
Abstract
Background: An ankle foot orthosis (AFO) using an oil damper (AFO-OD) to assist the first rocker during gait was previously developed but the effect on the other rocker functions has not been clarified.
Objectives: The immediate and short-term effects on the gait of stroke patients with the AFO-OD were investigated from the viewpoint of the rocker function.
Study Design: Crossover study.
Methods: The gait of eight stroke patients in chronic phase without an AFO, with the AFO-OD, and the gait with AFO-OD after three weeks of continuous use and gait training were measured by 3D motion analysis.
Results: Immediate changes observed on use of the AFO-OD were improvements in walking speed, the spatiotemporal parameters, and the angular change of dorsiflexion of the ankle joint. Three weeks of continuous AFO-OD use and gait training showed further improvements in walking speed and the spatiotemporal parameters as well as an increase in dorsiflexion angle and plantar flexor moment of the ankle joint of the paretic limb in stance.
Conclusions: These changes produced improvement of the second rocker function, but improvement of the third rocker was insufficient. Results show the importance of gait training to take full advantage of an AFO.
Clinical relevance
An AFO using an oil damper (AFO-OD) to assist the first rocker function during gait improves the gait of stroke patients. The immediate effects were improvements in walking speed, the spatiotemporal parameters, and the angular change of ankle joint. Three weeks of continuous use and gait training with AFO-OD shows further increase of walking speed and improvement of the second rocker function, such as increase of dorsiflexion and plantar flexor moment of the paretic limb in stance. These findings show the importance of understanding the gait of stroke patients from the viewpoint of rocker function and they also show the importance of gait training to take full advantage of an AFO.
Background
The gait of stroke patients is characterized by decreased walking speed, and significant correlations between self-selected walking speed and clinical parameters have been reported. 1 Gait analysis studies of stroke patients have shown that the anterior-posterior ground reaction force of the paretic limb is highly correlated with walking speed. 2 The intensive medial gastrocnemius and soleus muscle activities in stance of the paretic limb are also correlated positively with anterior ground reaction force impulse. 3 In addition the isokinetic torque of the ankle plantar flexors is highly correlated with walking speed. 4 Furthermore, a significant reduction in mechanical work of the paretic ankle joint at push-off has been reported.5,6 These findings suggest that reduced activity of the plantar flexors is likely to be one of the main causes of decreased walking speed in stroke patients.
Ankle foot orthoses (AFOs) are often prescribed to improve the gait of stroke patients. All AFOs inhibit plantar flexion, but the amount of dorsiflexion allowed depends on the type of AFO used. The commonly used posterior leaf spring (PLS) AFO generates resistance when it is deformed into dorsiflexion. 7 The PLS is thought to absorb energy in the second rocker and return it during the third rocker, 8 but the amount of resistive moment to dorsiflexion is minimal. 9 Solid plastic AFOs generate resistance to dorsiflexion in order to assist the activity of the plantar flexors during gait. From the viewpoint of rocker function, the activity of the plantar flexors makes the second and third rocker functions possible. However, Mulroy et al. showed restriction of dorsiflexion movement during the second rocker in the gait of stroke patients with minimal contracture of the plantar flexors when they walked with solid AFOs. 10 A previous study examining the gait of children with cerebral palsy found that while the first and the second rockers were improved by a dynamic AFO, the third rocker was actually impeded by it. 11 Several studies have shown the importance of the tuning of AFO-footwear combinations using the shank to vertical angle (SVA) to optimize the gait of children with cerebral palsy and stroke patients.12,13 Tuning improves the alignment of the shank and thigh during gait mainly in the second and the third rocker functions. Using a specially designed carbon fibre spring AFO, Desloovere et al. have shown improvement of all three rocker functions in the gait of children with cerebral palsy. 14 It appears then that improvement of the rocker function through the use of an AFO can improve gait. However, to date, only a limited number of studies have examined the effects of AFO use, from the viewpoint of rocker function, on improving the gait of stroke patients.
On the basis of gait analysis results for stroke patients, an AFO equipped with an oil damper (AFO-OD) was designed specifically to assist the first rocker during gait.15,16 Gait improvement has been reported in stroke patients using the AFO-OD, 17 but the mechanism by which it changed the rocker function was not clear. The first aim of the present study was to ascertain the effects of the AFO-OD on the rocker function in the gait of stroke patients by using 3D motion analysis. As is well known, the gait of stroke patients using AFOs alters gradually and the period of use of the AFOs must be considered when studying their effects on gait. Previous studies which showed the effect of AFOs measured gait after several weeks of AFO use but they did not examine gait changes.10,14 Therefore, the second aim of this study was to clarify the short-term effect of the use of the AFO-OD.
The hypotheses of this study were that the AFO-OD, which assists the first rocker function, would improve the other rocker functions during gait in stroke patients, and that the short-term use of the AFO-OD would alter the gait of patients.
Methods
Features of the AFO-OD
In normal gait there are three rocker functions in stance phase. 18 In the first rocker, the body moves forward over the supporting foot with the pivotal axis as the heel, in the second rocker as the ankle joint, and in the third rocker as the forefoot. An AFO-OD (GaitSolution Design, Kawamura Gishi) which was developed to assist rocker functions was used in this study. It is an AFO with a mechanical ankle joint that is equipped with an oil damper (Figure 1). The oil damper set in the ankle joint generates a resistive moment when the ankle joint moves to plantar flexion. To tune its use to the needs of individual patient, the magnitude of the resistive moment can be changed easily by rotating a screw at the top of the oil damper. The initial angle of the ankle joint can also be changed to adjust the ankle joint angle in which the resistive moment starts to generate. The resistive moment assists insufficient eccentric contraction of the dorsiflexors, making first rocker function possible during loading response of the paretic limb (Figure 2). Since the ankle joint of the AFO-OD moves freely to 30 degrees in dorsiflexion, the AFO-OD does not itself assist the activity of the plantar flexors (Figure 2). The oil damper generates the resistive moment to plantar flexion in the third rocker to prevent excessive plantar flexioin. The foot part of the AFO-OD has no contouring and has a shorter length to allow general shoes to be worn with it.
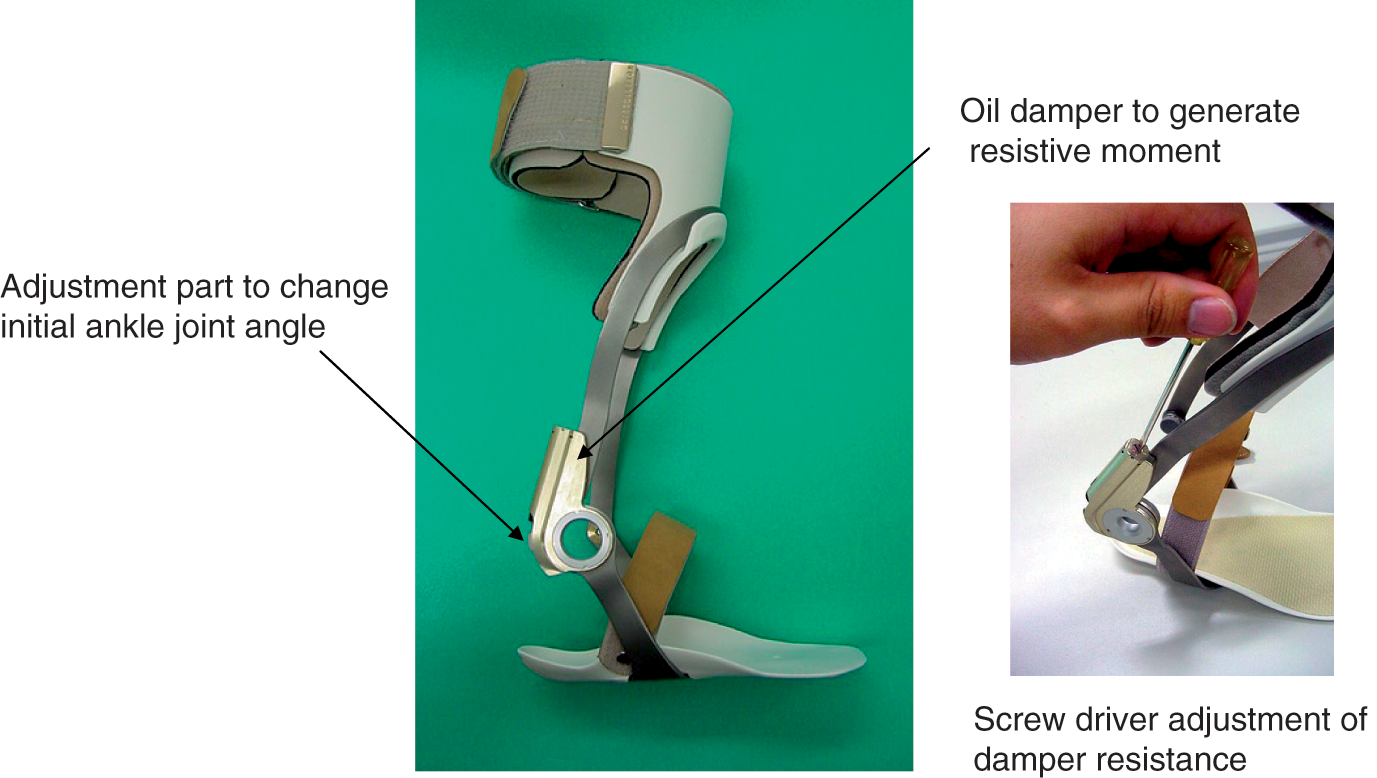
Structure of the ankle foot orthosis using an oil damper.
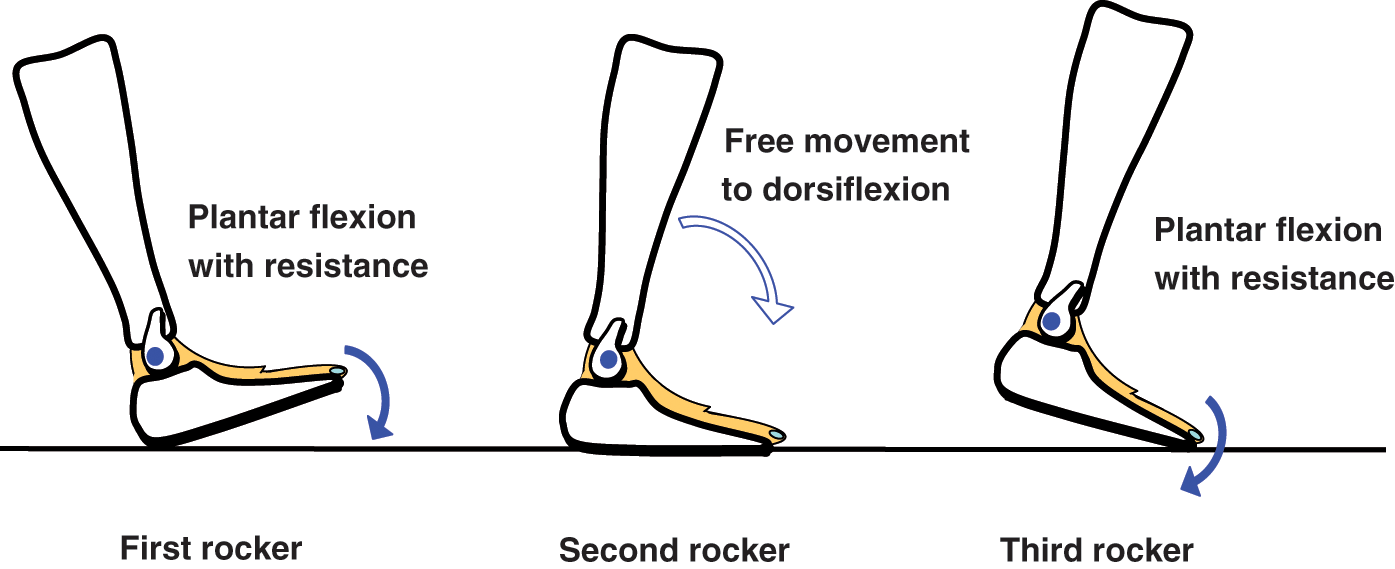
Schematic function of the ankle foot orthosis using an oil damper (AFO-OD) during gait. The AFO-OD generates resistive moment to plantar flexion to assist first and third rocker functions, but the ankle joint moves freely to dorsiflexion in the second rocker.
Patients
Ten stroke patients in chronic phase (more than 181 days after onset) participated in this study. Patients in chronic phase were selected because of the steady state of their gait, based on the fact that the recovery curve of stroke patients rises to plateau at around six months post-onset. 19 Other inclusion and exclusion criteria were decided according to previous results of a questionnaire survey concerning monitoring of AFO-OD use among 99 stroke patients. 20 In that study, clinical and gait parameters which affected the adaptation of the AFO-OD were investigated. The inclusion criteria were use of an AFO daily or recommended use of an AFO in daily living, and first heel loading of the paretic limb during gait with any types of AFO. Present use of an AFO and the type of AFO used were not of concern here because they did not affect the adaptation of the AFO-OD. The exclusion criteria were non-concurrent pathologies affecting the central nervous system (CNS) or neuromuscular system, communication problems, severe spasticity and proprioceptive sensory impairment. All 10 patients participated between one and three times per week in a general rehabilitation program run by physiotherapists. Walking speed was almost constant, as determined on the 10 -m walk test.
After the first session of the study protocol described below, two patients dropped out. The reasons were severe inversion which could not be controlled by the AFO-OD in one patient, and toe dragging at initial swing which could not be improved by the AFO-OD in the other patient. The profiles of the remaining eight patients who participated in the entire study are shown in Table 1.
Patient profiles
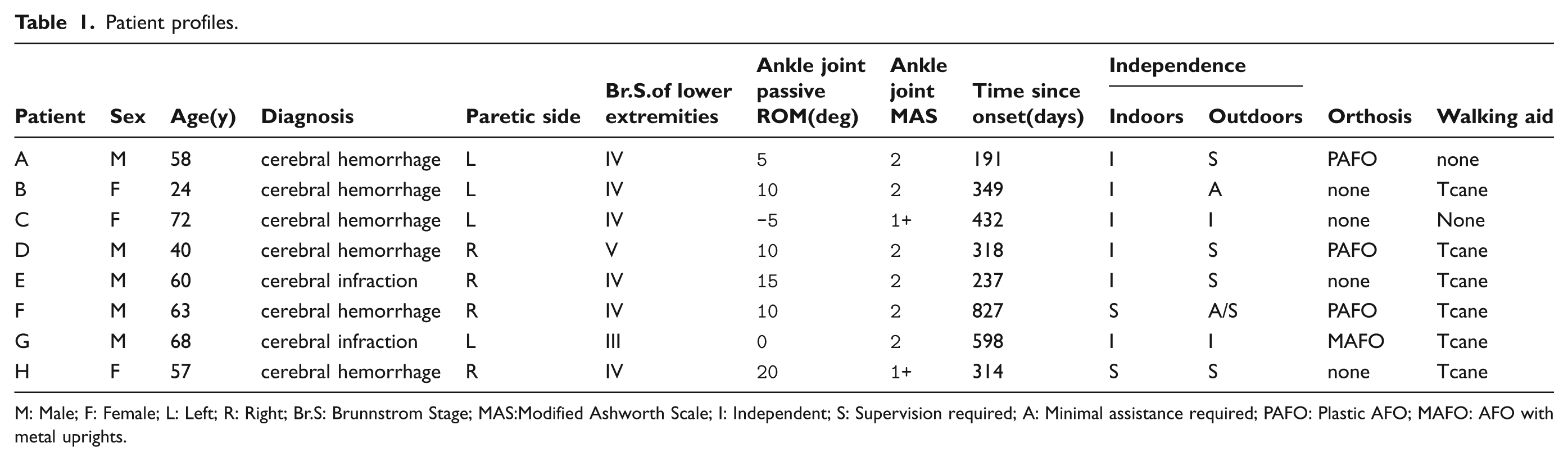
M: Male; F: Female; L: Left; R: Right; Br.S: Brunnstrom Stage; MAS:Modified Ashworth Scale; I: Independent; S: Supervision required; A: Minimal assistance required; PAFO: Plastic AFO; MAFO: AFO with metal uprights.
All procedures were approved by the local ethics committee of Seiai Rehabilitation Hospital and were consistent with the Declaration of Helsinki. Informed consent was obtained from all patients prior to their participation in the study.
Study protocol
Gait was measured using a 3D motion analysis system (10 VICON Mx cameras and six AMTI force plates). Six force plates were arranged in three rows of two. The patient stepped onto the right-hand plates with the right foot and onto the left-hand plates with the left foot. A total of 16 reflective markers were attached to the following landmarks of the patients: bilaterally on the acromion process, trochanter, and posterior aspects of the iliac spine, elbow, wrist, lateral epicondyle of the knee, lateral malleolus, and fifth MP joint. The trajectories of the markers and the force plate data were measured at a sampling frequency of 100 Hz. Patients wore their own shoes in all measurements and the use of canes was allowed during measurement if necessary. First, gait with shoes but without an AFO was measured at the patient’s selected speed, and measurements were repeated until five steps of affected limb on the force plates were obtained. Then, the patients started using the AFO-OD. After five to 10 minutes practice to acclimate to the AFO-OD, gait with the AFO-OD was measured. Before measurement of gait with the AFO-OD, the magnitude of the resistive moment and the initial ankle joint angle of the AFO-OD were tuned by orthotists to each patient’s condition according to the physiotherapist’s observation and the patient’s opinion. The tuning of the resistive moment was made to achieve smooth foot contact during loading response. The initial joint angle was adjusted so that the resistive moment started to generate from the ankle joint angle at the initial contact.
After the first measurement, the patients were asked whether they wished to use the AFO-OD continuously. If the patient answered affirmatively, they started using the AFO-OD for three weeks. During this three-week period, the patients used the AFO-OD daily and participated in 20-minute gait training sessions while wearing it. The hours in which the AFO-OD was used per day depended on each patient’s condition. The training sessions were run by physiotherapists between one and three times per week. During gait training, the therapists told patients to pay attention to making heel contact with their knee joint extended as much as possible, which ensured first rocker function of the paretic limb. After three weeks, gait with the AFO-OD was measured by the same protocol. Consequently, measurements were carried out for each patient in the following three conditions: without an AFO and with the AFO-OD before and after three weeks of continuous use.
Data processing
The trajectory of markers and the force plate data were low-pass filtered by a second-order Butterworth filter with a cut-off of 6 Hz. 21 The link segment model consisted of 11 segments: the trunk including the head, both of upper arms, forearms, thighs, shanks, and feet. The center of gravity (COG) and the joint centers were calculated using anthropometric data for each segment of the link segment model. The joint kinematics and kinetics were calculated using the inverse dynamic model employed in previous studies21,22 The use of a cane when needed meant that the floor reaction force and the joint moments of the non-paretic limb could not be measured because patients often put the cane on the same force plate as the non-paretic limb. From these data, the spatiotemporal parameters and peak values of joint angles and joint moments of the paretic limb examined in previous studies10,14,23,24 were detected for one gait cycle of each patient in each condition. Step length was normalized by body height, and the joint moment was normalized by body height and body mass. The baseline of the ankle joint angle was defined as when the shank was vertical to the floor. The ankle joint angle from initial contact to peak plantar flexion during loading response was also detected because this value showed how the joint of the AFO-OD moved during the first rocker. A positive joint angle value indicates flexion and dorsiflexion. The joint moment is shown by internal moment as positive extensor and plantar flexor.
Additional parameters were calculated including anterior-posterior floor reaction force and ankle plantar flexor power generation in stance. These parameters were chosen because they are indicators of the propulsive ability of gait in stroke patients.2–6 The floor reaction force and the power were normalized by body mass. In total, 28 gait parameters (left column, Table 2) were used for the analysis.
Mean and standard deviation for gait parameters of the three walking conditions (n = 8), and results of statistical analysis
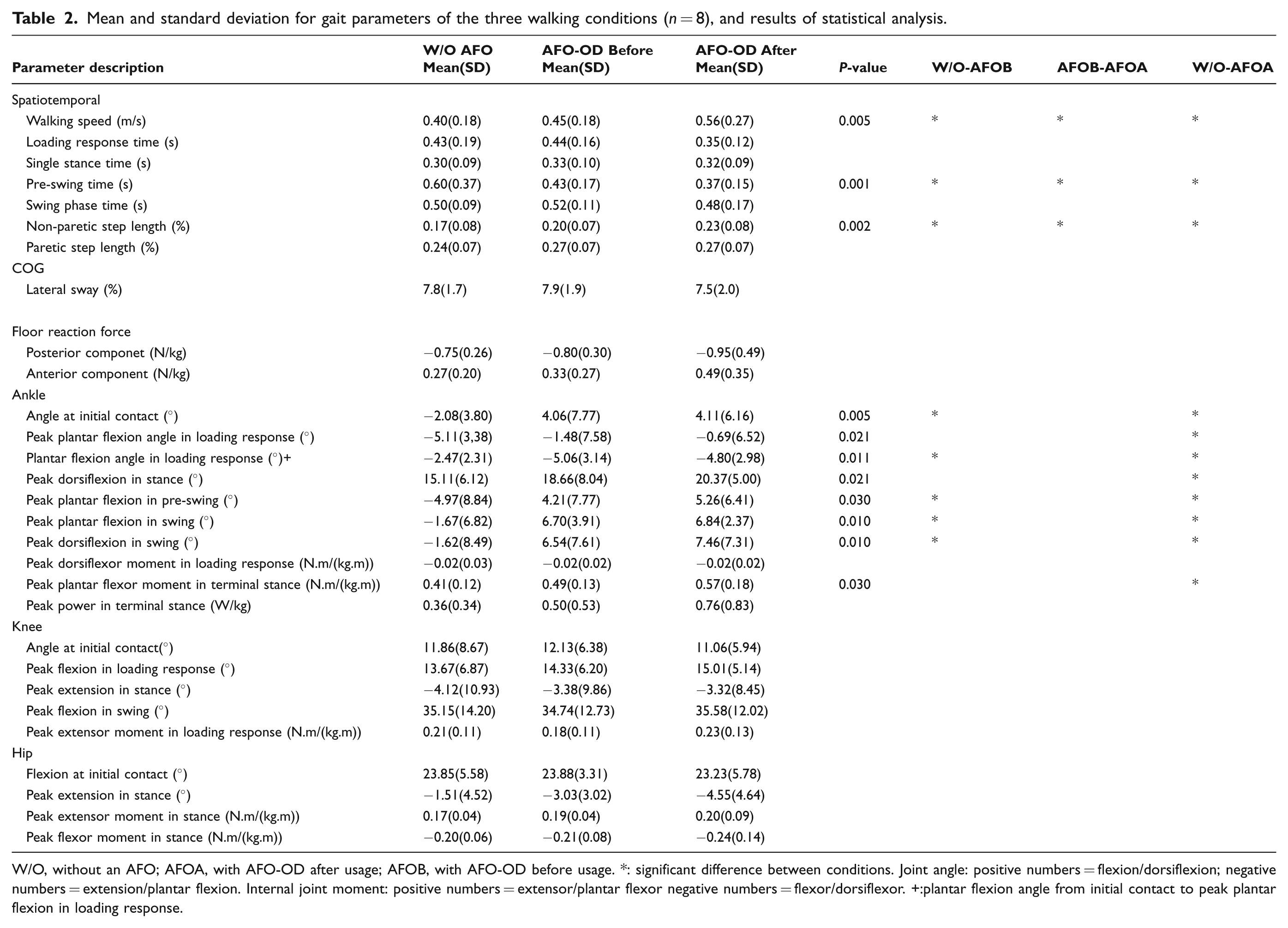
W/O, without an AFO; AFOA, with AFO-OD after usage; AFOB, with AFO-OD before usage. *: significant difference between conditions. Joint angle: positive numbers = flexion/dorsiflexion; negative numbers = extension/plantar flexion. Internal joint moment: positive numbers = extensor/plantar flexor negative numbers = flexor/dorsiflexor. +:plantar flexion angle from initial contact to peak plantar flexion in loading response.
Statistical analysis
The gait parameters were determined and averaged for at least five gait cycles in each of the three experimental conditions. To exclude the effect of outliers in this small test group, non-parametric statistical analyses were performed. First, a Friedman analysis was performed to determine whether there was a significant difference between the three conditions. If a significant difference was found, then further comparisons were made between without an AFO and with the AFO-OD before use, with the AFO-OD before and after continuous use, and without an AFO and with the AFO-OD after continuous use. A Bonferroni correction was applied to reduce the likelihood of obtaining false-positive results. Statistical significance was established at a P-value of 0.05 for the Friedman analysis and it was adjusted by number of comparisons for post-hoc pairwise comparison. SPSS version 15 for Windows was used for all statistical analysis.
Results
As shown in Table 2 results of the Friedman analysis showed significant differences in walking speed, pre-swing time of paretic limb, step length of non-paretic limb, and ankle kinetics and kinematics of paretic limb. Immediate change effected by the AFO-OD was found in an increase of walking speed, decrease in pre-swing time, and increase in non-paretic step length. The ankle joint angle at initial contact, peak plantar flexion in pre-swing, and angles in swing were more dorsiflexed with the use of the AFO-OD.
Three weeks of AFO-OD use and gait training resulted in a further increase in walking speed, decrease of the pre-swing time, increase of non-paretic step length, and improvement of angles around the paretic ankle joint. In addition, regarding the parameters related to second rocker function during gait, the peak dorsiflexion angle in stance changed from 15.11 degrees without an AFO to 20.36 degrees with the AFO-OD after three weeks of use. Peak plantar flexor moment in terminal stance increased from 0.41 N.m/(kg.m) without an AFO to 0.57 N.m/(kg.m) with the AFO-OD after three weeks of use.
As for the parameters related to third rocker function, pre-swing time was significantly decreased and peak plantar flexion angle in pre-swing was significantly decreased by the AFO-OD. The anterior component of floor reaction force and peak power in terminal stance increased in the condition with AFO-OD after three weeks of continuous use but the change was not significant. Joint kinetics and kinematics around the hip and the knee joints showed no significant differences.
The changes in walking speed and the peak plantar flexor moment in the three experimental conditions in the eight stroke patients are shown in Figure 3a and 3b. Patients who showed the increase in walking speed also showed an increase in the peak plantar flexor moment after using the AFO-OD for three weeks.
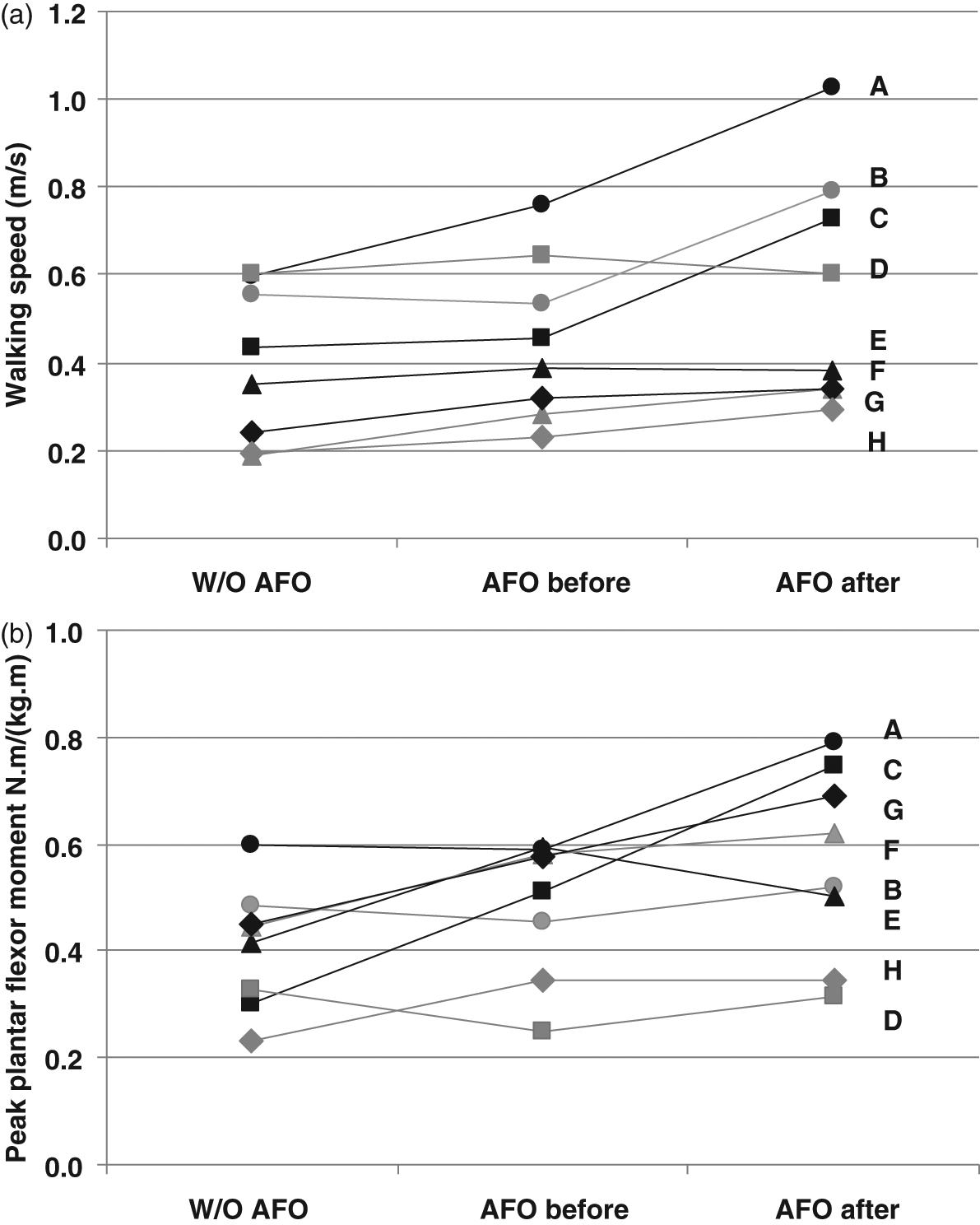
The changes in waking speed a) and the peak plantar flexor moment b) in the three experimental conditions in the eight stroke patients (each patient indicated with a letter).
Discussion
The hypotheses were supported by the results obtained in this study. When comparing the results of gait without an AFO and with the AFO-OD, walking speed, spatiotemporal parameters, and ankle joint kinetics and kinematics of the paretic limb all showed improvement. These results were similar to those of previous studies investigating the effects of using AFOs.10,14,23–27 In the present study, a dorsiflexed ankle joint angle at initial contact and increased plantar flexion angle during loading response were seen with the AFO-OD. This movement, which was assisted by the use of the oil damper in the AFO-OD, resulted in improvement of first rocker function. In this study the increase in walking speed, 0.40±0.18 m/s without an AFO and 0.56±0.27 m/s with AFO-OD after three weeks of continuous use and gait training, was larger than that in previous studies.10,23 In normal gait, the second rocker starts in the plantar flexed position of the ankle joint. Given the results of this study, it is suggested that controlled plantar flexion of the ankle joint during loading response may result in the successive second rocker function and increased gait speed. The amount of resistive moment generated by the AFO-OD was minimal, so it would not directly affect the kinetic changes of the gait of patients. However, it affected the loading condition on the paretic limb and thus caused the kinetic changes in later gait cycle.
At first glance, the function of the AFO-OD seems to be similar to that of the PLS. The PLS provides resistance to plantar flexion and its resistance to dorsiflexion is minimal. However, with regards to first rocker function, the resistance to plantar flexion of the AFO-OD differs from that of the PLS. At initial contact, the reaction force from the floor is applied to the heel and the force vector goes slightly behind the ankle joint. When patients wear the AFO-OD, the floor reaction force vector runs slightly behind the mechanical ankle joints, enabling plantar flexion but also generating resistive moment. It is similar to the function of the ankle joint and the eccentric contraction of the dorsiflexors in normal gait. The PLS does not have a mechanical joint and its center of deformation is slightly behind the malleolus. When patients wear the PLS, the floor reaction force is applied to the heel but the force vector is dissipated around the center of deformation. The floor reaction force does not deform the PLS to plantar flexion directly. The PLS starts to deform after the patient’s sole pushes the foot part of the PLS downward. Since the first rocker occurs in a very short period, the difference in timing of the deformation between the AFO-OD and the PLS is marked. Therefore, the difference in structure between the AFO-OD and the PLS is not negligible.
Previous studies have shown dynamic knee instability due to an increased external flexion moment during loading response when patients walked with excessive plantar flexion resistance produced by traditional AFOs with a plantar flexion stop.10,23,28 This phenomenon manifested as an increase in the internal knee extensor moment during loading response. In the present study, no difference was found in the knee joint moment because the knee joint was prevented from moving forward excessively due to the gradual plantar flexion supported by the oil damper.
The short-term effect of the AFO-OD resulted in a significant increase in the plantar flexor moment, which showed a relationship with walking speed in each patient, as shown in Figure 3. The plantar flexor moment relates to the forward progression of the center of pressure and it gradually increases during the second rocker in normal gait. Thus, the peak value of the plantar flexor moment indicates the performance of second rocker function. Parvataneni et al. showed an increase in walking speed after a muscle strengthening training program in stroke patients. 29 The significant increase in walking speed and plantar flexion seen in the present study are similar to Parvataneni et al.’s results. With use of the AFO-OD, the ankle joint moved freely to dorsiflexion, indicating that the AFO-OD provided no assistance to the plantar flexors. The increase in the plantar flexor moment did not involve assistance from the AFO-OD itself. Most patients in this study used a cane during measurement and therefore the effect of using a cane may not be negligible. The increase in the plantar flexor moment implies the possibility of a change in muscle activity when using the AFO-OD, and this possibility should be explored in further study involving electromyographic analysis.
The present results showed that the AFO-OD improved first and second rocker functions in the gait of stroke patients. However, the change in the anterior component of the floor reaction force and peak ankle plantar flexor power generation in pre-swing were not significant, indicating that improvement of third rocker function was insufficient even after continuous use of the AFO-OD. As the peak ankle plantar flexion power is larger than 2.0 (W/kg) in normal gait, 30 the value obtained in this study 0.76 (W/kg) is still smaller than it.
There were a number of limitations to this study. Only the paretic limb was evaluated and only the kinetics and kinematics in the sagittal plane were examined. Muscle activity was not measured. The small sample size recruited from a hospital may mean a lack of generalizability of the results of this study. Further investigation will be necessary with a larger and more diverse patient population.
Conclusion
Although the AFO-OD was designed to assist first rocker function during gait, the effects of its use on gait from the viewpoint of rocker function were unknown prior to this study. The gait changes resulting from immediate and three weeks of continuous use of the AFO-OD were investigated by 3D motion analysis. The immediate changes observed were improvements in walking speed, pre-swing time, step length of the non-paretic limb, and the angular change of dorsiflexion around the paretic ankle joint at initial contact and during swing phase. Three weeks of continuous use and gait training with AFO-OD run by physiotherapists resulted in further improvement in walking speed and the spatiotemporal parameters as well as an increase in the peak dorsiflexion angle and the peak plantar flexor moment of the paretic limb in stance. These changes indicate improvement of the second rocker but not third rocker function, with the latter remaining insufficient. These results showed the importance of gait training to take full advantage of an AFO.
Footnotes
Acknowledgements
The authors thank Mr A Hagiwara of Yokohama Stroke & Brain Center for valuable advice regarding the screening of patients. The AFO-OD was kindly provided by Pacific Supply Co., Ltd., and orthotists of Kawamura-Gishi Co., Ltd. manufactured and adjusted the AFO-OD to fit each patient. The authors thank therapists at Seiai Rehabilitation Hospital for providing gait training using the AFO-OD and the patients who participated in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.