology or pathology. If future similar studies are combined with vertebral evaluation, a wider area of discussion could be opened.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.