
Abstract
Background and aim:
Sport is associated with risk of injury and re-injury. A rehabilitative sport-related orthosis could protect the injured site and help in the earlier return of athlete to the match. This technical note aims to describe a potential high-prescribed face orthosis to protect/prevent a sport-related injury.
Technique:
Face-protective orthosis should be custom molded from negative impression of the injured athlete’s face. It is lightweight and structured as a one-piece rigid plastic shell that is secured in place with three elastic straps. Due to the diverse patterns of craniomaxillofacial injuries, the shape, length, trimline, and characteristics of face-protective orthoses could be different.
Discussion:
Face-protective orthoses could have prophylactic or rehabilitative roles according to task and prescription reason. Although the main action of the facial orthoses should be protection, the design of the face-protective orthosis should be improved both functionality and aesthetically to promote its use by athletes.
Clinical relevance
The craniomaxillofacial injuries have potential to be treated by custom-molded face-protective orthoses. These orthoses could have prophylactic or rehabilitative roles based on their prescription purpose. These orthoses could cause earlier return of athletes to sports matches.
Background and Aim
Sport is associated with risk of injury and re-injury. 1 Sport-related injuries vary greatly in pattern and location. Although craniomaxillofacial traumas are of the most common sport-related injuries, 2 11% to 40% of all cases, 3 limited attention is paid to their orthotic treatment, probably due to few athletic activities that are limited by these injuries.
The most common sport-related facial traumas are soft tissue injuries and bone fractures. Facial soft tissue injuries account for 8% of all soft tissue injuries. 3 The most common facial bone fractures are related to nasal, zygomatic, and mandibular bones primarily due to impact of other players especially in team games.2,3,4 Elbow or head strikes, falls, and collision to the game accessories and equipment are other causes of maxillofacial fractures. 5
Nowadays, sport is a profession, and often athletes are paid based on their participation and performance. Missing a training or playing session may encounter the athlete with loss of his or her place in the team in the next game or his or her wage. 5 Early return of an injured athlete to the match is associated with high risk of another impact to the injured site that may convert a simple situation to a sophisticated complex surgery. 6 A rehabilitative sport-related orthosis could protect the injured site and help earlier return of the athlete to the match. The main responsibility of a protective sport-related face orthosis is providing the highest possible protection for the face. It should closely fit the face, be smooth, and have little risk for opponent players during the match. This technical note aims to describe a potential high-prescribed face orthosis to protect or prevent a sport-related injury.
Technique
Although a great variety of materials exist for fabrication of protective sport orthoses, the proper selection of type, thickness, and density of material is defined by sports organizations that are responsible of care for the health and safety of the athletes at all levels of play. 7 These organizations range from international governing bodies to local clubs and should regularly determine regulations based on sport, age of participants, and the level of competition to manage risk of athletes during their sport.7,8 Although for protection of the most body parts, thermomoldable plastics with soft resilient padding are appropriate, due to high load and repetitive nature of most contact sports, they are inappropriate for sport gloves, for example, in lacrosse, hockey, and boxing. 8 Both high-temperature (325–350°F) and low-temperature (150–180°F) thermoplastics could be malleable to use for fabrication of protective sport orthoses. Low-temperature thermoplastics could be formed over body parts that provide faster fabrication and lighter orthoses. These materials have disadvantages of minor stiffness for protection and insufficient fit. 8
To fabricate a custom-molded FPO, the athlete should lie supine with face upward to prevent any distortion of the impression form. The orthotist should first isolate the athlete’s facial skin by a thin Nylon sheet prior to casting. The sheet is necessary for protection of eyes and should have nasal holes for passing tubes to allow breathing during casting. Negative impression should be taken by 4–6 plies of gypsum plasters that were pre-cut according to the shape (round, oval, square, asymmetric, or heart-shaped) and size of athlete’s face. After setting the plaster, negative impression would be removed from the face to be converted to a positive mold. Following some rectifications, for example, by addition of gypsum to the injured site to make it more prominent, the mold would be ready for thermo-molding the structure of the orthosis. Color transfer papers could be used for aesthetic improvement. The plastic shell of the orthosis should be custom-trimmed both to the athlete and the injury site; for example, in athletes with eyebrow soft tissue injury, probably less superior–inferior dimension of ocular hole is more beneficial. In addition, in athletes with nose fracture, the nasal section should preferably be greater than nose length for better coverage and protection. To design these orthoses, it is critical to consider open structure to reduce perspiration and improve ventilation.
Face-protective orthosis (FPO) should be lightweight, should preferably have a one-piece structure, and be secured in place snugly. The cranium surrounding straps in sagittal and frontal planes reduce risk of orthosis migration during activity. To further decrease motion, reduce friction of interfaces, absorb energy of contacts, and finally, to disperse the loads over a larger area, the plastic shell of the orthosis should be fully padded by soft resilient materials. 8 A 0.5 cm-thick layer of Neoprene glued to a layer of 0.5 cm-thick polyethylene foam is appropriate for padding the orthosis.
In most cases with facial traumas, the shell of the orthosis should consist of three sections: forehead, nasal, and zygomatic sections. The ocular hole of the orthosis should be properly trimmed to permit unobstructed sight. Holes were placed peripherally on the forehead and zygomatic sections for passing straps (Figure 1).
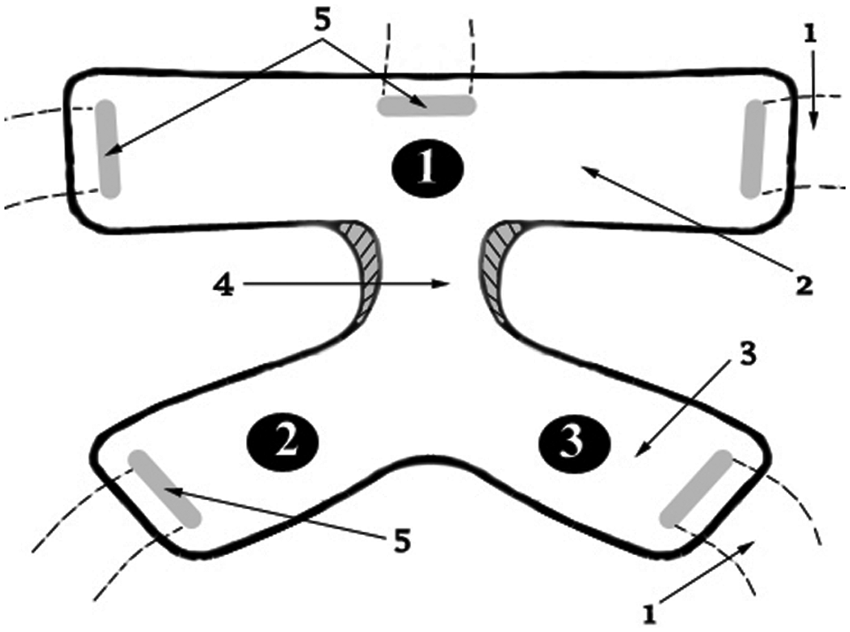
Schematic view of face-protective orthosis: (1) elastic strap, (2) forehead section, (3) zygomatic section, (4) nasal section, and (5) hole for strap.
The FPO is a static orthosis that has three posteriorly directed forces, one by forehead and two by zygomatic sections. This orthosis has a fully contoured gap in its nasal section for protection of the injured nose.
Due to diverse patterns of craniomaxillofacial injuries, the shape, length, trimline and characteristics of FPOs are different. Figure 2 shows a professional soccer player with eyebrow soft tissue injury that used FPO with gaps in soft padding on the sutures. The FPO could be applied by some modifications and attachment of intranasal clip wires in comminuted nasal bone fractures for fixation and reduction. 9

A professional soccer player used face-protective orthosis for protection of his prior injury.
Discussion
FPOs could have prophylactic or rehabilitative roles according to task and prescription reason. The popularity and acceptance of FPO in some sports, such as football and ice-hockey, as a prophylactic orthosis 5 is mainly due to sports regulations. In 1959, a high rate of fatalities during sports, especially in football, made governing bodies regulate mandatory use of facemasks for football players.6,10 Following this success, the national operating committee on standards in athletic equipment was formed in 1969 to evaluate the quality of the protective helmets and further decrease the rate of football-related injuries. 10 The use of FPOs in other sports such as soccer and basketball is not accepted as a prophylactic device mainly due to aesthetic issues and limited awareness.4,6 In soccer, use of FPOs is accepted as a rehabilitative device. 11 The fourth law of the international governing body for soccer regarding the player’s equipment has clearly determined that at the start of a match the referee should inspect the player’s equipment to ensure that they are not dangerous. This resource also determined that facemasks are permitted based on referee’s approval, if they are made of soft, lightweight, padded materials. 11
Although the main action of the FPOs should be protection, the design of FPO should be improved both functionally and aesthetically to promote its use by athletes. Due to these limitations, the most prescribed postoperative or postinjury FPO is the prefabricated nose guard. These prefabricated orthoses are not as efficient as custom-molded ones due to diverse patterns of facial injuries and lack of a proper fit. 12 It is worth noting that there are many variables when designing FPOs, but their descriptions are beyond the scope of this technical note.
Key Points
Diverse patterns of facial injuries and importance of proper fit urge orthotists to design custom-molded FPOs.
Governing bodies are responsible of care for safety of athletes and should regulate the use of FPOs in contact sports.
Functional and aesthetical improvements of FPOs may increase their popularity in future.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.