
Abstract
Background:
A divide is experienced between producers and users of evidence in prosthetic rehabilitation.
Objective:
To discuss the complexity inherent in establishing evidence-based practice in a prosthetic rehabilitation team illustrated by the case of prosthetic prescription for elderly dysvascular transfemoral amputee patients.
Study Design:
A qualitative research design was used, in which data from multiple sources was triangulated to extract themes for discussion.
Methods:
This discussion paper draws on empirical material gathered by individual and focus-group interviews with members of a prosthetic rehabilitation team, information on technological advancements presented on websites of orthopaedic industry, guidelines and literature study.
Results:
A prosthetic rehabilitation team needs to deal with lack of evidence, contradictory results, various classification systems, diverging interests of different stakeholders and many modifying factors, and all of this in a continuous technological changing environment. Integrating research designs with different strengths but not sharing the same biases may help researchers to deal with the multimorbidity and multifaceted disability of the target group. Articulating clinical knowledge, patients’ needs and values in a systematic way provides depth, detail, nuance and context for evidence-based practice issues in prosthetic rehabilitation.
Conclusions:
Reconsidering the relationship between evidence, technology and rehabilitation practice is an imperative shared enterprise for clinicians and researchers. Scientific, clinical and patient-related knowledge are seen as important knowledge practices that should inform and strengthen each other.
Clinical relevance
This discussion paper puts the academic clinical debate on evidence-based practice in prosthetics and orthotics in another light. By demonstrating the complexities surrounding evidence-based practice, it is argued and illustrated how both researchers and clinicians can contribute to optimal patient care in which evidence, technology and rehabilitation practice are integrated.
Background
Evidence-based practice (EBP) is growing in the field of Prosthetics & Orthotics (P&O), and its importance is emphasized.1–4 Establishing an EBP is considered as highly relevant in a time of increasing pressure on health service budgets for all health-care branches. 5 Rehabilitation researchers have been quite successful in proving that multidisciplinary rehabilitation assessments and treatments are effective in optimizing the functional recovery after acute injury/disease and during chronic illness.6–8 At the same time, there is mounting awareness of the complexity in establishing a coherent evidence base for multidisciplinary rehabilitation: that is, in determining, translating and integrating external evidence from systematic research on different patients in improved and more efficient assessments and treatments for rehabilitation settings. This definitely yields for clinicians working in prosthetic rehabilitation with lower-limb amputee patients. 9
In line with Sackett et al.’s 10 definition of evidence-based medicine (EBM), EBP in prosthetic rehabilitation is characterized as the process of integrating individual clinical expertise and patient values with the best available evidence from systematic research, in order to provide the best clinical care.1–4 This definition comes across as attractive. It gives the impression that it is the ‘simple’ task of (rehabilitation) clinicians to combine original evidence produced in different research settings with their own individual clinical expertise including the individual needs of patients to whom they wish to give the best treatment. Of course, it is not that simple. A number of practical barriers in performing EBP are to be dealt with, such as lack of high-level evidence in P&O, time constraints and workload demands experienced by clinicians and finally limited skills, knowledge and resources required to perform EBP.1–4 Researchers interested in P&O point variously to limitations in both research and practice hindering the evidence-based integration process. A culture change is plead for, in which clinicians in P&O are to be educated as lifelong, self-directed learners and are encouraged to pursue relevant clinical research themselves. 3 In this discussion paper, it will be argued and illustrated that the evidence-based integration process implied in EBP is an extremely complex task in general, and in prosthetic rehabilitation in particular, and should therefore be considered as a shared enterprise of both clinicians and researchers.
Methods
This discussion paper stems from a broader research project aimed at narrowing the experienced divide between research and practice in multidisciplinary rehabilitation. Inspired by theory-driven programme evaluation,11,12 participatory action research,9,13,14 and social studies of science,15,16 questions about the complexity of EBP are addressed from the perspective of rehabilitation clinicians. In this discussion paper, the case of prosthetic prescription for older dysvascular transfemoral amputee patients is explored. The argument presented here draws on the following: (1) empirical material gathered by individual interviews and a focus-group interview with members of a prosthetic rehabilitation team, (2) information on technological advancements presented on websites of orthopaedic industry and the clinical practice guideline for rehabilitation of lower-limb amputation and (3) prosthetic rehabilitation literature and literature on the research–practice divide.
For the empirical part of the study, first individual interviews and a focus-group interview were conducted with members of a multidisciplinary prosthetic rehabilitation team in a Dutch rehabilitation centre. The rehabilitation centre is part of a university medical centre. Two physiatrists, five physical therapists, two occupational therapists and one prosthetist participated in the interviews. All professionals provided informed consent. The interviews were recorded and transcribed verbally. S.v.T. asked individual respondents about the motives behind their actions in prosthetic prescription and prosthetic training and about the impact of technological advancements on their actions. They were also asked about the sources they used to keep up to date with technological advancements. An independent experienced moderator led the focus-group interview on topics that needed to be further explored. The prescription of a knee mechanism for transfemoral elderly amputee patients was taken as case in order to make the discussion more concrete. The moderator also gave room for reflections on new topics that arose in the efforts of participants to understand each other. Based on these interviews, a scene was sketched of clinicians that needed to operate in a complex health landscape in order to perform EBP.
Second, the websites of two orthopaedic industries (Otto Bock and Össur) were explored, as these were used by the clinicians to keep up to date with the technological possibilities. The clinical practice guideline for rehabilitation of lower-limb amputation 17 was also added as a source of information for implementation of EBP.
Third, the scientific literature on prosthetic rehabilitation and on the research-practice divide collected by our research group within the past 10 years was studied to explore the scientific context. The literature studies were not conducted in a systematic manner, as is required for systematic reviews summarizing and critically appraising published evidence on certain issues. Indeed, our intention was neither to give an overview of the research-practice debate nor to present evidence for prosthetic rehabilitation that is methodologically generalizable. Rather, we wanted to reflect from a scientific point of view on issues and on-going dilemmas the rehabilitation clinicians had to face in attempting to work in an evidence-based manner and explore promising solution directions in the scientific literature.
The themes that emerged from the empirical and scientific material across sources are (1) the methodological complexity in research on elderly amputee patients, (2) the impact of technological advancements on evidence-based prescription, (3) diverging classification systems in prosthetic prescription and (4) additional modifying factors in the transfer to individual patients. With this discussion paper, we invite both researchers and clinicians to comment on the solution directions we recommend and participate in the academic debate in a shared effort to establish EBP in P&O.
Results
Methodological complexity in research on elderly amputee patients
In EBM, proofs of effectiveness of treatment are preferably assessed in clinical trials and its evidence summarized and critically appraised in systematic reviews. Most systematic reviews judge research findings on a basis of a hierarchy of study designs, with randomized controlled trials (RCTs) at the top, producing the highest level of evidence, and case studies at the bottom, producing the lowest level of evidence. RCTs are placed on the top of the hierarchy, as they are best suited to rule out threats to internal validity. Therefore, RCTs are preferably carried out on homogeneous populations of adult patients who are preferably not older than 65 years and who have only the condition in question. 18 Indeed, most research and clinical practice guidelines are based on a single-disease paradigm, which may not be appropriate for elderly patients with complex and overlapping health problems. 19 Optimizing the care of older persons with multiple medical conditions is therefore a complex task, with clinicians receiving potentially contradictory recommendations regarding how to tailor care for elderly from the medical literature. 20 The majority of the patients in the field of P&O for whom clinicians need to make evidence-based decisions are also elderly with two or more morbidities such as diabetes and vascular diseases.21,22 That introduces bias into data, which makes it difficult to get conclusive evidence for this complete target group. Excluding patients based on confounding factors such as multimorbidity results in a more homogeneous group and more conclusive results but at the same time limits the applicability of research findings for the complete group. Therefore, exclusions made by researchers to prevent bias entering the research setting in order to produce methodological sound and generalizable results, do not resolve the complexity of the clinical decision process in prosthetic rehabilitation of older dysvascular amputee patients.
Although researchers in the field of P&O do recognize the complexity of the research in question, many of them continue to rely above all on the traditional study design hierarchy articulated in the EBM movement. Cumming et al., 21 for instance, concluded in their systematic review on older dysvascular amputee patients that more reliable evidence from high-quality and sufficiently powered RCTs on interventions is needed. They could include only one trial in their systematic review, a trial of which the methodological quality was judged as moderate because of lack of power (only 10 patients), a missing description of the randomization, no intention to treat analysis, lack of point estimates and measures of variability presented for the primary outcome measures, and so on. 21 The researchers explained that they conducted this study because they felt that the results of the previous studies on their research topic might not be directly attributable to the older less active poorly conditioned dysvascular amputees. 23
Thus, researchers are urged to conduct high methodological quality in experimental settings (internal validity), on the one hand, and need to ensure applicability of the research findings for the wider population seen in clinical settings (external validity), on the other hand. A relative neglect of external validity in the EBP health literature is reported, which does have consequences for the relevance, generalizability and applicability of the research findings in varied circumstances in clinical settings. 24 In the light of an ageing society, in which clinicians will face more and more older people with multimorbidity and multifaceted disabilities, there is an urgency to incorporate other research designs for this heterogeneous group. We therefore argue that researchers working in the field of P&O should reconsider traditional study design hierarchy, where appropriate, and explore other options like mixed methods research.
Mixed methods research can also provide high internal validity and at the same time offer the opportunity to deal with the heterogeneity of amputee characteristics. It involves the combination of two or more research designs having different strengths and not sharing the same biases. 25 Often mixed methods research refers to the combined use of both quantitative and qualitative methods, in which the researcher collects and analyses the data concurrently or sequentially, integrates the findings and draws inferences using both methods in a single study or programme. 26 In post hoc evaluations for instance, qualitative examination can identify why differences in intervention outcomes occurred, uncover additional treatment benefits and explore barriers to achieving the best intervention outcomes. 27 But the approach of mixed methods research can also encompass combining different qualitative methods such as in-depth interviews, focus-group discussions, documentary analyses or observations.9,28 Mixed methods research may thus assist in enhancing internal validity in a heterogeneous research population as well as balancing issues of internal and external validity. To our opinion, researchers in prosthetic rehabilitation could and should therefore profit from this ‘new’ research approach that can provide evidence that is better attuned to the variability of prosthetic rehabilitation and heterogeneity of the target group.
Impact of technological advancements on evidence-based prescription
Emerging technological advancements in prosthetics is another aspect that adds to the complexity in establishing EBP in P&O. Due to these advancements, clinicians face an overwhelming amount of available prosthetic componentry from which they have to choose. 29 A problem is that empirical evidence on the surplus value of novel prosthetic componentry in relation to existing technologies comes quite some time after the innovations have been put on the market. Let us take the developing technology in prosthetic knee mechanisms as an example. Knee mechanisms must provide stability and swing at appropriate rates to properly match an amputee patient’s ability. 30 Several orderings in available knee mechanisms can be distinguished.
In the interviews, clinicians illustrated the impact of developing technology on their clinical decision process as follows; in former days, it was relatively simple: clinicians and their patients could choose between several passive knee mechanisms comprising locked knee mechanisms and free swinging mechanisms. Interviewed clinicians elucidated that when they were in doubt about the most appropriate knee mechanism in former days, they chose a manual locked knee mechanism because of its safety. After prosthetic training, they could then decide whether a free swinging knee mechanism was optional for the longer term. With the invention of, for example, stance and swing phase control techniques, free swinging knee mechanisms got more and more sophisticated. These novel mechanisms became applicable for a wider variety of patients. For the clinicians in the local setting, this led to an actual shift in the prescription of prosthetics. They reported that nowadays they mostly select a free swinging mechanism with stance-control technique, and when that does not work out well, they can still choose a locked knee mechanism. The clinicians rationalized their choice for this sequence by arguing that it fits the learning strategy that patients use to incorporate the mechanism of the prosthesis in their movements. They argued that it is very hard for a patient to unlearn a ‘stable’ movement pattern A (locked mechanism) and learn movement pattern B (free swinging mechanism) that is far more unstable. That is why they now often choose to start with the free swinging mechanism.
For elderly dysvascular amputee patients, however, issues like muscle weakness, loss of coordination and balance are common additional conditions. Therefore, patient safety is a primary concern for clinicians. 31 With the incorporation of several electronic control systems into prosthetic knee mechanisms, the range of available knee mechanisms is again broadened. 32 In these active controlled knee mechanisms, microprocessors direct the knee’s resistance to flexion and extension, thereby influencing a user’s ability to ambulate safely and/or effectively. 31
Most interviewed clinicians, however, clarified that they barely prescribed microprocessor controlled knee mechanisms (MKMs) for the older transfemoral amputee patients. They felt that most of these prostheses were developed for younger, more active patients. Nonetheless, there were also clinicians who pointed to advantages: that is, MKMs might require less cognitive demand for older amputee patients, who find it in general harder to conduct dual tasks. This might attribute to the safety of their functioning. But even then, prescription of MKMs remains a complex activity. The interviewed clinicians reported that the relative high costs of MKMs lead to resistance by health insurers. When they decided to take advantage of innovative technology in MKMs and prescribe a prosthesis with such a knee mechanism for an elderly patient, health-care financers were not eager to pay for it.
Clinicians in prosthetic rehabilitation thus not only have to keep up-to-date with the technological advancements and fit its pros and cons in their prescription process, but they also have to take into account the interests of other stakeholders such as the care financers of their patients. There is thus an urgent need for evidence in P&O: first, to support clinicians in making evidence-informed prosthetic prescriptions for different target groups, and second, for grounding that prescription towards health-care financers. Lack of evidence to support clinicians in the prescription process is indeed experienced as a huge barrier.21,33 In a meeting on the state of the evidence in P&O, the ‘science’ of P&O was even referred to as severely immature. 34 The scientific literature on MKMs, for instance, showed mixed results on energy expenditure, gait performance and cognitive demand, while users’ satisfaction was globally positive. This is confirmed by a recent survey with prosthetists and orthotists, who also felt that research studies presented too many contradictory results, and what is more, the research findings were considered out of date. 1 Contradictory research findings and various opinions about prescription of MKMs are among other things attributed to a lack of knowledge on the exact target group for MKMs. Are the most technologically advanced prosthetic components only suitable for the young athletic amputees or can patients with a lower level of functioning also profit from this technology?31,35 The possibilities nowadays seem endless, but at the same time, clinicians in prosthetic rehabilitation are warned for too much optimism: when an individual is unable to ambulate with a nonmicroprocessor knee, there is little chance that he or she is able to ambulate and benefit from the features and functions of a MKM. 36 More conservative components are often prescribed for patients with limited mobility, although several studies provided evidence that can counter this presumption.29,31
Therefore, advancements in technology certainly have an impact on clinical practice, and contradictory evidence on these advancements contributes to the complexity of EBP in P&O. Clinicians, researchers and designers are seen as important actors in this combined field of technology, research and prosthetic rehabilitation. We therefore applaud initiatives that stimulate the multi-actor process in which all stakeholders combine their knowledge. Meetings in which clinicians, prosthetic users, researchers and prosthetic device manufactures 37 or where prosthetists, orthotists, user representatives and research engineers 34 come together in order to attune their agendas on research projects on prosthetic technology are seen as promising examples.
Diverging classification systems in prosthetic prescription
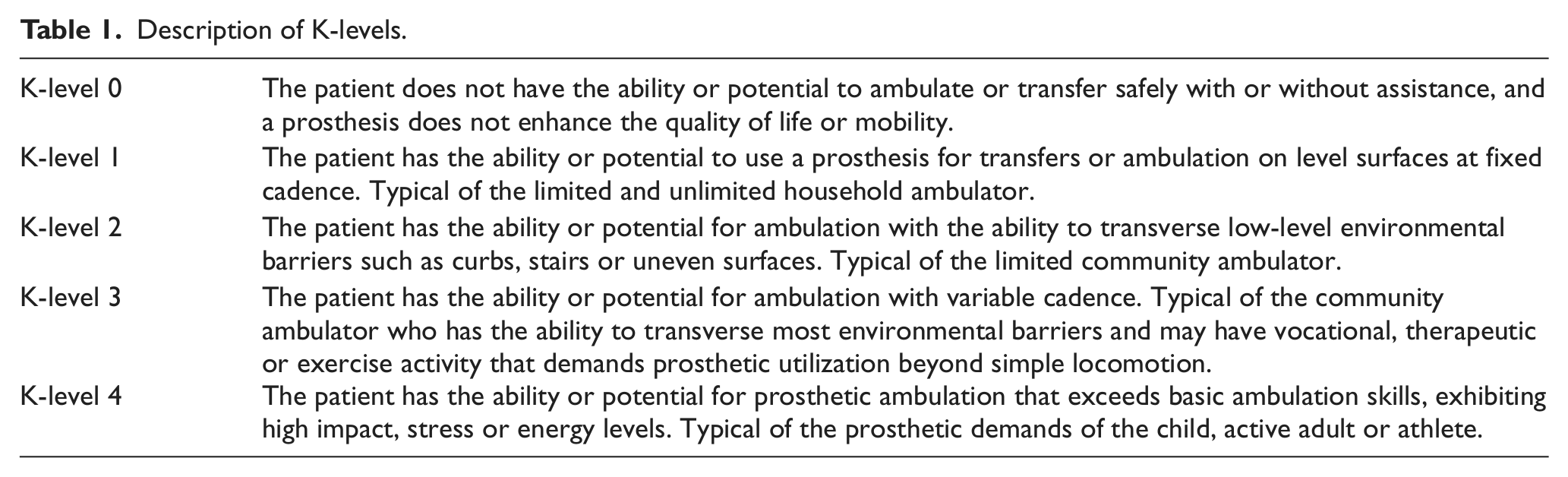
Despite contradictory results and various opinions influencing clinicians in their decision process, there are evidence-based guidelines available for clinicians. These clinical practice guidelines for rehabilitation of lower-limb amputation dedicate two subparagraphs to the prosthetic prescription phase. Clinicians are recommended to determine functional goals of prosthetic fitting (D1) and prescribe the prosthesis based on the current or potential level of ambulation (D2). 17 To determine the potential level of functioning, the guidelines refer to the use of K-levels. K-levels stem from a coding system of the Health Care Financing Administration (HFCA), comprising a 5-level functional classification system ordering the functional abilities of persons who have undergone lower-limb amputation. 38 This system was originally developed to assist a health-care insurance company (Medicare) with the decision which prosthetic components to cover but is now also incorporated in the guidelines to support clinicians in the prescription process. The K-level system can assist clinicians in selecting available componentry that is indicated for the specific K-levels. When a patient is resided in K-level 2, for instance, a prosthesis that meets the functional goals of limited community ambulation is recommended (see Table 1).
Description of K-levels.
The question, however, is how patients will be assigned to a certain K-level. Especially when taken into consideration that patients are being evaluated on their potential, which could affect their future care as with Medicare patients. Therefore, it is important that what constitutes potential is standardized and measurable. 39 The clinical guidelines nevertheless do not provide direction for this selection. It is again the clinician or the rehabilitation team that has to determine the skills and features of the patient and combine that with the desired level of participation of the patient. Therefore, this recommended classification system depends heavily on subjective procedures and clinical expertise of the rehabilitation team. The evidence-based guidelines thus implicitly pass the responsibility to clinicians.
With the involvement of another stakeholder, the orthopaedic industry, the use of the classification system as a helpful instrument for clinical decision-making gets even more ambiguous. Certainly since providers, like Össur 40 and Otto Bock, 41 present their own ‘unique’ classification systems on their websites. Otto Bock presents a classification system that is named the MOBIS-Otto Bock mobility system with levels that are called ‘mobility grades’, and Össur presents a classification system with ‘impact levels’. The four mobility grades of the MOBIS-Otto Bock mobility system resemble the K-levels 1–4, omitting K-level 0, as this indicates no prosthesis. Both the MOBIS-Otto Bock system and the K-level system base their levels on the possibilities of the amputee to perform certain transfers, on which surface and with a certain kind of cadence. The impact levels of Össur, however, present ranges of activities and focus on the loading force (minimal, moderate amount, high and extreme). The activities like shopping, gardening and household tasks are, for instance, linked to the low impact level. Although all three classification systems do have common features, they diverge in terminology and content. It is understandable that different industrial ventures wish to present their products as exclusive and therefore introduce their own ‘unique’ classification system. Yet for clinicians who need to decide on prosthetic componentry, this leads to more unnecessary complexity. We therefore argue to further work in a joint manner on a more standardized classification system that is attuned to the needs of clinicians and their patients.
Transfer to individual patients: additional modifying factors
The functional abilities as categorized in the classification system recommended by the guidelines are indeed not conclusive for the clinical decision process in the prescription phase. Also physiological factors – including general health, weight, height, level of the amputation and length and shape of the residual limb – are to be considered when prescribing a prosthesis. According to the suppliers of prosthetic componentry, it is therefore not possible to offer an exact prescriptive tool online. 40 In addition, also psychosocial factors need to be considered in the choice of componentry.
Interviewed clinicians emphasized within this context, the impact of fear of falling, which is present by many older amputee patients. According to them, a disabling fear of falling has a negative impact on autonomous movement, which endangers safe functioning. Therefore, in order to succeed with the prosthetic fitting, elderly amputee patients must feel confident enough to deal with the knee mechanism.
The scientific literature, however, provides little insight into the predictive character of the different physiological and psychosocial factors. Therefore, also on these issues scientific knowledge is lacking to inform clinicians in prosthetic rehabilitation. Even of greater importance for a good prescription of prosthetic componentry are the wishes and preferences of patients themselves. Considering all the advancements in technology, it is necessary to examine what patients prefer. Several researchers have actually focused on the patients’ perspective on prosthetics including the role of advancements in prosthetics.42–44 They expressed their concern that patients’ preference into the decision process lacks intention. They plead for standardized methods in which to measure patient preferences within prosthetic prescription. In this technology-driven time frame in prosthetic rehabilitation, clinicians should be well aware of the patients’ psychosocial issues and patients’ emotions and feelings towards technological devices. 43
These researchers42–44 thus impute an important role for clinicians in rehabilitation to balance the functional opportunities offered by technology with a holistic view on the patient. We argue that researchers themselves can also fulfil an important role in this balancing process. Combining several qualitative research techniques provides a fuller and deeper understanding of a certain issue. 45 With the help of in-depth interviews individual perceptions, beliefs, feelings and experiences with prosthesis can be identified. 28 Focus-group discussions can accordingly be used to gain in-depth understanding of the values of subgroups of patients and about the acceptance and use of certain prostheses, thereby comprising more comprehensive knowledge on the issue. Researchers can provide clinicians in this way with in-depth knowledge about the grounds underlying articulated patients’ values and preferences by giving words to the voices of elderly patients and their caregivers in the field of P&O.
Explicating and comparing the tacit knowledge of clinicians working in P&O
There is not a simple recipe for prosthetic prescription that supports clinicians in the implementation process of EBP of lower-limb amputee patients in general and elderly dysvascular amputee patients in particular. The selection of the right componentry for a prosthesis cannot easily be made by summarizing and critical appraising available evidence in systematic reviews. To the contrary, clinicians do face a lack of evidence and when available contradictory results. On top of that, they have to deal with various classification systems, diverging interests of different stakeholders and many modifying factors, and all of this in a technological changing environment. In their search for an optimal prosthesis for individual patients, clinicians are thus confronted with many uncertainties and unidentified knowledge areas that contribute to the complexity of evidence-based prescription in P&O. The rehabilitation team therefore relies for a great part on their own clinical experience to select the right prosthesis for an individual patient. In the individual and focus-group interviews, clinicians described the prescription phase in this context as ‘an art’, ‘a sensitivity’, or ‘something speculatively’. Unfortunately, this so-called tacit knowledge is scarcely made explicit in prosthetic rehabilitation, which does not attribute to transparency in the field of P&O. This is a well-known problem and also seen in other fields. It is indeed acknowledged that it is difficult for clinicians in general to put the reasoning behind their decisions and actions into words.46,47 Clinical knowledge is understudied and needs more articulation to make it transportable for sharing and thus for improvement. 48 How to profit from this area of clinical knowledge and expertise?
Participatory action research can be of great help in explicating this implicit knowledge of clinicians and can also be helpful in facilitating improvement. The participation part in participation action research implies that clinicians are seen as partners in the research process, and the action part defines the commitment to change. 28 Participatory action research aims at (1) conducting research with people, not on people; (2) improving the situation and (3) learning and reflection between the researcher and researched. 28 Researchers trained in participatory action research can assist clinicians to make their implicit practical knowledge explicit with help of documentary analysis, observations of treatments, individual and focus-group interviews and so on. By incorporating clinicians as partners in a research process, the researcher and clinicians can co-construct knowledge. 49 In a previous study, 9 a participatory action research design helped us to collect, unravel and articulate tacit knowledge of clinicians in prosthetic rehabilitation on specific issues, which was accordingly specified by asking clinicians to critically reflect on them in focus-group discussions. Through this articulation process, we were able to identify the essential issues for improvement of the intervention and its conceptual underpinnings in terms of problem-solving principles and practices.
Participation research, however, demands several skills of the researcher. To be able to articulate knowledge from an insider point of view (tacit knowledge of clinicians), researchers must have the skills to put themselves in the shoes of clinicians. From an outsiders point of view, they accordingly have to be able to put together the articulated knowledge in conceptual frameworks developed to work on programme development.9,11,12 For example, they have to be able to specify systematically the treatment content (the features of the interventions, recipients and their environment) and its theoretical underpinnings. With this knowledge, treatment outcome research can be designed that can enhance both the understanding of research findings and their usefulness in rehabilitation practice.11,12
We thus argue that participatory research provides depth, detail, nuance and context to EBP issues. Explicating the implicit knowledge of clinicians can contribute to a better understanding of clinical decision processes and can examine issues that are too complex to be easily disentangled by clinical epidemiological research. Integrating clinicians and patients in the research process involves recognizing the rights of those whom research concerns, enabling people to set their own agendas for research and development and so giving them ownership over the process. 13
Discussion
In this discussion paper, we have unravelled and explicated the problems that clinicians encounter when they want to implement the results of scientific research into practice of the P&O field. We focused on just one part of prosthetic rehabilitation, namely, the prosthetic prescription phase for older dysvascular transfemoral amputee patients and in particular on innovative technology of knee mechanisms. We illustrated that clinicians motivated to work on EBP in a lifelong manner not only need to handle a number of practical barriers in performing EBP but also have to be in accord with emerging technological advancements in this field 50 and are on top of that asked to translate the collective and averaged body of external evidence (when available) to the individual needs of their patients. 2 This means that a lot is asked from clinical and academic reasoning of clinicians in their effort to perform EBP. Certainly when taken into consideration that a prosthesis encompasses much more componentry than just a knee mechanism like ankle and foot mechanisms. All these mechanisms interact with each other, which increases the complexity of the prescription of the right componentry.
We argued that it is a shared responsibility of both clinicians and researchers to deal with the complexity in P&O and rethink the relation between evidence, technology and rehabilitation practice. This implies that researchers have to learn to experiment with the many shades of grey designs that lie between black (case studies) and white (RCTs) designs, in order to provide scientific knowledge that will be better attuned to the complexity seen in clinical practice. Take the elderly dysvascular amputee patients, their multimorbidity and multifaceted disabilities indeed influence the linear relationship between experimental interventions and outcomes presumed in clinical trials thereby confounding research results. Adding qualitative research on the situated perceptions and experiences of the researched elderly will provide researchers with more detailed knowledge on the confounding factors. These findings will help them to place the quantitative data in perspective. It could be stated that in experimenting with the research designs, researchers also have to become lifelong learners, just like the clinicians, as was plead for in the culture change in P&O. 3 It would even mean a culture change for funders, publishers and educators to enable, teach and support such research designs.
The role of clinicians in establishing EBP in P&O can also be seen in another light. Clinicians need to deal with several complex issues when they are asked to integrate individual clinical expertise and patient values with the best available evidence. This holds for rehabilitation medicine in general and prosthetic rehabilitation for elderly dysvascular amputee patients in particular. To put it more encouragingly, it can also be said that clinical decision-making in rehabilitation practice requires craftsmanship, creativity and pragmatic considering and assembling of all multifaceted aspects. 16 Explicating this craftsmanship, creativity and resourcefulness, which clinicians make use of when dealing with the complexity, is of great importance. This is still a blind spot in rehabilitation research that does not do justice to the hard work of rehabilitation clinicians. The articulation of clinical practice as having a quality and logic of its own is a first step in the quest for more situated strategies for the improvement of rehabilitation practice. 16 Although there is the tradition of writing case reports and transferring clinical knowledge through medical education, researchers seldom reflect on clinical experience as a form of knowledge in itself. The practical knowledge of patients is even less studied and reflected on. 48 It is therefore important to distinguish between evidence-based knowledge produced in experimental settings, clinical knowledge gathered by assessments and treatments of patients and practical knowledge from patients living with a condition or disease.
With this, we touch upon a more fundamental question being: is the term based in ‘EBP’ in this perspective an accurate term? If we argue that research evidence produced in experimental settings should not override, or take precedence over, clinical experience, clinical embodied skills, patients’ needs, values and knowledge, then the relationship between evidence and practice cannot be that of supplying a basis for that very practice.9,15,51 It is of course important to critical appraise rehabilitation practices in experimental settings and conduct creative scientific investigations that may help to (im)prove it. But we suggest that all three knowledge practices, scientific knowledge from researchers, clinical knowledge from clinicians and practical knowledge from patients are important and should inform and strengthen each other. We therefore propose to replace the term based in EBP for informed. In evidence-informed practice (EIP), clinicians are encouraged to be knowledgeable about the findings coming from all types of scientific studies, and researchers are urged to support them in translating it to the local realities of different rehabilitation settings in an integrative manner.9,51
Conclusion
Researchers should learn to take into consideration both articulated clinical experiences and judgments, clients’ preferences and values, context of intervention and relevant evidence produced in experimental settings and help clinicians to attune it to each other. In our opinion, EIP acknowledges both the crucial role and craftsmanship of the clinician and the researcher in providing the knowledge for the performance of optimal patient care in prosthetic rehabilitation.
Footnotes
Conflict of interest
The organization that sponsored the study was not involved in its design, data collection, data processing or manuscript preparation. None of the authors have financial or personal conflicts of interests.
Funding
For preparing this article, data were used from a study that was funded by Stichting OIM, the Netherlands.