
Abstract
Background: Existing techniques of taking foot impressions for producing foot orthoses are static, while walking is a dynamic process.
Objectives: The aim of the study was to evaluate a newly developed dynamic casting method for foot orthoses in comparison with static casts.
Study Design: Double-blind, randomized two-period cross-over trial.
Methods: Twelve healthy volunteers (six women, six men) were randomly assigned within gender to two groups. The first group wore orthoses made from static casts for two weeks and then orthoses made from dynamic casts for two weeks, and the second group vice versa. The orthoses were worn during work in sports shoes. The outcome measure was coefficient of variation (CV, defined as standard deviation/mean) over seven measurement spots on each foot.
Results: Foot orthoses produced by a dynamic casting system redistributed plantar pressure (reduced CV) more effectively in the first period on both feet. In the second period, carry-over effect and/or treatment wearing off was observed.
Conclusion: The dynamic casting procedure is simple, low-cost and appears promising, but further research is needed to introduce it into clinical practice.
Clinical relevance
The novel dynamic casting procedure for foot orthoses, which is simple and low-cost, is at least as effective in redistributing plantar pressure as traditional static casting.
Background
Foot orthoses, i.e. insoles, are devices that are confined to the foot only. 1 They are commonly prescribed for treatment of various foot/ankle pathologies, such as diabetes mellitus,2,3 rheumatoid arthritis,4-11 hallux valgus, 12 flat feet,13,14 pes cavus, 4 plantar fasciitis,15-20 and following foot and ankle injuries.21-23 There have been several randomized controlled trials and review articles published about their effectiveness in people with many different pathologies. In most, individually made foot orthoses more effectively improve functioning and/or decrease pain than sham orthoses, but it is not clear which type is the most appropriate due to a wide array of casting techniques, materials used, corrections made and other factors.1-23
There are several types of foot orthoses. According to the way of manufacturing, they can be off-the-shelf (prefabricated) or custom made; according to the design, they can be full-length or short (whereby they can be cut at different places – under the sulcus of the toes or just proximal to the metatarsal heads). According to their primary purpose, they can be corrective, supportive or accommodative. According to the materials used, they are rigid, semi-rigid or soft. Impression-taking techniques for custom-made foot orthoses also vary. The three main ways are by plaster of Paris, by foam impression block or by scanning the plantar surface of the foot. When taking the impression by plaster of Paris, one may use either the slipper cast technique or the circumferential wrap (where it is more difficult to correct the position of the calcaneus). However, all these techniques are static, while walking is a dynamic process and the shape of feet changes during walking.
The aim of this study was to evaluate a newly developed dynamic casting method for foot orthoses by finding out whether foot orthoses made from dynamic casts distribute plantar pressure more equally than those made from static casts. Hence, the main statistical null hypothesis tested was that the effect of both types of orthoses upon plantar pressure distribution is equal.
Methods
Subjects
The study was performed in spring 2011 in the authors’ institution. Twelve healthy volunteers with no foot deformities and no previous history of lower limb injuries, foot problems or pain, six women and six men, were randomly assigned within gender to two groups, so that two gender-balanced experimental groups of six people were formed. Within each group, the subjects were consecutively assigned to groups based on a computer-generated randomization list. No sample size calculation was performed because of the preliminary nature of the study and because no information was available on what effect size in the main outcome measure (within-subject coefficient of variation (CV) of plantar pressure between measurement spots – see below for details) we could expect.
Casting
For static casting, Pedilen foam (Otto Bock, Germany) was used. Subjects seated on a chair with knee flexed at 90 degrees and femur in the neutral position (rotation, ab/adduction). The heel was impressed first, followed by the mid and front part of the foot (Figure 1).
Static casts in Pedilen foam.
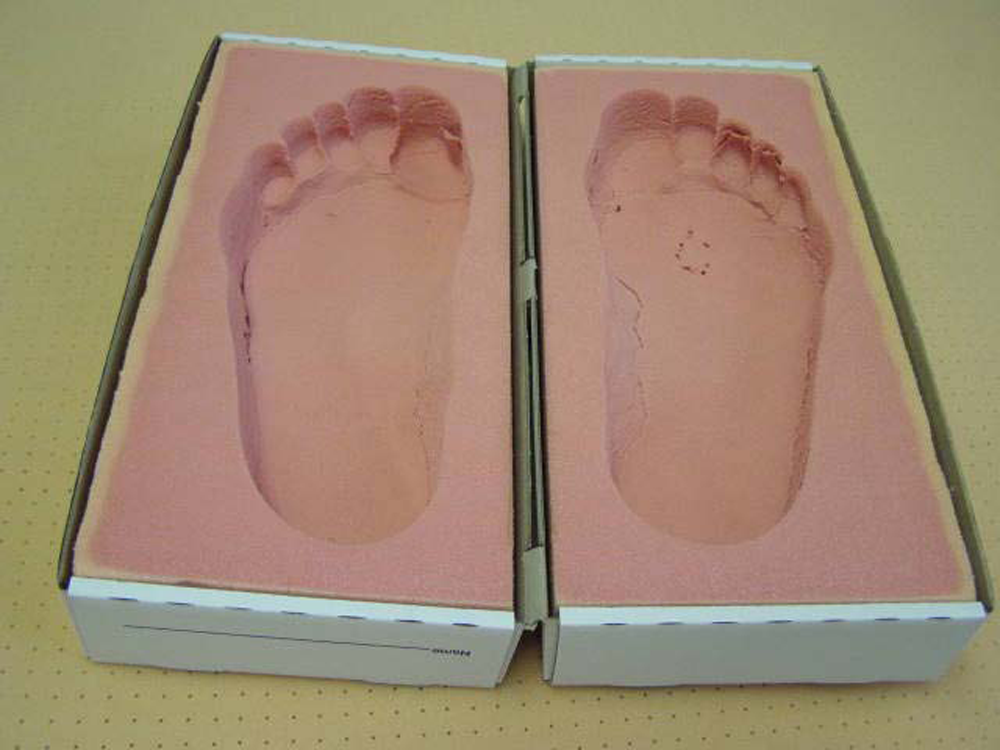
For dynamic casting, special shoes were made in two sizes (Figure 2). They had room for a 10-mm layer of plasticine. Hardness of the plasticine was chosen on the basis of an unpublished pilot study by the same authors, in which subjects walked using plasticine of three different hardness and the one with which impressions of medium depth were obtained was found to be the most appropriate. Subjects walked with the special shoes for 10 metres, so that the dynamic foot impression was obtained (Figure 3). Plasticine was then put into a model for foot orthoses and filled with plaster of Paris to get the model.

Shoes for dynamic casting.

Dynamic impression after walking.
Cast rectification and production of foot orthoses
All casts were minimally modified in the area of transversal and longitudinal arch by the same orthotist. All foot orthoses were made from the same material: 2 mm of viola on top, 6 mm of polyphorm beneath it, and 5 mm of thermo cork at the bottom. In the area of the longitudinal arch, 10 mm of thermo cork was added. Layers were glued together and vacuumed on the model.
Research protocol and outcome measurement
The study was designed as a two-group two-period cross-over experiment with a single baseline measurement. 24 At the beginning, each subject received a pair of sports shoes and plantar pressures were measured in the shoes without foot orthoses. All the subjects were used to regularly wearing sports shoes. Half of the subjects (group A) then received foot orthoses made from the static casts, and the other half (group B) received orthoses made from dynamic casts. Neither the subjects nor the study authors (who performed the measurements) knew who received which type of orthosis. The subjects had to wear the sports shoes with orthoses for two weeks at work (approximately eight hours per day); they were allowed to also wear them in their spare time if they wanted to. After two weeks (i.e. at the end of the first study period), plantar pressures were measured and, after measurement, the groups were switched: group A received foot orthoses made from dynamic casts and group B from static casts. They wore them for two further weeks and after the end of the second study period, plantar pressures were measured again. In addition to the plantar pressure measurements, feet were checked for abrasions, blisters or wounds after the first and the second period.
Plantar pressure measurements were performed using the F-Scan system (version 5.0, Tekscan Inc., Boston, MA, 2001) according to the manufacturer’s standard protocol. The system uses an insole constructed from a matrix of 960 force-sensing resistors (25 mm2 cells) embedded in a very thin Mylar coating. The electrical resistance at each cell is inversely proportional to the pressure applied at its surface. The system allows the measurement of pressure due to vertical component of ground-reaction-force on the foot during walking. Spatial resolution is good enough to identify small features in the foot. The insole is thin (0.18 mm) and unobtrusive in the shoe. Sampling rate (up to 165/s) is adequate for most clinical applications. Since the sensors have been found to lose accuracy with prolonged use, 25 a new pair of sensor insoles was used for each subject. The sensors were cut to fit the shoes and calibrated using body mass as the applied force. All the subjects were given a warm-up period to accommodate to the sensors and to allow temperature equilibration of the sensors since the data are influenced by the temperature of the insole. 26 The recording was performed while the patients walked along an open corridor at their normal walking speed. At least five left and right steps were recorded. The system software was used to analyze the average peak pressures on seven predetermined spots of each foot: hallux, metatarsal head (MT) I, MT II, MT III-IV, MT V, midfoot and heel. In accordance with the system manufacturer instructions, the first and the last step were excluded from the analysis and the average peak pressures were computed from the remaining steps. The system has been found to be sufficiently reliable for conducting studies like ours. 27
All the subjects were informed about the study protocol and provided written consent. The study was approved by the local Research Ethics Board.
Statistical analysis
Descriptive statistics were first calculated for all the studied variables and their distributions and relationships presented graphically. Plantar pressures were analyzed as within- subject CV (i.e. the standard deviation divided by the mean) between measurement spots for each foot. The CV is a suitable measure of effectiveness of plantar pressures redistribution, 10 whereby a lower CV indicates plantar pressure more equally distributed across the joints.
Firstly, comparability of the groups in terms of two possible confounding variables was statistically tested. Since initial graphical examination of the data (Figure 4) indicated a clear carry-over effect, it was warranted to formally test its significance (using difference in mean over periods 1 and 2 between the two groups as a suitable test statistic)28,29 and consequently analyse the data as a parallel-group study (i.e. consider only the first study period). Hence, the difference in mean CV between groups at the end of period 1 when adjusted for baseline value was tested using analysis of covariance (one-way ANCOVA with period 1 mean as dependent variable, group as between-subjects factor and baseline value as covariate). In addition, mean and median ratios of CV at the end of period 1 to baseline were estimated with corresponding confidence intervals. Further justification of the statistical analyses is given in the Discussion. Statistical analyses were performed using SPSS software (version 15.0 for Windows, SPSS Inc., Chicago, IL, 2007).
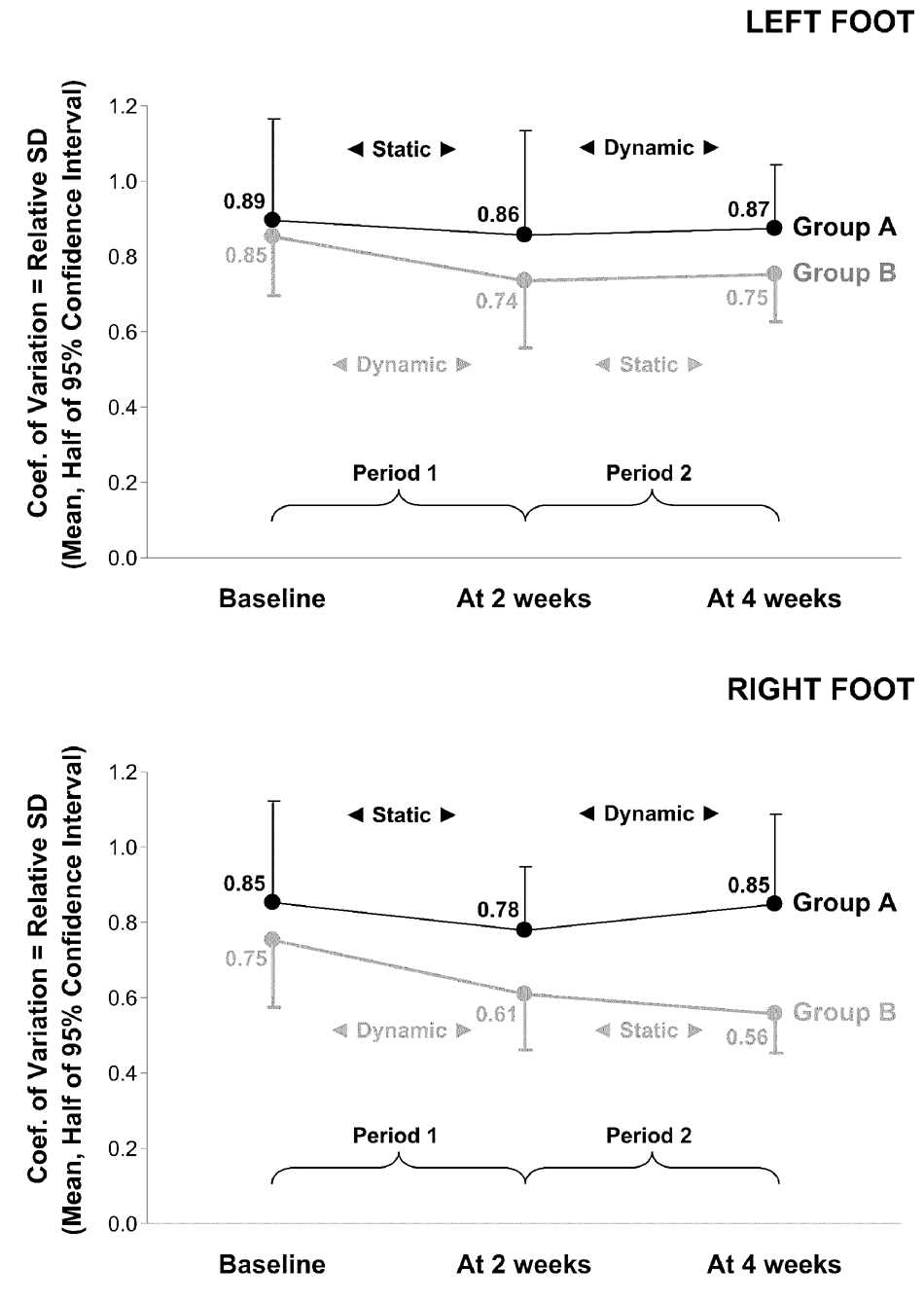
Mean observed coefficient of variation values (with the width of the estimated 95% confidence intervals) at the three measurement time-points.
Results
The groups were confirmed to be comparable regarding the two key anthropometric characteristics that could have influenced the result – weight (group A: mean 77.0 kg, SD 16.7; group B: mean 88.1 kg, SD 25.7; t = -0.892; df = 10; p = 0. 393) and height (group A: mean 1.76 m, SD 0.08; group B: mean 1.75 m, SD 0.09; t = 0.240; df = 10; p = 0.815).
Neither foot orthosis did any skin damage (abrasions, blisters, wounds). The mean observed CV values (with the width of the estimated 95% confidence intervals) at the three measurement time-points are presented in Figure 4. It is clear that during the first study period both types of foot orthoses redistributed plantar pressure more evenly (i.e. reduced the CV), in which the orthoses from dynamic casts appeared to be more effective than those from static casts. This is also indicated (though not formally correctly statistically tested) by comparison of baseline and period 1 means within each group using paired t-test, which indicated a reduction possibly due to chance in group A (i.e. for orthoses from static casts; p = 0.284 and p = 0.418 for right and left foot, respectively) and a reduction highly unlikely due to chance in group B (i.e. for orthoses from dynamic casts; p = 0.048 and p = 0.017 for right and left foot, respectively).
The situation in the second period was less clear. A statistically significant carry-over effect was found on the right foot (t = 2.725; df = 10; p = 0.021), and a notable effect was also observed on the left foot (t = 1.286; df = 10; p = 0.227). As already stressed in the Methods section, further statistical analyses were therefore conducted using the first two measurements only, i.e. the CV at baseline and at the end of the first period.
The groups did not differ significantly in the mean CV at the end of period 1 when adjusted for baseline value (using one-way ANCOVA) either on the right foot (F = 3.308; df = 1, 9; p = 0.102) or on the left foot (F = 1.835; df = 1, 9; p = 0.209), although there was a clear trend towards lower values in group B (i.e. for orthoses made from dynamic casts).
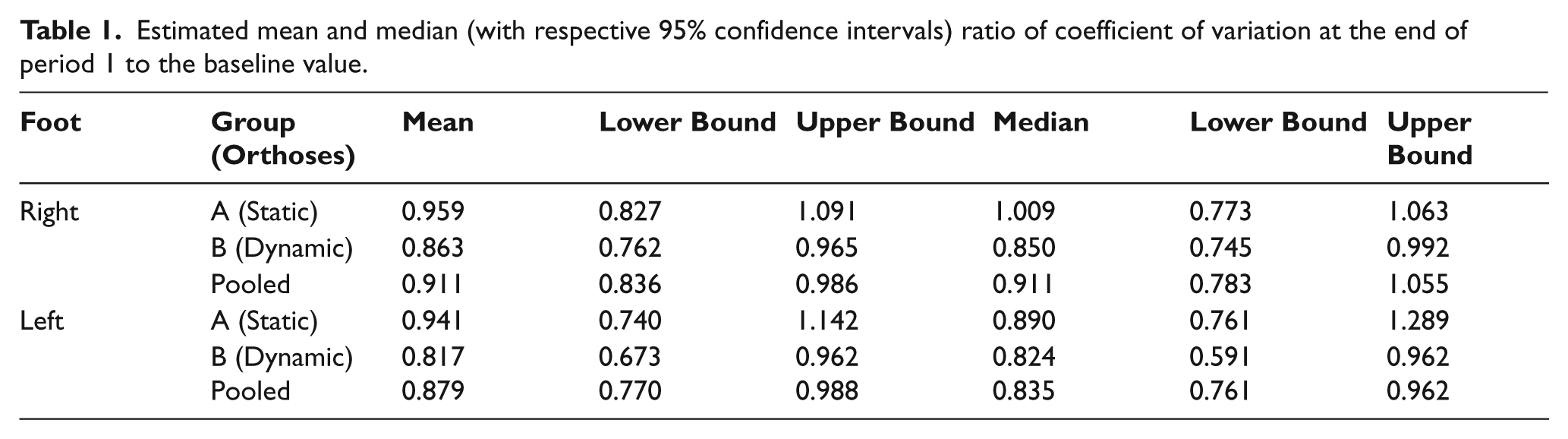
Another view of the effects of the two types of foot orthoses is provided by the estimated ratios of CV at the end of period 1 to baseline (Table 1). On both feet, the mean and median ratios were lower for orthoses from dynamic casts than for orthoses from static casts, whereby the corresponding confidence intervals excluded 1 (thus proving reduction from baseline with high confidence) for orthoses from dynamic casts and included 1 (thus not proving reduction from baseline with high confidence) for orthoses from static casts. Mean and median CV ratio and their corresponding confidence intervals for the pooled sample were below 1 on both feet, thus proving that in general, the distribution of plantar pressure at the end of period 1 was more equal than at baseline.
Estimated mean and median (with respective 95% confidence intervals) ratio of coefficient of variation at the end of period 1 to the baseline value.
Discussion
Foot orthoses are frequently used in subjects with different foot problems to correct deformity, decrease pain and improve function. When foot deformities are flexible and we want to correct them, the preferred way is to make a cast of plaster of Paris, where subsequent corrections can be performed by hand. 1 It is also the most effective and easiest way to correct the heel position. When deformities are fixed and we want only to accommodate them and unload areas with high pressures, other casting methods are used. To decrease pain, it is necessary that the areas with high foot pressure are unloaded. This load is redistributed to the areas which are not loaded at all or where foot pressure is smaller – the goal is to redistribute pressure more equally over the entire foot.
We found out that this redistribution was better with foot orthoses made from dynamic measurement than with those made from static measurements. No other differences were found between the two types of orthoses since none of the orthoses had any side effects, such as skin abrasion, blisters or wounds. In a previous study, 30 it was also found out that subjects were equally satisfied with both types of orthoses and were able to walk equal distances.
Regarding statistical analyses, it should first be emphasized that tachyphilaxis, 31 i.e. the treatment effect wearing off over time, cannot be statistically separated from a carry-over effect in the two-period two-group cross-over trial design that we used. In addition, such particular form of the general problem of period-by-treatment interaction can also affect a parallel-group study, 24 and there are other arguments of contemporary biostatistics against tests and adjustments for carry-over in cross-over trials. 24 Nevertheless, the simple graphical overview of the data sufficed for convincing us to take the so-called two-step approach,24,28 thus preferring fewer and simpler conclusions to statistical optimality that would require additional assumptions. A similar issue was encountered when testing comparability of the groups regarding weight and height as possible confounding variables. Namely, comparability was tested despite the randomized design though such practice is a matter of ongoing statistical debate. 32 In this case, our decision was based on the limited sample size, which made blocking as a possible prevention measure unfeasible, and justified by focusing on only two variables, which are also both known to be related to the outcome measure. In all statistical analyses, reliability of our conclusions was supported by the fact that alternative approaches to those reported (e.g. testing a between-group difference non- parametrically using exact Wilcoxon test instead of parametrically using t-test, or adjusting for baseline by analysing difference scores instead of by analysis of covariance) led to essentially equivalent conclusions.
From the practical standpoint, the key fact is that dynamic measurement is quick, easy and low-cost. It is not necessary to maintain an exact body position, so the measurement can be performed even by non-skilled staff. The same pair of special shoes can be used for all subjects. Plasticine can be reshaped and used several times, whereas foam can be used for one subject only.
The main difference between dynamic measurement and impression in foam is that with impression in foam, it is possible to perform a slight heel correction, while with dynamic measurement it is not. However, no other correction can be made during measurement with either method. Corrections can only be done subsequently by rectification of casts, but none were done in our study because the subjects did not need them. If they had been required, they would have been done in the same way within both methods. Nevertheless, additional studies on patients who have various heel impairments are needed to find out whether the studied problem is sensitive to the correction of the heel.
To summarize, our principal finding is that foot orthoses produced by a dynamic casting system appear to have redistributed plantar pressure in healthy subjects at least as effectively as the orthoses produced by conventional static casting, and at least in the same short term. It will be necessary to check whether the same holds for patients, although there is no reason for a difference if one just wants to accommodate deformities. The only difference in patients may be that deformed feet may behave differently than healthy ones, but there are no studies so far on this topic. Additionally, if the subjects in future studies are not accustomed to daily wearing sports shoes, a learning and accommodation period will have to be incorporated into the study design.
On a final note, it was very surprising for us to observe the carry-over effect and/or the effect of the orthoses wearing off. Based on the literature and clinical experience, we could not have anticipated such an effect, so no ‘wash-out period’ 24 was incorporated into the study design. Together with the sample size, this turned out to be the main limitation of our study. The observed data thus opened several questions to be addressed in further studies: how long does the carry-over effect last, can it also be observed in patients, and what are the most effective ways of wearing foot orthoses? At the very least, our study provides useful data for designing those studies.
Conclusion
In the studied healthy subjects, the redistribution of plantar pressures tended to be better with foot orthoses made from dynamic measurement than with those made from static measurements, but the study limitations do not permit a definite conclusion. Hence, dynamic casting is a promising method for producing foot orthoses, but further research on its efficiency in patients is needed.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors report no conflicts of interest.