
Abstract
Background:
Static wrist splinting after stroke was not effective in facilitating distal movement. However, the purpose of this study is to evaluate the efficacy of training using kinematic parameters after a SaeboFlex orthosis training on chronic stroke patients.
Case Description and Methods:
Five stroke patients participated in 4 weeks of training using a SaeboFlex orthosis for 1 hour per day, five times per week. Fugl-Meyer Assessment, Box and Block Test, Action Research Arm Test, and Kinematics using a three-dimensional motion analysis system were used for evaluating of training effects.
Findings and Outcomes:
The upper extremity score of the Fugl-Meyer Assessment and the Box and Block Test score were increased significantly after the intervention. The jerkiness score of the shoulder and elbow joints at the sagittal plane decreased significantly during the reach-to-grasp task at acromion height, and the jerkiness scores of the wrist joint during the reach-to-grasp task decreased significantly at both elbow and acromion heights.
Conclusion:
The results of this study indicate that a SaeboFlex training is effective in recovering the movement of the hemiparetic upper extremity of patients after stroke.
Clinical relevance
Using a spring-assisted dynamic hand orthosis is considered to be an effective treatment option for providing repetition, task-oriented training, and real-world activities for the hemiparetic upper extremity, which was impaired hand to perform functional training.
Background
Stroke causes a variety of damage to body structures and functions, including changes in the level of consciousness, and impaired sensory, motor, cognitive, perceptual, and language functions. 1 Clinically, complications in the shoulder, such as pain and subluxation, can also hinder the patient’s ability to move. It has been proposed that stroke survivors experience a conditioned suppression of movement in the affected upper extremity. 2 In fact, several previous studies reported that some physical interventions were effective in improving upper extremity functions even in chronic stroke patients.3–6 However, the effectiveness of intervention has generally been less pronounced for the upper extremity than for the lower extremity.7,8
Practicing real-world tasks is one of the most commonly accepted training strategies for overcoming the residual functions of proximal and/or distal segments of the affected limb. 9 Constraint-induced movement therapy (CIMT) is one of the relatively new treatment options for maximizing the motor recovery of upper extremity in functional rehabilitation for stroke victims. CIMT has been influenced by the task-oriented approach and it consists of unaffected limb constraint, massed training of the affected limb, and shaping of behavior to improve the amount of use in the affected limb. 10 Dursun et al. 11 suggested that CIMT is an encouraging treatment approach for improving upper extremity motor function in chronic stroke patients. Moreover, static splinting is accomplished by positioning the wrist at a static extension angle, and maintaining the digits in desirable positions. The expected benefits of the splint are the prevention or reduction of contracture, with its resultant shortening of the wrist and finger muscles, and the functional improvement of affected hand. 12 However, the effectiveness of a static hand splint on motor recovery in hemiplegic hand function is controversial. 13 In addition, problems related to task-specific practice do not increase movement in the case of minimal distal movement in the hemiparetic upper extremity, and therefore, it is difficult to apply intensive training. 14
A commercial splinting system called SaeboFlex orthosis (Saebo, Inc., Charlotte, NC) was developed in order to overcome the disadvantages of previous approaches as described above. It is designed to permit quick training in opening and closing the affected hand. It is attached to a dorsal hand covering that anchors the pulley and spring attachments. It is a new treatment approach applied recently in patients suffering the effects of a stroke.12,15 The purpose of this study was to evaluate kinematic parameters for the effectiveness of training using a SaeboFlex orthosis on jerkiness score, and the Box and Block Test (BBT), Action Research Arm Test (ARAT), and Fugl-Meyer Assessment (FMA) of clinical assessment scores for upper extremity function of the affected limb in chronic hemiparetic patients.
Case Description and Methods
Participants
For this study, five stroke patients for the training group were recruited from a local rehabilitation hospital in Republic of Korea. This project was approved by the Yonsei University Wonju College of Medicine institutional review board; all patients agreed to participate in this study and signed an informed consent form. Inclusion criteria were the following: (1) unilateral hemiparesis more than 6 months post-stroke duration; (2) no current or previous orthopedic or surgical histories affecting the hemiparetic upper extremity; (3) Mini-Mental State Examination (MMSE)—score ≥ 23; (4) patients should have at least some active voluntary movement of the upper extremity (i.e. 10° of shoulder flexion/abduction, 10° of elbow flexion/extension, and 30° of interphalangeal proximal joints/20° of interphalangeal distal joints of volitional finger flexion when the hand is positioned in wrist and finger extension) (Table 1).
General characteristics of participants (n = 5).
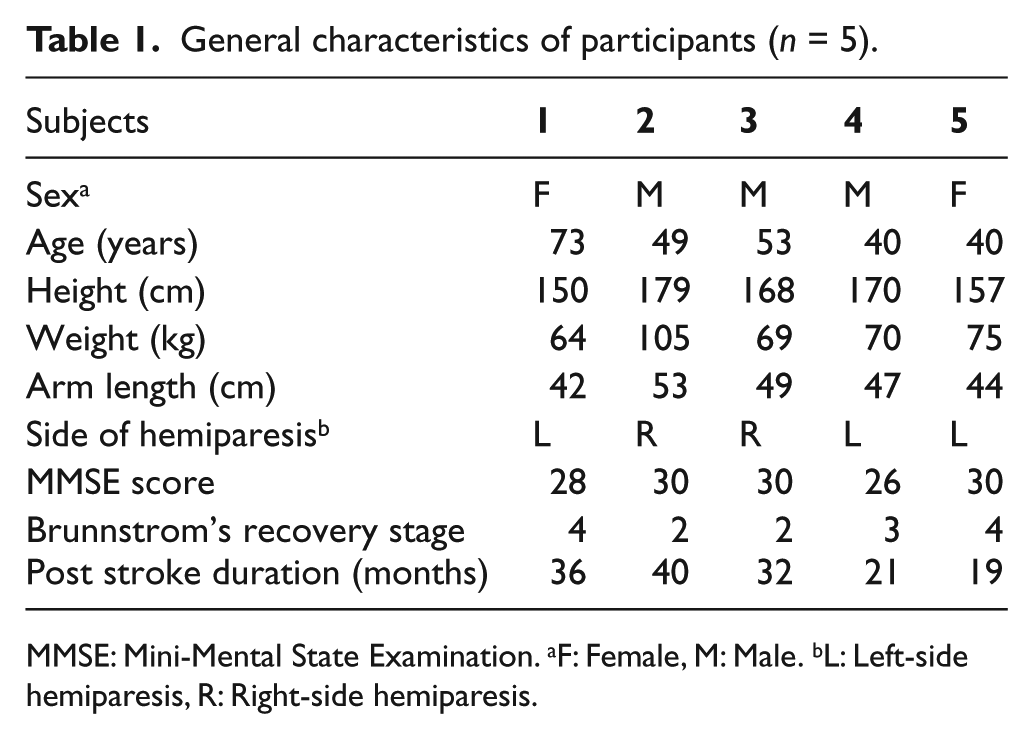
MMSE: Mini-Mental State Examination. aF: Female, M: Male. bL: Left-side hemiparesis, R: Right-side hemiparesis.
Intervention
The advantage of using a SaeboFlex orthosis was that activities could be performed even though patients wear the splint, so that training was considered to involve activities. Each finger sleeve is attached to the springs by a high-tensile polymer line in order to provide assistance with finger extension. Spring tensile strength can be adjusted for the appropriate amount of finger extension assistance needed, and the orthosis has no motor or electrical parts (Figure 1).
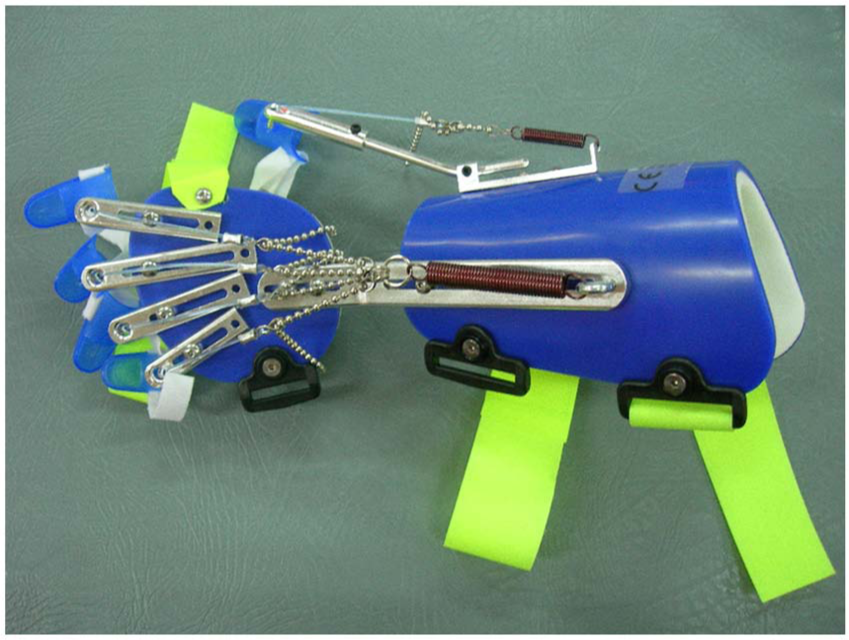
SaeboFlex orthosis.
Training activities for the experimental group consisted of 20 sessions (five times per week): typically 1 h per session. Each session consisted of nine task-oriented practice sessions using the hemiparetic arm and one rest period. Practice tasks were conducted with the patients wearing the SaeboFlex orthosis. Tasks for the training program were as follows: (1) moving a soft ball from the side of the affected foot to the table, while seated; (2) moving a soft ball diagonally from the less-affected side to the affected side while standing; (3) moving a soft ball diagonally from the affected side to the less-affected side while standing; (4) moving a soft ball from the left to the right side on the table while standing; (5) moving a soft ball from a box, situated at knee height on the affected side, to a table while standing; (6) moving a soft ball through the target from the left to right side while standing; (7) grasping and releasing a soft ball to straightly forward and backward transfer on the table while standing; (8) grasping and releasing a soft ball to diagonally forward and backward transfer on the table while standing; and (9) moving a soft ball from a cup to a cup on the table while standing. Each task was performed for about 5–6 min.
Outcome measures
Clinical assessments
The outcome measures for clinical assessments were the ARAT, FMA, and BBT. The ARAT is a relatively short and simple measure of upper extremity function for stroke patients. The test–retest reliability (ICC) value of ARAT reported in an ARAT-related study of 50 patients with stroke was 0.98. 16 Inter-rater reliability as reported in an FMA-related study with 37 stroke patients was 0.99, and test–retest reliability was 0.97. 17 Inter-rater reliability reported in a BBT-related study of 37 stroke patients was 0.99, and test–retest reliability was 0.96. 17
Three-dimensional (3D) motion analysis
Spatiotemporal parameters were collected using a three-dimensional (3D) motion analysis system and workstation software pre- and post-test (VICON MX system, Oxford Metrics, UK). Data collection was conducted at the Motion Analysis Research Laboratory in the Yonsei University. A 6-infrared camera VICON MX system obtained kinematic data at 60 Hz, which was processed by Nexus 1.4 software. A total of 28 spherical retro-reflective surface markers were placed at bony landmarks directly on the skin, according to the guidelines of the VICON “upper limb” model marker-set. We defined the start and end of movement by Hingtgen et al. 18 Start and end of movement was defined as elbow flexion (beginning) to elbow extension (end). The jerkiness score of each axis at the joint characterizes the average rate of change of acceleration during the reach-to-grasp movement toward the target. 19
The patients performed two different reach-to-grasp tasks while seated in non-swivel, stationary chairs. Their feet were flat on the floor with a knee angle of 90°. Their trunk was secured to the chair back with a harness in order to prevent lateral and forward flexion and rotation, but still allowed scapular motion. The hand to be tested rested on a table on the ipsilateral side, such that the shoulder was at approximately 0° of flexion/extension and 0° of internal rotation. The elbow was at 90° of flexion; the wrist rested palm down on the table with the finger joints in slight flexion. The target used for the spherical grasping task was a soft, 10-cm diameter ball, and it was positioned for two different reach-to-grasp tasks: elbow and acromion height. The first position for the reach-to-grasp task was directly in front of the tested arm at 100% length and at elbow height, and the other position was directly in front at shoulder joint (level with the acromion), also at a distance of 100% length. The participants were instructed to grasp at their preferred speed. In this study, arm length was defined as the distance from the anterior axillary fold to the distal wrist crease when the subject raised his or her arm as close to 90° elevation as possible and reached forward (without trunk movement) as far as possible. For each reach-to-grasp task, the participants were provided with three practice trials prior to the actual reach-to-grasp tasks, and each task was repeated five times (for calculation of the mean data) with a 3 s rest between trials.
Data analysis
The parameters used for the data analysis were ARAT, FMA of upper extremity function, and BBT of clinical assessments, and a jerkiness score of movement smoothness for the shoulder, elbow, and wrist joints. A Wilcoxon signed-rank test was used to identify the training effects after the intervention. An alpha level of p < 0.05 was considered to be statistically significant. All statistical analyses were performed using the SPSS statistical package 15.0 (SPSS, Chicago, IL).
Findings and Outcomes
Table 2 shows the effects of intervention on hemiparetic extremity function in the group; the FMA of upper extremity score and BBT score increased significantly (p = 0.043). Table 3 shows the changes in jerkiness score after the intervention of the hemiparetic extremity. In the group, the jerkiness score of sagittal plane movement at the shoulder joint decreased significantly in the reach-to-grasp task at acromion height (p = 0.043), and jerkiness score of the sagittal plane at the elbow joint significantly decreased in the reach-to-grasp task at acromion height (p = 0.042). Jerkiness score of transverse plane movement at the elbow joint decreased significantly for the reach-to-grasp task at acromion height in the group (p = 0.042). The jerkiness score of the coronal plane and transverse plane at the wrist joint significantly decreased in the group after intervention. The jerkiness score of the coronal plane decreased from in the reach-to-grasp task at elbow height (p = 0.042) and at acromion height (p = 0.043). The jerkiness score of transverse plane movement at elbow height (p = 0.041) decreased in the reach-to-grasp task, and at acromion height (p = 0.042).
Clinical assessment score after intervention (n = 5).
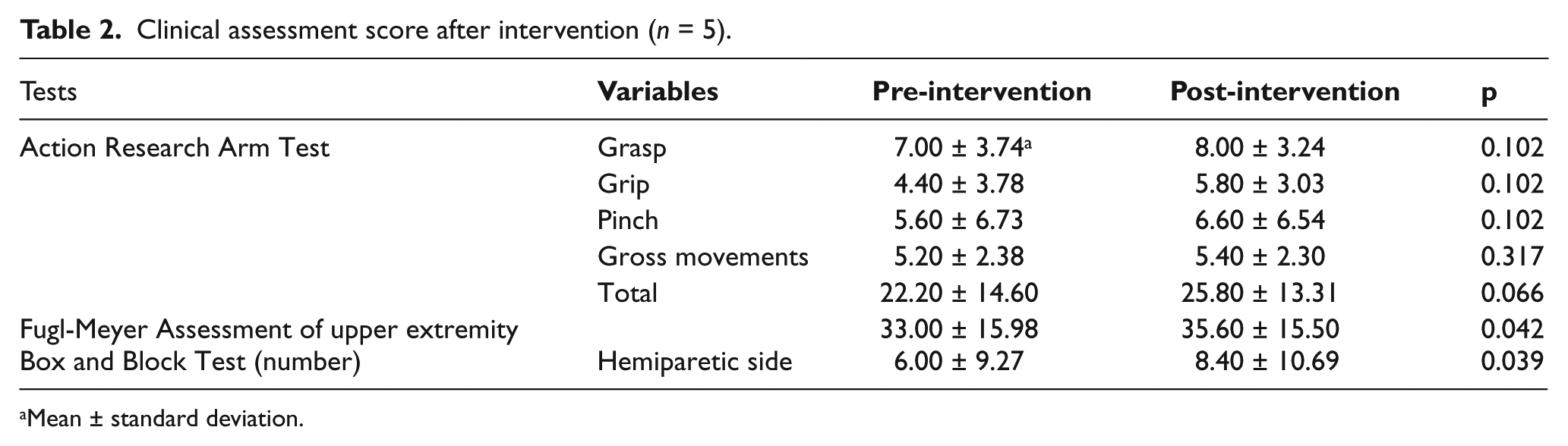
Mean ± standard deviation.
Jerkiness score (number) after intervention (n = 5).
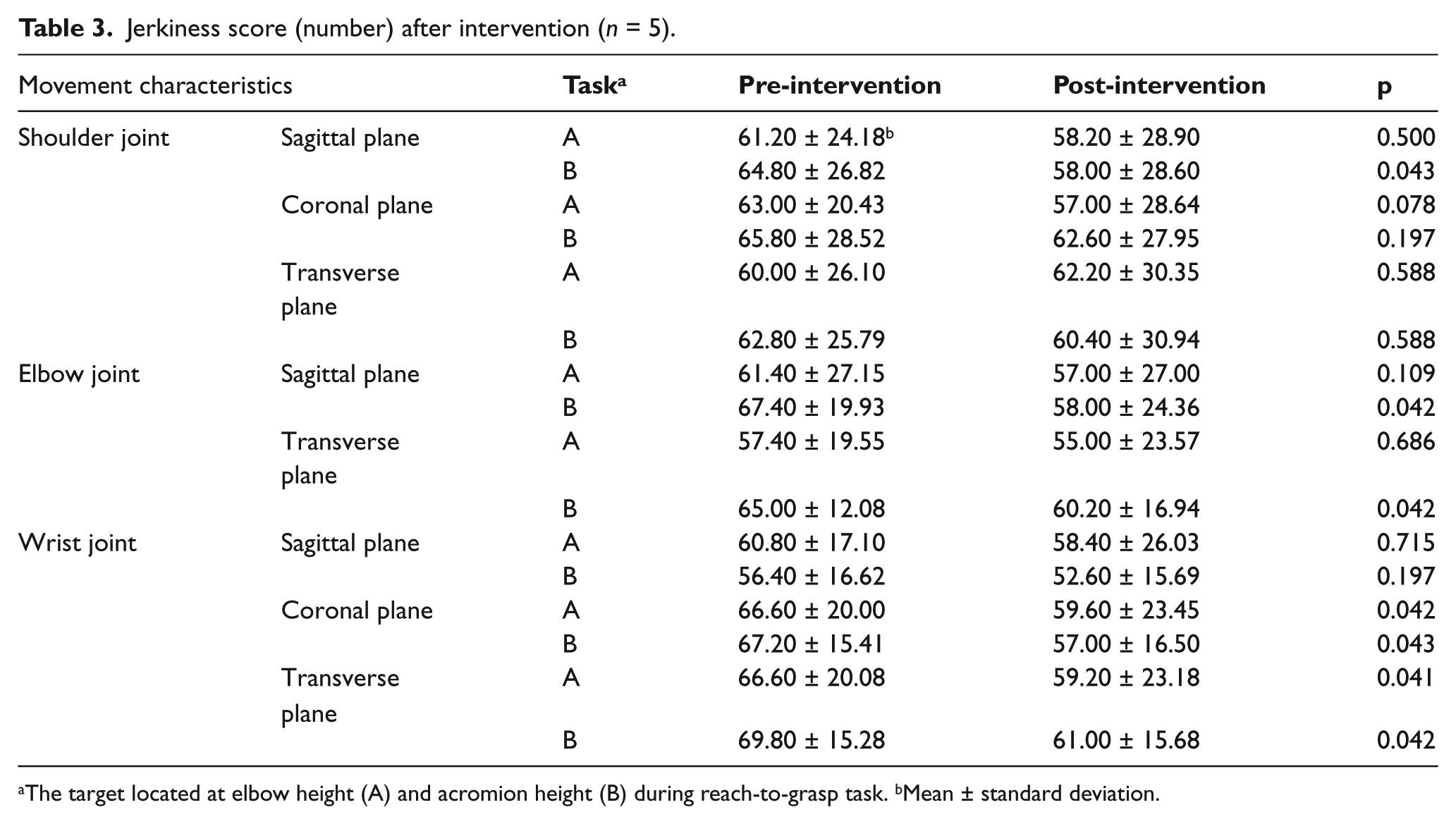
The target located at elbow height (A) and acromion height (B) during reach-to-grasp task. bMean ± standard deviation.
Discussion and Conclusion
In our study, we used clinical assessment and jerkiness score as kinematic parameters, for assessing recovering functions of the upper extremity during reach-to-grasp tasks in persons with stroke. These assessments of clinical assessment and jerkiness score were identifying gross motor skill ability at body structures and functions level, and activity levels based on International Classification of Functioning, Disability and Health (ICF) model by the World Health Organization’s (WHO) framework. Results of the assessments showed significant difference in the BBT score (p = 0.042) and the FMA score (p = 0.039). However, the ARAT score of subjects did not differ after the intervention in the group (p = 0.066), because of the ARAT was used to test grasp and grip performance for different objects, measure of fine motor skill, during each session, which the BBT tested performance in grasping similar objects.
In our study, a 3D motion analysis system was used to demonstrate the training effect of movement dysfunction as a replacement for assessment using an observation. 20 Commonly, the focus of the observation and evaluation during 3D motion analysis was how a performer’s upper extremity was coordinated in space and time during movement, using the parameters of velocity, and jerkiness score for movement smoothness.4,21 In the results of jerkiness score in our study, the jerkiness scores of movement in the sagittal plane of the shoulder joint significantly decreased during the reach-to-grasp task at acromion height (p = 0.043). Moreover, jerkiness scores in the sagittal (p = 0.042) and transverse planes (p = 0.042) of the elbow joint significantly decreased during the reach-to-grasp task at acromion height. In the wrist joint, the jerkiness scores of movement in the coronal plane and transverse plane decreased during the reach-to-grasp task at both heights significantly (p < 0.05).
Our results showed that the jerkiness scores of movement in the coronal and transverse planes of the wrist during the reach-to-grasp task at both heights significantly decreased. Moreover, jerkiness scores in the sagittal and transverse planes of the elbow joint, and sagittal plane of the shoulder joint, significantly decreased during the reach-to-grasp task at acromion height. These results indicated that there was limited need for shoulder movement during the reach-to-grasp task at elbow height; therefore, there was no significant change in the reach-to-grasp task at elbow height after the intervention. We confirmed that there was a decrease in the jerkiness of movement in the reach-to-grasp task sessions at higher positions.
Generally, in the hemiparetic upper extremity, movement increased jerkiness during the task.4,19 Therefore, the movement of upper limbs became smoother, less jerky, and more direct as recovery occurred in stroke patients. 22 The measurement of upper extremity performance in patients with stroke show jerkier, less accurate, less coordinated, and less direct movement paths, and fewer are well-timed during movement. 23 Arm movements in stroke patients had increased jerkiness, were longer, more segmented, more variable, and had larger movement errors.19,24–26 In this study, movement smoothness improved, as measured by jerkiness score, after the intervention. These results suggest that movements became less jerky, more coordinated, and well-timed during tasks undertaken in laboratory situations. These results indicate that recovery also continued in case of chronic stroke.
Most of important points for treating upper extremities after neurological injury involves intervention that is repetitive, and involves task-oriented training of the impaired extremity for several hours a day and constraining of patients to use the impaired extremity during waking hours. 2 The orthosis in this study was designed to provide splinting and repetition, task-oriented training, and mimicking of real-world activities for the hemiparetic upper extremity. Using the SaeboFlex orthosis has advantages in assisting finger extension for impaired grip opening caused by spasticity or flexor synergy. It allows the impaired hand to perform functional activities during training and is expected to facilitate use of the impaired extremity during functional tasks, which will carry-over into the real-world activities of daily living. Therefore, the spring-assisted hand orthosis system is considered to be an effective treatment option for undertaking task-oriented activities.
In this study, one limitation was that our sample size of stroke patients was quite small, and hence, there are some limits in generalization of the results of this study although we used non-parametric tests for statistical analysis. Therefore, further research is recommended using a larger patient sample size. Another limitation is that we did not mention about the spasticity level of participants directly, although it is another factor that affects the functional recovery of stroke patients. Because of spasticity is velocity dependent increase in tonic stretch of muscles due to central nerves system lesions and altered passive mechanical properties due to prolonged immobilization, but the most of clinical scales assessed by passive movement not a stretch reflex. Therefore, we use the clinical scales for Brunnstrom’s recovery stage instead of using scales for evaluating spasticity directly, because the latter do not exactly inform the characteristics of spasticity. 27
The results of this study indicate that the spring-assisted dynamic hand orthosis training is effective in kinematic parameters of the hemiparetic upper extremity of patients after stroke. Parameters, such as jerkiness score for movement smoothness, also improved in the hemiparetic upper extremity. Therefore, the spring-assisted dynamic hand orthosis training is considered to be a treatment option for clinical conditions. Further research is recommended using other parameters for effective evaluation of hemiparetic upper extremity and a larger patient sample size.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.