
Abstract
Background:
Scottish-Rite orthosis is one of the conservative methods used to treat Legg–Calvé–Perthes disease. As there was not enough evidence to show the effects of using this orthosis on reducing the loads applied on the limb, this research aimed to find the influence of this orthosis.
Case Description and Methods:
A participant with Perthes disease on the left hip joint was recruited into this study to walk with and without the orthosis. The kinetic and kinematic parameters were collected by a motion analysis system and a Kistler force platform.
Findings and Outcomes:
No significant differences were noted between the hip joint flexion/extension range of motion and the moments between the sound side and the side affected by Legg–Calvé–Perthes disease. It may be concluded that use of orthosis may not have any positive effects to decrease the loads or to improve the alignment of the hip joint in participants with Perthes disease, as expected.
Conclusions:
The use of Scottish-Rite orthosis not only does not improve the containment of the hip joint, but also does not have any significant influence on loads applied on the joint during walking of the subject with Perthes disease.
Clinical relevance
The results of this research can be used by clinicians involved in treatment of patients with Legg–Calvé–Perthes disease.
Background
Legg–Calvé–Perthes Disease (LCPD) is a condition in which the blood supply of the femoral head is disrupted and as a result the bone temporarily dies. Depending on the severity of the disease, this leads to irritability of the hip bone and finally deformation of the femoral head can result. Although it is claimed that genetic or deprivation factors influence the incidence of this disease, its etiology is likely to be multifactorial and is not clear. 1 It occurs in children aged between 5 and 12 years, and its incidence is 10.8 per 100,000 for White and 0.45 per 100,000 for Black children.2–4
There are some problems associated with the Perthes disease, which include decrease in the hip joint’s range of motion and alternation in the growth of the femoral bone and also pain while walking.5 –10 Various types of methods have been used to treat LCPD, which are divided into operative and nonoperative methods. In nonoperative methods, various types of orthoses such as Scottish-Rite, ischial weight-bearing, Newington, and Birmingham orthoses have been used by the patients. Whereas, surgical treatments include pelvic and femoral osteotomies to increase the containment of the femoral head within the acetabulum.10 –19
Although the original prescription of Perthes disease occurred nearly 100 years ago, the treatment remains controversial, and there is a lack of agreement regarding the best treatment protocol for the patients.10,11 The main assumption behind orthotic treatment of the Perthes disease is to decrease the load applied on the hip joint during walking and to increase the containment of the femoral head within the acetabulum.15–17
Unfortunately, little evidence exists regarding the gait analysis of the participants suffering from Perthes disease. The only research in this regard was done by Westhoff et al., 20 who demonstrated that these patients have two different gait patterns in the frontal plane. However, there is no research study regarding the gait performance of patients with LCPD while walking with orthosis. Moreover, it is not clear whether using orthosis reduces the force applied on the hip joint. The aim of this study was, therefore, to evaluate the gait performance of a participant with LCPD while walking with and without an orthosis commonly used to treat this disease. The hypothesis was that the load applied to the hip would be decreased when ambulating while wearing a Scottish-Rite orthosis.
Case Description and Methods
Participant
A single participant with Perthes disease in the left hip participated. He had symptoms of the disease in his left-side hip joint. The participant used Scottish-Rite orthosis for more than 12 months before participation in this study. The severity of Perthes disease was determined based on the classification system developed by the Pediatrics Orthopedic Society, which was classified according to the criteria of Stulberg et al. and Mose, based on the latest follow-up X-ray classifications.9,10,21 In Mose’s method, the sphericity of the femoral head is measured by means of transparent templates with circles drawn at 2 mm intervals.18,21 If the bone outline is a circle or deviates from a circle less than 2 mm on both anteroposterior and lateral roentgenograms, the result is rated as good. If the deviation from a circle is 2 mm on either X-rays, the result is rated as fair. A poor result shows a deviation of more than 2 mm. 21 Based on the above-mentioned method, the scope of severity of LCPD of the participant was scored as fair. His age, height, and mass were 8 years, 1.35 m, and 35 kg, respectively. An ethical approval was obtained from Isfahan University of Medical Sciences, ethical committee. The participant and his parents were asked to sign a consent form before data collection.
Parameters
The spatiotemporal gait parameters, hip joint flexion/extension, abduction/adduction, external and internal rotation, the moments (flexion/extension, abduction/adduction, and internal/external rotation) transmitted through the leg joints, and the forces (axial, anteroposterior, and mediolateral) applied on the leg while walking with and without orthosis were the main parameters selected in this study.
Orthosis
A Scottish-Rite orthosis was used by the participant in this research study. This orthosis was developed in 1971 at the Scottish Rite hospital for crippled children in Atlanta and is a most popular brace for treatment of LCPD. 17 The brace consists of three main components, which include plastic thigh cuffs, a pelvic band, and a single-axis hip hinge. The brace maintains the hip joint in abducted and external-rotated posture. 17 Due to its extension from the hip joint up to the knee joint, it does not restrict the knee joint’s range of motion (Figure 1).
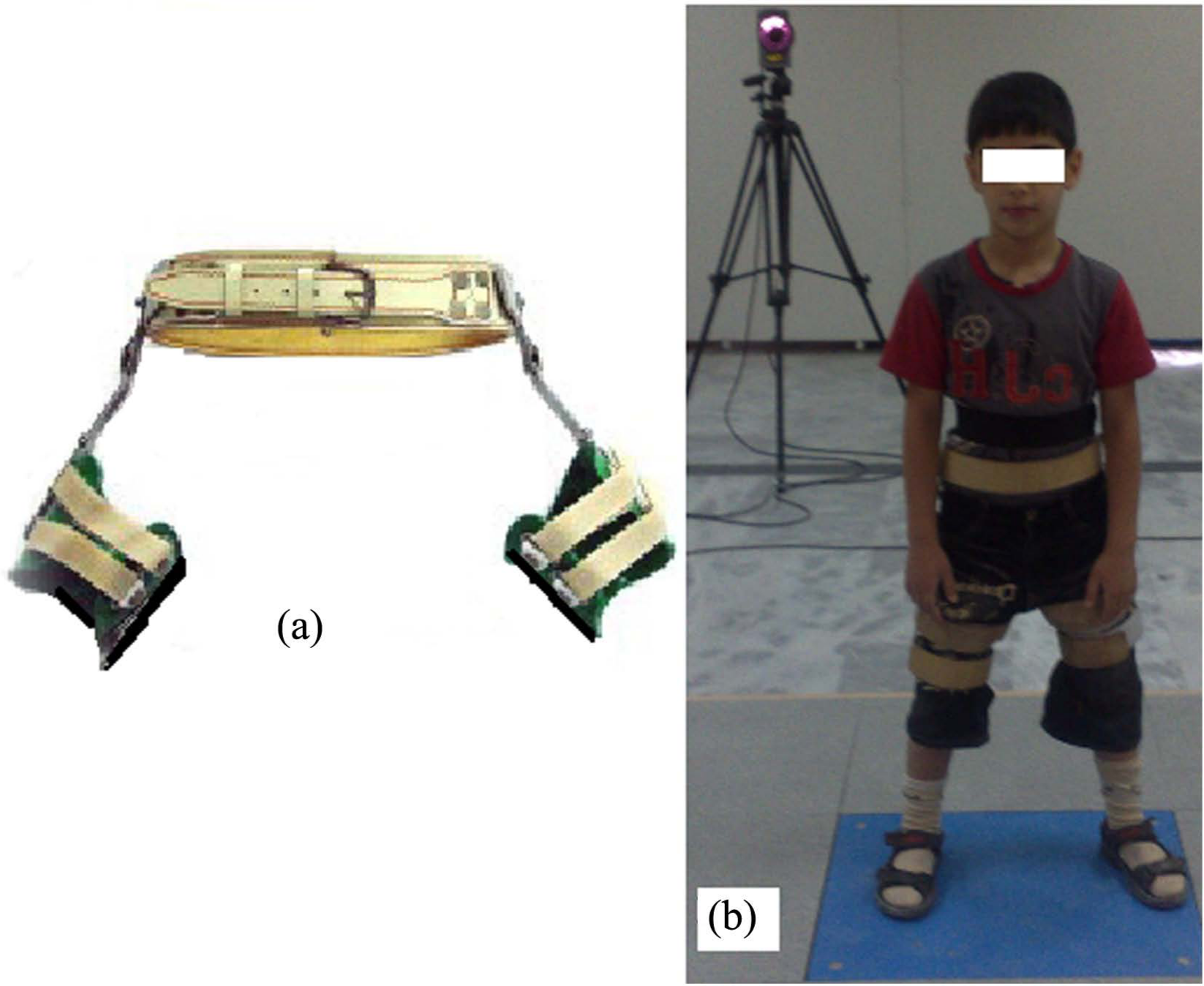
(a) Scottish-Rite orthosis and (b) the patient with Perthes disease in the left hip joint standing with the orthosis.
Procedure
Kinetic and kinematic assessments were performed in the gait lab using seven cameras of a three-dimensional (3D) gait analysis system (Qualisys Motion Analysis System) and a force plate (Kistler). The data were analyzed using visual 3D software, developed by C-Motion, Inc., which allows calculation of the forces and moments of different joints from the collected raw data. The frequency of force plate and cameras was set at 120 Hz.
The participant was asked to walk and stand with and without the orthosis along the gait lab. The markers used in this research were spherical with a diameter of 14 mm covered with a reflective sheet that can be detected by the cameras. The markers were attached on the legs and pelvis according to the preferred method of marker adhesion and subsequent identification used in the Bioengineering Unit of the University of Strathclyde. In total, 16 markers were attached on the right and left anterosuperior iliac spine (ASIS), right and left posterior superior iliac spine (PSIS), medial and lateral malleolus, first and fifth metatarsal heads, and right and left greater trochanter (R-L GT). Moreover, four-markers cluster comprising four markers attached on rhomboid plates were attached on the anterior surface of the legs and thighs using extensible Velcro straps. The participant was asked to walk with a comfortable speed along the gait lab. The tests were repeated 10 times while walking with and without orthosis.
Data analysis
The paired samples t-test with a significant point at 0.05 was used for final analysis. The statistical test was done using SPSS software (version 15).
Findings and Outcomes
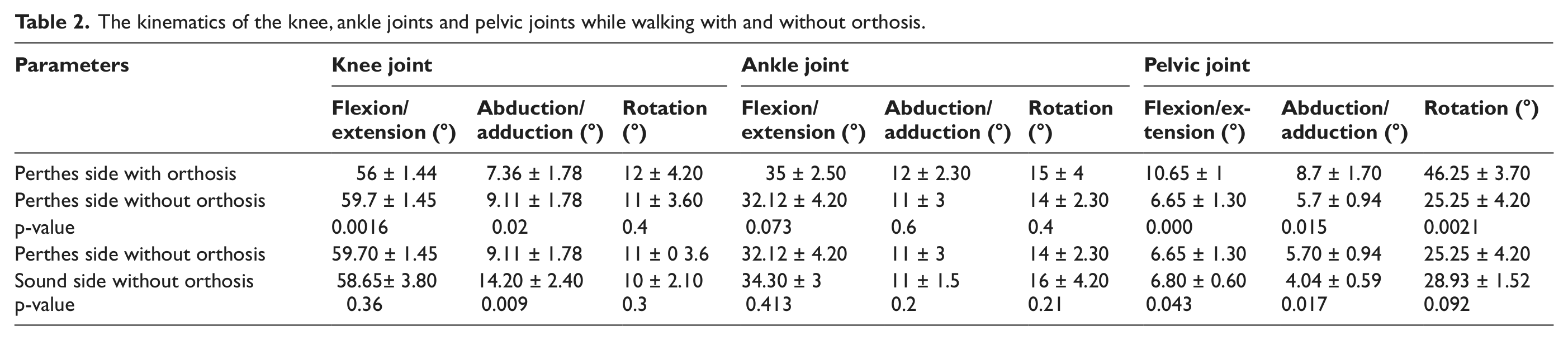
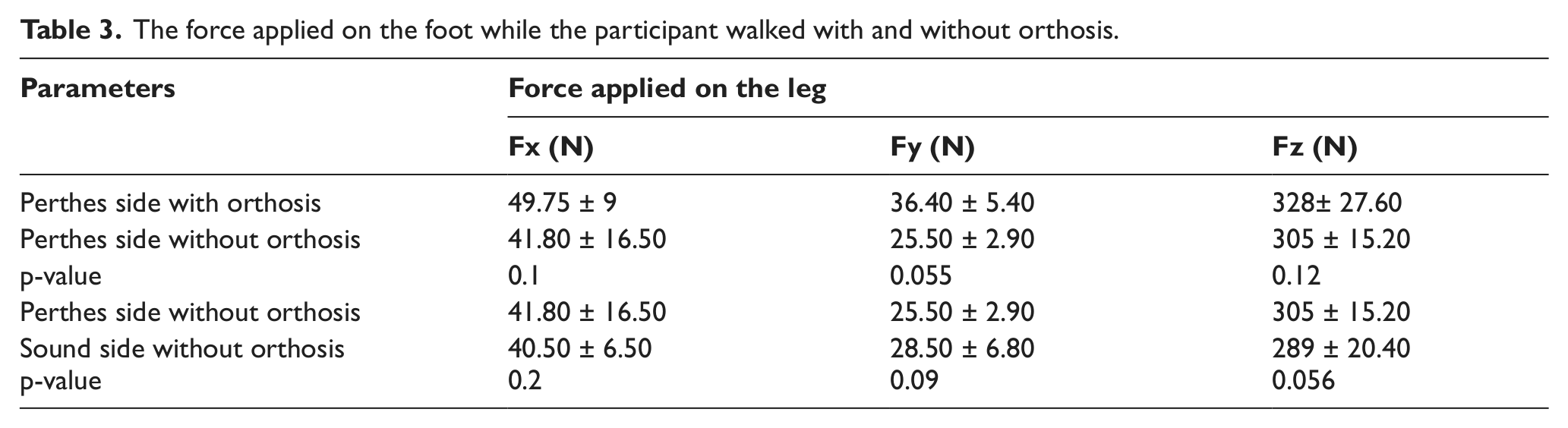
The results of the kinematic parameters of the hip joint while walking with and without orthosis are shown in Table 1. It can be seen from Table 1 that the mean values of flexion/extension excursion of the hip joint was 15.7 ± 2.3° and 39.9 ± 5.3° while walking with and without orthosis (p-value = 0.007). The abduction/adduction excursion of the hip joint was 6.35 ± 1.2° and 9.6 ± 1.3° while walking with and without orthosis, respectively. Moreover, there was no significant difference between the excursion of the hip joint in the sagittal plane in the left and right sides. The abduction/adduction excursion of the hip joint decreased significantly in the effected side (p = 0.0015). The magnitude of the force applied on the leg did not differ significantly while walking with and without orthosis (p > 0.05). However, the difference between the force applied on the hip joint in the left (Perthes side) and sound side differed significantly. The mean value of the left hip joint flexion moment was 8 ± 3.7 and 14.7 ± 2.5 N m while walking with and without orthosis, respectively (p < 0.05). However, there was no difference between the adduction moments in the above-mentioned conditions. Table 2 shows the kinematic pattern of the knee, ankle, and pelvis in three planes while walking with and without orthosis. As can be seen from Table 1, using orthosis influenced the motion of the pelvis in three planes (p < 0.05). The mean values of the force applied on the foot while the participant walked with and without orthosis are shown in Table 3.
The kinetic and kinematic of the hip joint while walking with and without orthosis.
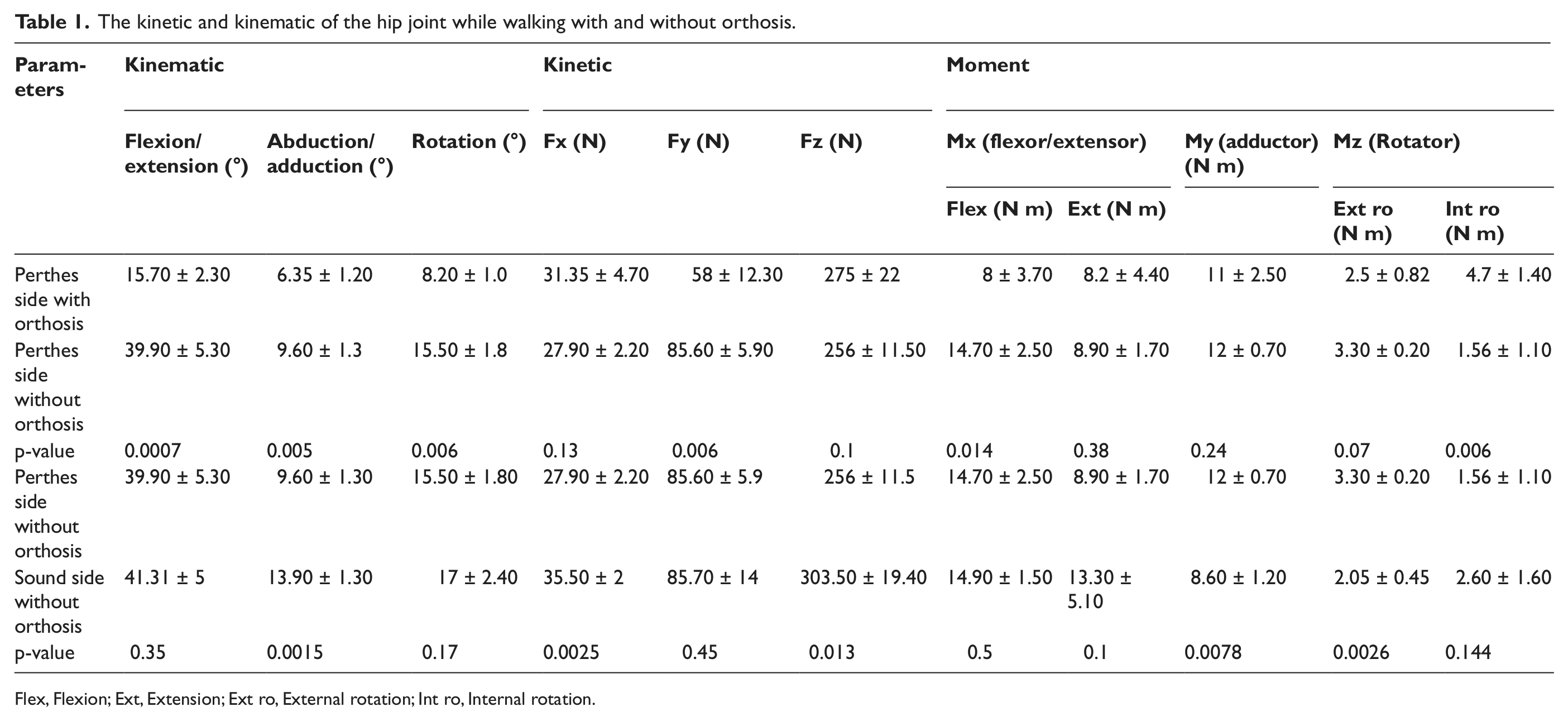
Flex, Flexion; Ext, Extension; Ext ro, External rotation; Int ro, Internal rotation.
The kinematics of the knee, ankle joints and pelvic joints while walking with and without orthosis.
The force applied on the foot while the participant walked with and without orthosis.
The mean value of walking speed with and without orthosis was 57 and 56.6 m/min, respectively, which showed no significant difference. However, cadence increased slightly when the participant walked with orthosis (Table 4). The stride length was 0.99 and 1.08 m in walking with and without orthosis, respectively. Force time integral (FTI) was the other parameter selected in this research study. Based on the results of this research study, the value of FTI parameter was 125.7 N s while walking with and 131.91 N s while walking without orthosis.
The spatiotemporal gait parameter and force time integral of the hip joint resultant force while walking with and without orthosis.
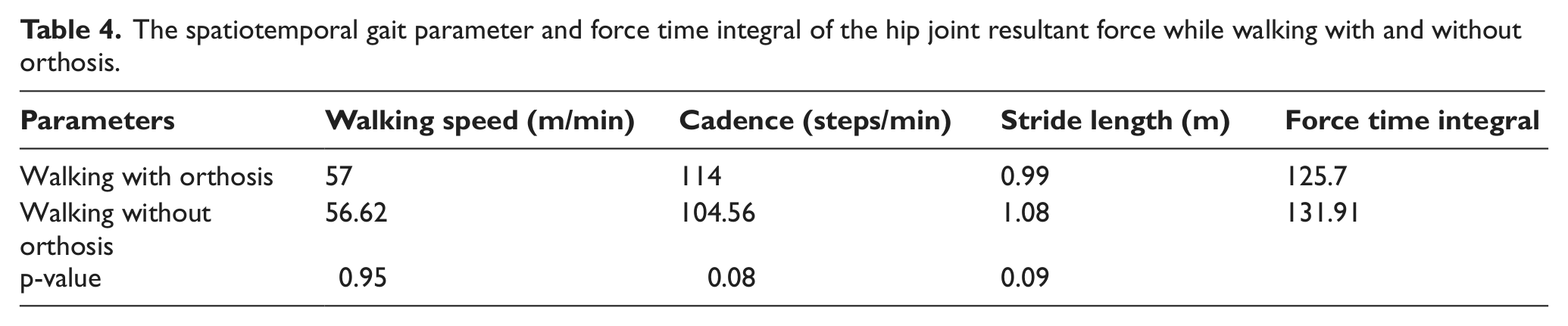
Figure 2 shows the pattern of the left hip joint motions while walking with and without orthosis. Figure 3 represents the motion of the pelvis while walking with and without orthosis.
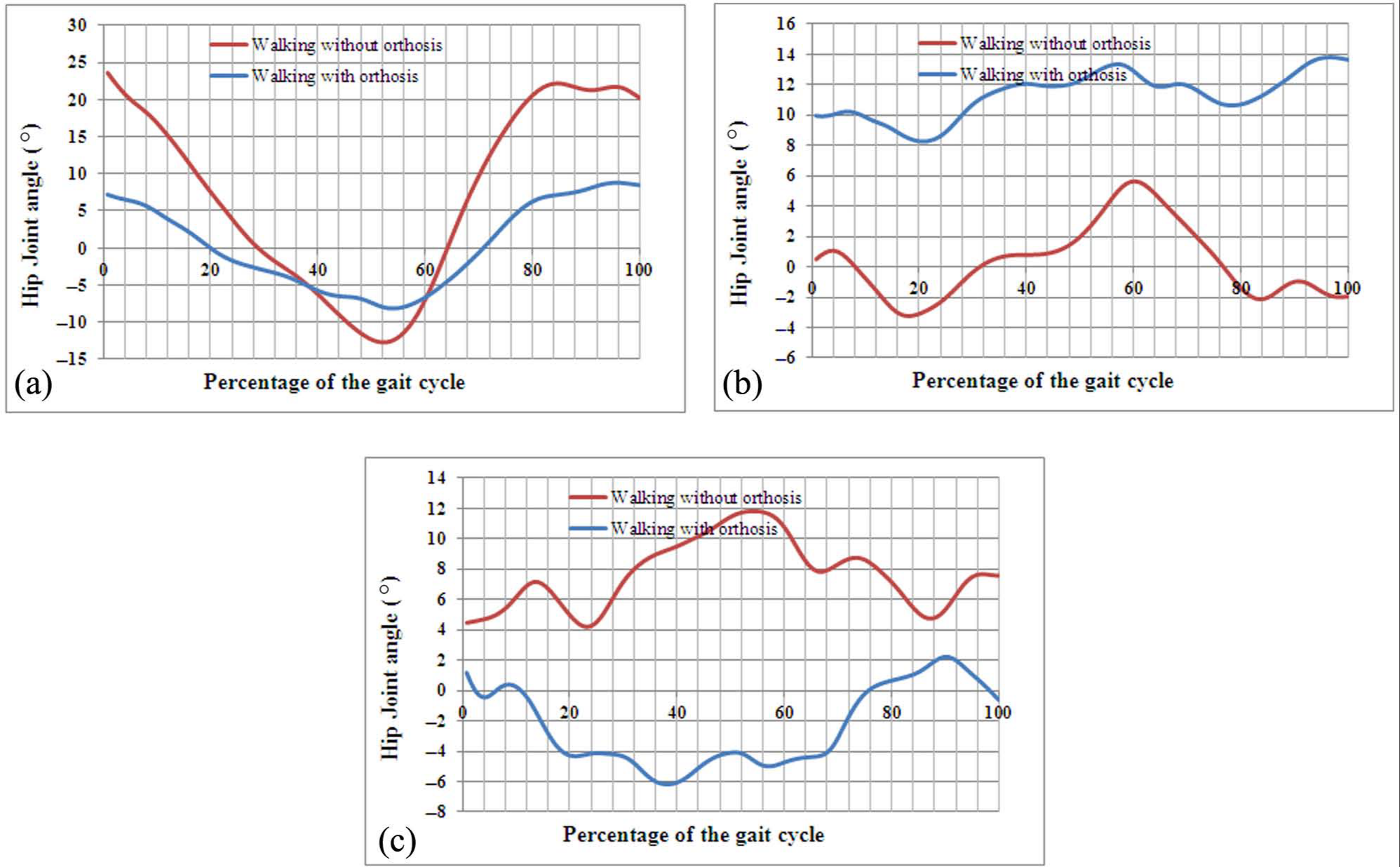
The hip joint motions of the participant while walking with and without orthosis: (a) hip joint flexion/extension, (b) hip joint abduction/adduction, and (c) hip joint external/internal rotation.
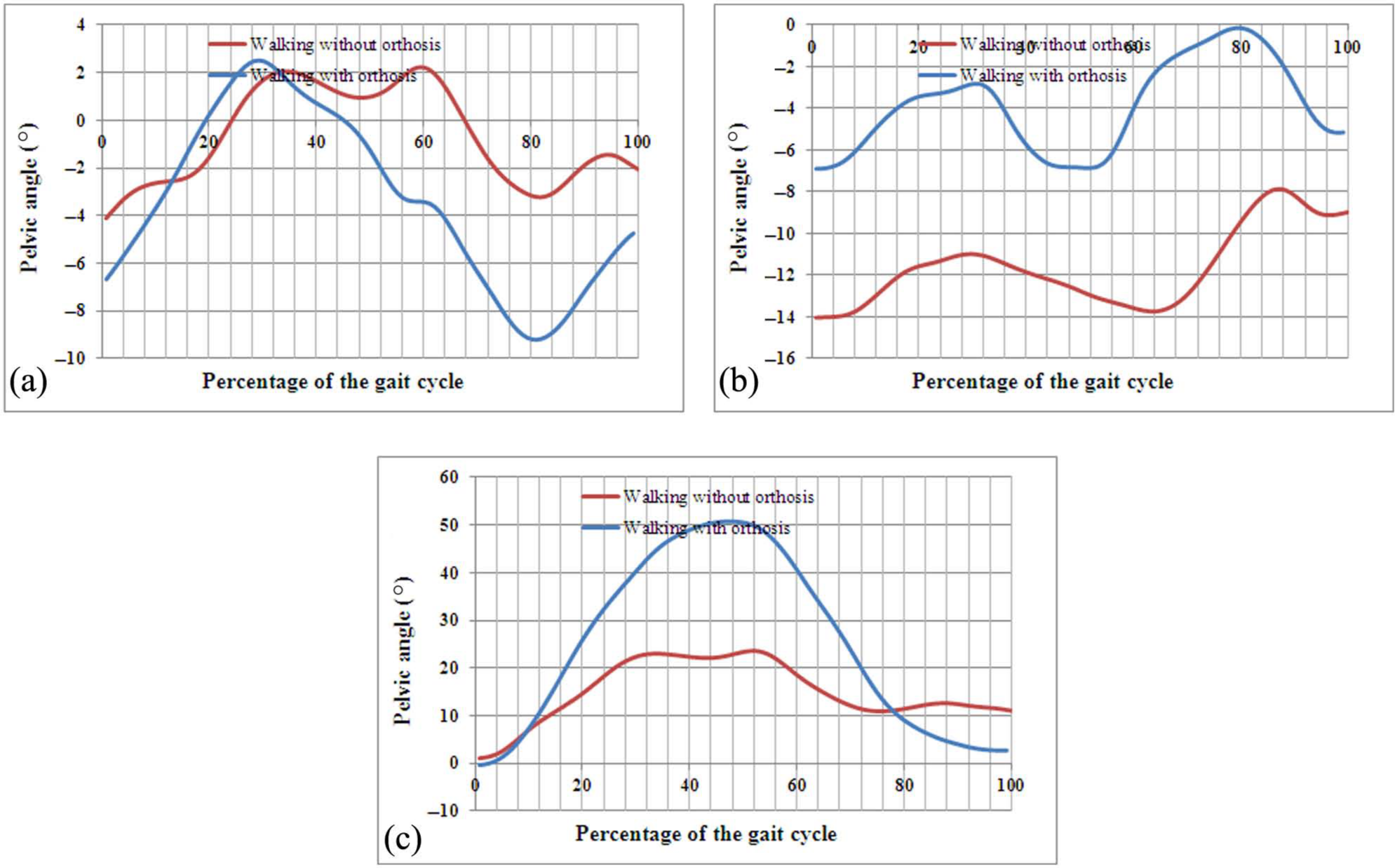
The motions of the pelvis in three planes while walking with and without orthosis: (a) pelvic flexion/extension, (b) pelvic abduction/adduction, and (c) pelvic external/internal rotation.
The main aims of the treatment of LCPD are to prevent the further deformity of the femoral head, relief of symptoms, containment of the femoral head, and restoration of the hip joint range of motion. There are two main approaches regarding treatment of this disease, which include operative and nonoperative treatment approach. Unfortunately, the literature relative to treatment of LCPD is inclusive, and it is difficult to select a standard approach in this regard.7,10 –14
There was no research to represent the influence of using orthosis on the gait performance of participants suffering from LCPD. Therefore, the aim of this research was to analyze the influence of Scottish-Rite orthosis; one of the most commonly used orthosis for Perthes, on the gait performance.
Based on the results of the current research, the kinematic pattern of the hip joint was influenced by the use of Scottish-Rite orthosis (Table 1), due to the restriction provided by the orthosis in the mediolateral and also transverse planes. Although the hip joint flexion/extension range was influenced by use of orthosis, there was no difference between the range of the Perthes and sound sides without orthosis (p > 0.05).
The hip joint range of motion in the coronal plane decreased following Perthes disease by more than 4.3°, Table 1 and Figure 2. In contrast, Westhoff et al. 20 showed that the range of hip joint abduction/adduction increased in this disease.
From Table 2, the kinematics of the knee and ankle joints did not vary significantly between the normal and the affected limb, however, the motion of these joints were influenced by use of the orthosis. The motion of the pelvis was also influenced following the use of the orthosis, the excursions of the pelvis increased in all planes. It represents the importance of close kinematic chain concept while walking with an orthosis. Based on this concept, the restrictions of joint motions influence the patterns and magnitude of motions in other joints.
Although there was no difference between the mean values of the moments applied on the hip joint in the sagittal plane between normal and affected sides, using orthosis decreased the flexion moment of the hip joint, due to restricted hip joint motion in the sagittal plane following the use of orthosis (Table 1). It was expected that the hip joint abduction/adduction would be decreased significantly when the participant walked with the orthosis; however, it increased significantly by use of orthosis. In contrast, it was reported by Westhoff et al. that the hip joint mediolateral moment decreased in this disease compared to normal participants.
The magnitude of the anteroposterior and vertical forces applied on the hip joint decreased in the effected side in contrast to that in normal side (Table 4). Moreover, using orthosis only decreased the mediolateral force applied on the limb. The main reason is the angulations of the hip joint in the mediolateral direction, which was influenced by the orthosis; the orthosis was aligned at 25° of abduction. FTI, which represents the magnitude of force applied on the hip joint with respect to time, was the other parameter selected in this research. Based on the results, the mean value of FTI in walking with and without orthosis was 125.7 and 131.9 N s, respectively. Therefore, the use of orthosis did not influence the force applied on the limb with respect to time.
Although it was expected that walking speed, stride length and, cadence decreased significantly following the use of orthosis, there was no difference between the aforementioned parameters in walking with orthosis. Moreover, the FTI of the resultant force applied on the hip joint did not decrease significantly by orthosis.
There are some limitations associated with this study, which include the following:
This research was done only on one participant.
The stress developed in the hip joint was not measured in this study.
Therefore, it is recommended that the same research be done on a bigger number of participants.
Conclusion
Based on the results of this research, the use of Scottish-Rite orthosis did not decrease the force applied on the hip joint and also the force with respect to time. Moreover, the kinematics of the hip and knee joints was influenced by the orthosis. Although it was expected that the orthosis aligned the hip joint in some degrees of abduction and external rotation, the angle of the hip joint abduction decreased during walking.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.