
Abstract
Theraplay® is a relationship-focused intervention based upon attachment theory that involves both adult and child. There is a growing evidence base for Theraplay® as an intervention with children and families although empirical research on its use with adoptive families is currently in its infancy. This research provides an understanding of the reasons for choosing Theraplay® as a support for adoptive families and how the intervention was implemented within a Regional Adoption Agency (RAA) and explores the views of adoptive parents and professionals regarding its effectiveness. The research design was a multiple case study with embedded units of analysis. Semi-structured interviews were used with adoptive parents, and three focus groups were held with professionals to collect qualitative data. The data were analysed thematically resulting in the emergence of four main themes: support, process of intervention, impact of intervention and meeting the needs of adoptive parents. These themes are discussed in relation to existing literature, implications for practice and future research. The limitations of the research are also discussed.
Plain Language Summary
Theraplay® is an intervention that focuses on developing relationships between adults and children and is rooted within attachment theory. Some studies suggest that Theraplay® is an effective intervention in work with children and families, but there is little research into its benefits specifically for adoptive families.
The current study gathered the views of three different adoptive families who attended a Theraplay® informed intervention and the corresponding professionals involved in running these sessions. It focuses on the reasons why Theraplay® was chosen as a support for adoptive families, how it was established and run within one Regional Adoption Agency (RAA) and whether the intervention was seen as beneficial for the three families as well as what improvements could be made.
Participants’ views were gathered through interviews and focus groups and the findings were analysed to look for similar themes to report on. The four main themes generated were: support, process of intervention, impact of intervention and meeting the needs of adoptive parents. These themes are discussed here, linking them to previous research on Theraplay® and future suggestions for how professionals may deliver the intervention. The limitations of the research are also discussed.
Introduction
The National Context For Adoption And Adoption Support In The Uk
Adoption is the legal process by which a child who cannot be brought up by their birth family becomes a full, permanent and legal member of their new family (Adoption UK, 2023). The number of children adopted within the UK in 2022 was 2,950, representing a 2% increase since 2021 (UK Government, 2022).
In 2015, the Department for Education (DfE) published a paper outlining reforms to adoption by proposing a move to Regional Adoption Agencies (RAAs) (DfE, 2015). The hope was that by developing RAAs, the life chances of adoptive children would be enhanced, in part, by improving adoption support. RAAs were encouraged to explore new models of delivery and to be at the forefront of innovative practice. As of August 2020, there are currently 22 such agencies operating in the UK (DfE, 2020).
RAAs have a statutory requirement to provide adoption support, as set out in the Adoption Support Regulations 2005 and the Statutory Guidance for Adoption 2013 (DfE, 2020). These documents stipulate which services should be available for different groups such as the adopted child, adopters and potential adopters, alongside support for the birth families. While the RAA or local authority must complete an assessment of need, it is not a requirement for the local authority to provide any specific support but to advise what services would be beneficial and to ensure they are made available if required. However, the Adoption and Special Guardianship Leadership Board (ASGLB) has commissioned consultative work to develop a blueprint for high-quality adoption support (DfE, 2020).
Adoption support can mean different things to different families and will often vary depending on the age and development of the child. Pennington (2012) suggests that for adoption to be successful, placements need to be backed by high-quality support services, including therapeutic support. Finding appropriate support can be the difference between a thriving child in a secure family environment and the potential breakdown of the adoption order, creating further trauma for both the child and family (Pennington, 2012). Adoption support encompasses a variety of services: opportunities to enable groups of families to come together, therapeutic support, counselling, information and advice, mediation, financial and practical support as well as working in partnership with schools to train other professionals (Stother, Woods and McIntosh, 2019).
Adopted children are suggested to be one of the most vulnerable groups in society (Langton and Boy, 2017). Children who have been placed for adoption are more likely to have experienced abuse and neglect prior to entering the care system (Gore Langton, 2017). The complexity of developmental trauma suggests that most adopted children have been deeply hurt in their early relationships, which affects how they form subsequent relationships (Langton and Boy, 2017). By taking a multidisciplinary therapeutic approach to support, which may include services such as educational psychology, child and adolescent psychotherapy and attachment-focused therapies, children can be supported to build and maintain positive relationships with adoptive parents, and with other people in their lives (Pennington, 2012).
A small-scale research project examining what professionals working in an RAA view as key elements of early post-adoption support was conducted in 2021 (France and McIntosh, 2021). The findings suggested that the professionals viewed Theraplay® informed parent–child dyadic groups as one of the key elements to successful adoption support within the first 12 months of placement.
Theraplay®
Theraplay® is an attachment-based therapeutic intervention with the goal of supporting the development of the relationship between the adult and child through attuned interactions. These adult–child interactions are based upon four core dimensions: structure, engagement, challenge and nurture, with the hopeful outcome being one of strengthened connection. The sessions are intended to be playful and to promote trust and joy between the adult and child (Norris and Lender, 2020). Games and activities are selected by the therapist, session by session, making each one bespoke to the needs of the individual, dyad or group. Challenge activities are used to encourage mastery and competence while allowing the child to take developmentally appropriate risks. Nurture activities enable the adult to show the child that they are worthy of care and are used to promote opportunities for positive touch and co-regulation. The structural dimension is used to help regulate the child’s experience while setting adult-led boundaries. The engagement dimension helps to foster a sense of playfulness and fun while encouraging the child to enjoy themselves (Norris and Lender, 2020). Managing the child’s regulation is much of the focus of a Theraplay® intervention, with the therapist being aware of the child’s arousal state and using activities to keep the child within their window of tolerance (Siegel, 2012). Traditionally, Theraplay® is facilitated dyadically with parent and child; however, more recent empirical research has shown success when it is used as a group intervention (Francis, Bennion and Humrich, 2017; Siu, 2009).
The Evidence Base For Theraplay®
In 2016, the DfE commissioned an evidence review of the efficacy of the most well-used and prominent therapeutic post-adoption support interventions, of which Theraplay® was one (DfE, 2016). The review aimed to better understand the interventions and further examine the scope of evidence on their effectiveness for post-adoption support. The review stated that there was very little empirical evidence of the effectiveness of Theraplay® as an intervention; however, it was found to be one of the 15 most frequently used therapies funded by the Adoption Support Fund (ASF) and judged as high profile within adoption support (DfE, 2016).
A recent scoping review found only 11 published articles within its parameters exploring Theraplay® with children and families, with only one being research based in the UK (France, McIntosh and Woods, 2023). Within the 11 articles in this review, only three had included adoptive families in their research. Purrington and colleagues (2022) found that Theraplay® informed support did produce some positive outcomes for adoptive families. Adoptive parents were more able to handle challenging behaviours displayed by their adoptive children, which helped to develop the relationships between them. The same research also found an improvement in the child’s ability to accept greater levels of nurture, structure, challenge and engagement from their adoptive parents. Weir and colleagues (2013) found that integrating family systems theory and Theraplay® with adoptive families did have some level of clinical efficacy. They identified an overall improvement in the adopted children’s behavioural functioning, and family communication was enhanced. Weir (2008) used parental self-report within his research involving one adoptive family. The findings indicated an improved relationship and demonstrated that when integrated with play therapy, Theraplay® did produce some overall positive outcomes for children with Reactive Attachment Disorder. A systematic literature review conducted in 2020 showed that Theraplay® with children under 12 was promising in its effectiveness, but that more rigorous empirical research was needed to develop an evidence base (Money, Wilde and Dawson, 2020).
Dunsmuir and Hardy (2016) state that educational psychologists (EPs) need to keep up to date with relevant therapeutic interventions and be responsible for adding to the research into their effectiveness. The current study aims to contribute to the research literature relevant to EPs working therapeutically, particularly with adoptive children and families. In the USA, Theraplay® has been rated a promising intervention and has been given evidence-based status by the California Evidence-Based Clearinghouse (Theraplay® Institute, 2021). This research hopes to add to the evidence base for Theraplay® in the UK.
Research Questions
The aim of this study is to explore Theraplay® informed groups as an intervention for adoptive families within one RAA in the North-West of England. It will consider the rationale behind choosing Theraplay® informed group intervention, how it has been implemented, and explore parental and professional views of its effectiveness.
The research addresses the following questions:
Why was a Theraplay® informed intervention chosen to support adoptive families? How have the Theraplay® informed interventions been implemented with adoptive children and families within the RAA? How has attending a Theraplay® informed intervention group supported adopted children and their families?
Methodology
Research Design
The current study utilised a descriptive multiple case study design with embedded units of analysis informed by Yin (2018). This research set out to discover what Schramm (1971: 6) describes as the essence of a case study as a research method, which ‘tries to illuminate a decision or set of decisions: why they were taken, how they were implemented, and with what result’.
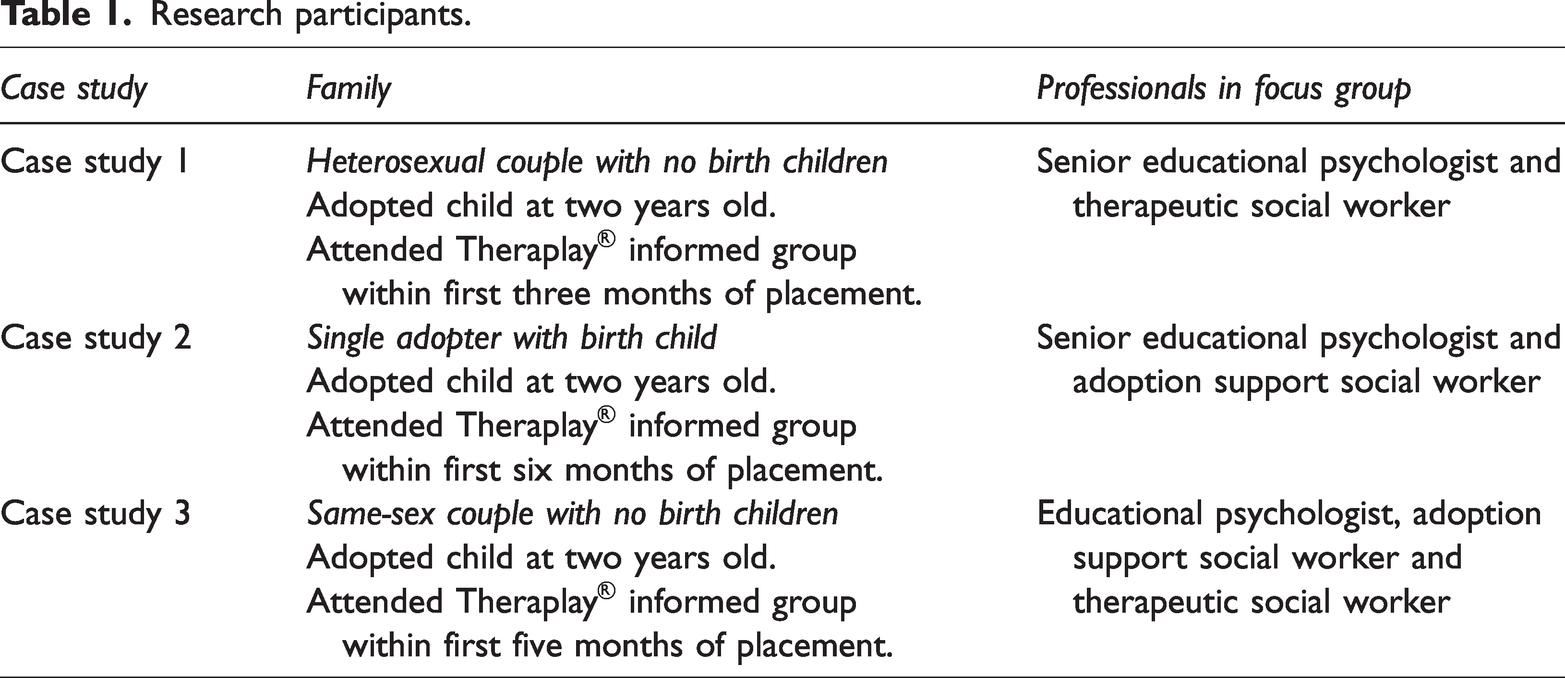
Qualitative data were acquired from three cases to make up the multiple case study, with the aim of developing a more in-depth understanding of the phenomena than a single case could provide (see Figure 1). Yin (2018) maintains that case studies are an advantageous approach when aiming to answer ‘how’ and ‘why’ questions, where the researcher has little control over the phenomena or events being studied and where results are likely to be contextually dependent. Within this research the RAA is the context for the case studies. Further information about the three cases included can be found in Table 1.
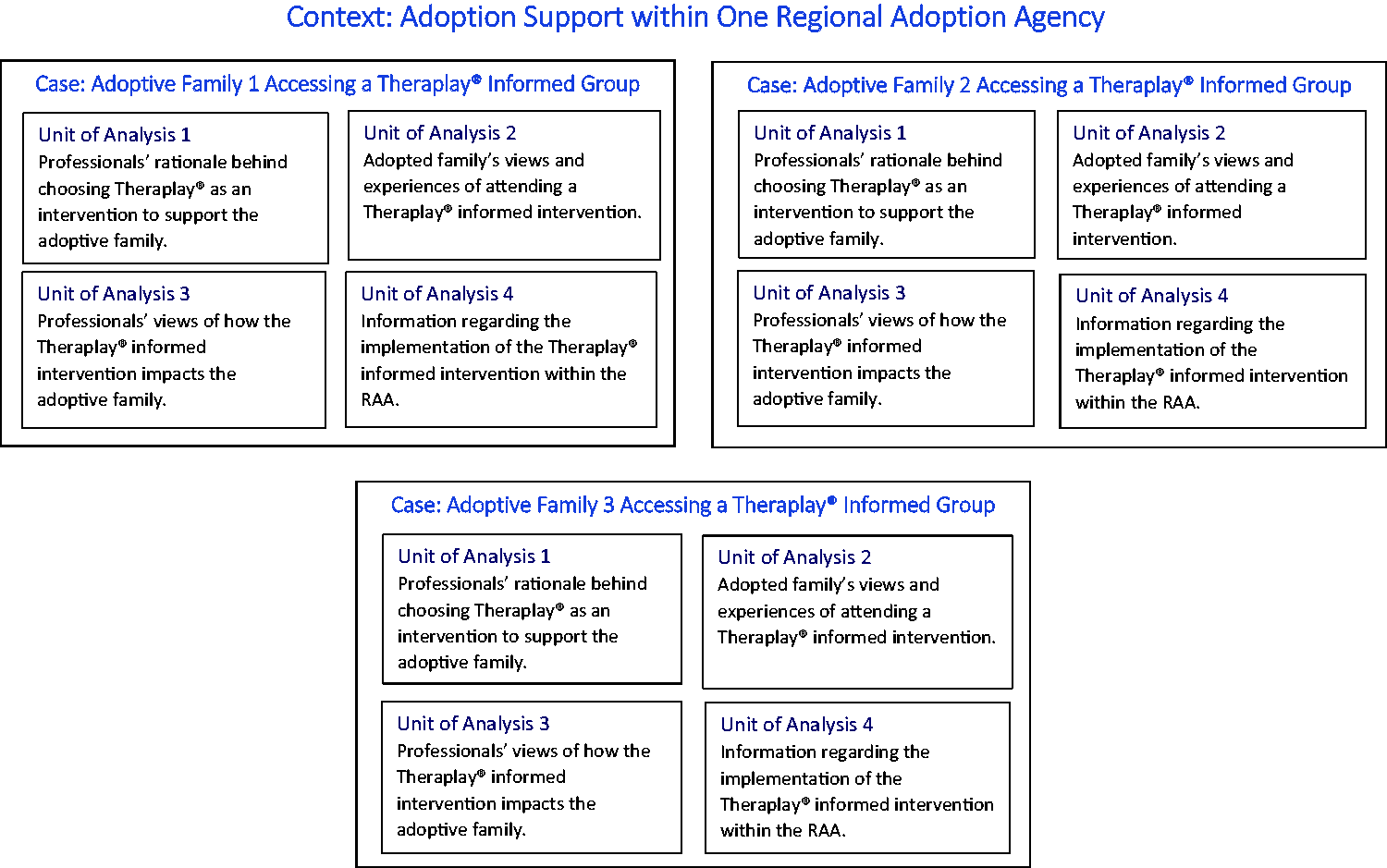
Diagram of multiple case study design.
Research participants.
Alternative research designs were considered, including a large-scale survey approach; however, due to the lack of existing research in this field, and therefore little information from which to guide a quantitative exploration on the application of Theraplay® informed interventions for adoptive families, a small-scale qualitative study was deemed most appropriate.
Sampling And Participant Recruitment
A purposive convenience sampling strategy was used to recruit families to participate. Three families were recruited through links with the Adoption Psychology Team. This allowed the lead researcher to establish the homogeneity of the sample to ensure that each research question could be addressed comprehensively in each case. The lead researcher sought to recruit families with contrasting family/placement contexts to enhance the potential transferability of the findings (see Table 1).
The focus groups consisted of professionals in adoption support currently working in the Adoption Psychology Team within the RAA. They included EPs, therapeutic social workers and adoption support social workers. Focus group participants were identified once the families had been recruited and had given consent for the researcher to contact them. At least one of the professionals within each focus group had facilitated the Theraplay® informed group linked to the family. Each of the lead facilitators had completed the Theraplay® Institute accredited Level 1 or 2 and group training as a minimum requirement.
Data Collection Methods
Parental interviews took place after participation in a full course of Theraplay® informed intervention via the RAA; this group intervention comprised four online sessions for adopters only and six face-to-face dyadic sessions with their child within a larger group. The groups were facilitated by professionals who were trained to at least Level 1 or Level 2 and group Theraplay®, which is accredited by The Theraplay® Institute. The 10 sessions were devised based upon the principles of Theraplay®.
Semi-structured interviews were facilitated online owing to the RAA covering a large geographical area; also, research suggests that participants are more likely to take part when researchers are flexible, adapt to existing commitments and have respect for their participants’ time (Brueton et al., 2013). Newby (2010) states that semi-structured interviews provide a method which encapsulates participants’ views through open-ended discussions. Semi-structured interviews also allow for additional unplanned questions to be asked and for modification of initial questions depending on the participant’s responses. Each semi-structured interview had a question schedule to ensure that the same questions were asked within each interview, while providing the flexibility to explore additional topics brought up.
Focus groups were used to ascertain professionals’ views on their rationale for choosing Theraplay® informed group interventions, to gain their views on using this method for adoptive families and to understand how it had been implemented within the RAA. Focus groups also took place once the intervention sessions were complete. Focus groups were used as they allow the researcher to gather multiple views from individuals simultaneously. These groups are often chosen in research where time constraints are an issue as they can be an effective and efficient tool to provide rapid responses to research questions (Cyr, 2014). In addition, focus groups are valued because they can stimulate discussion between participants, allowing them to explore views they had not previously considered and to highlight consensus and areas of disagreement (Robson, 2002).
Contextual information was gathered from the RAA. This included a welcome pack for adoptive parents on Theraplay® informed group interventions, alongside some pre- and post-measures from each of the families that highlighted their hopes and goals of attending the group. Only documents that were deemed useful but not sensitive were shared with the researcher. Using documents can provide background information and broad coverage of data and is therefore helpful in contextualising the research (Bowen, 2009).
Method Of Analysis
Semi-structured interview and focus group data were analysed through thematic analysis using the six-step method outlined by Braun and Clarke (2006):
Familiarisation with the data
The researcher read the transcriptions multiple times prior to and during analysis to become familiar with the data and facilitate analysis. Transcripts were checked for accuracy and read in detail several times prior to beginning analysis.
2. Generating initial codes
The researcher used a mixture of hand-coding and NVivo Pro data management software (NVivo qualitative data analysis software; Version 12, 2018) to code the data and look for patterns in responses between parent-participants and professionals. Each case study was coded before comparing themes identified across case studies.
3. Searching for themes
Codes were categorised by hand under themes, and thematic maps were created to organise the data to ensure all relevant information was included within the analysis. An appropriately qualified researcher cross-checked coded sections from the three different case studies and compared them with the researcher’s initial coding, which resulted in a high level of agreement.
4. Reviewing themes
Themes were reviewed initially by the primary researcher. The same additional researcher reviewed the final themes and illustrative quotations, which were systematically selected to ensure a breadth of participants’ views. Member-checking was conducted with the participants from each case study to further support credibility, which highlighted agreement from all participants.
5. Defining and naming themes
Themes were finally renamed and defined more precisely before being checked against the original transcripts to ensure no data had been overlooked. A final thematic map was created and can be seen below (Figure 2).
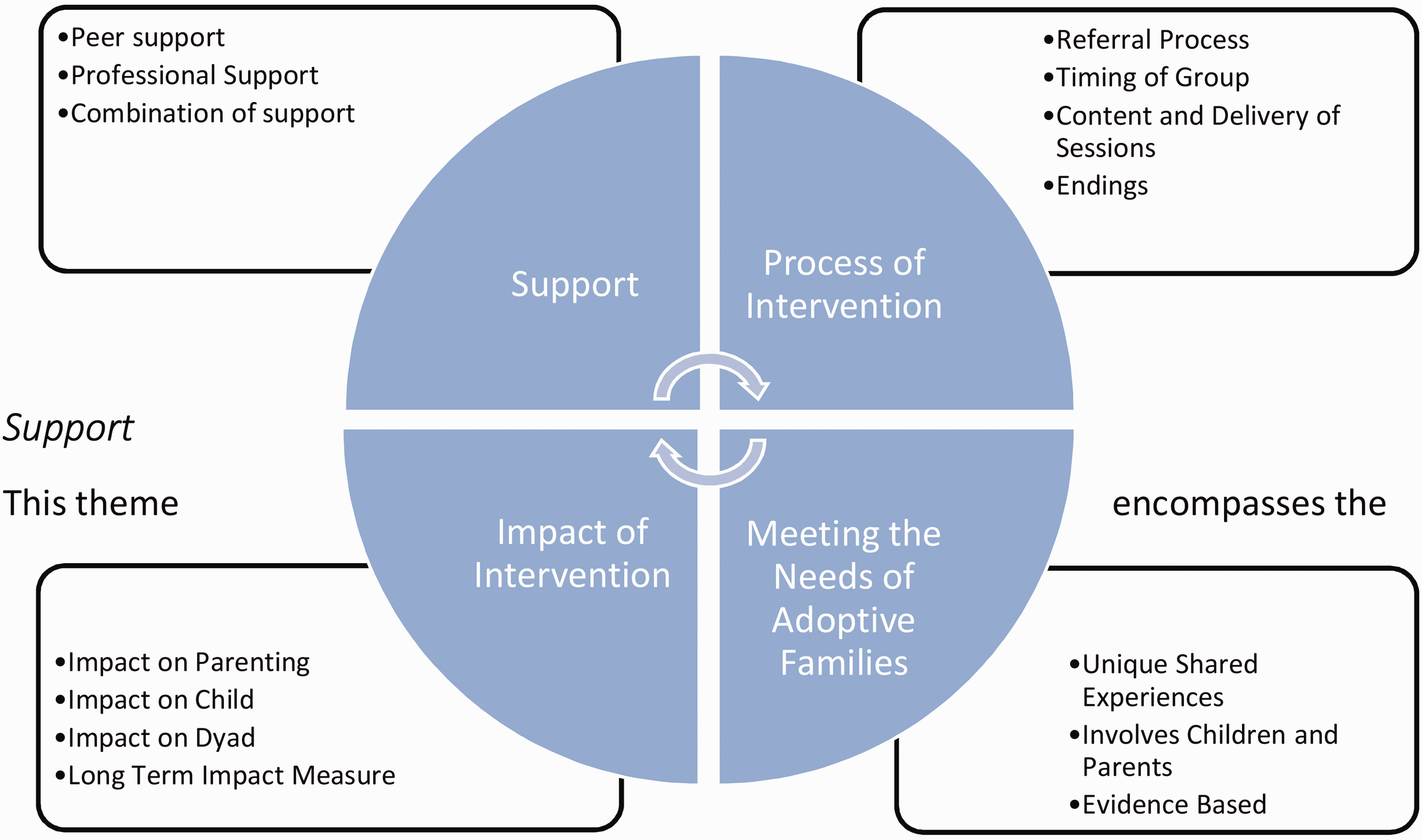
Thematic map.
6. Producing the report
Findings have been reported narratively with consideration of the initial research aims and interview transcripts. Verbatim quotations have been included to support themes and subthemes.
Additional measures were taken to increase the trustworthiness of research (Nowell et al., 2017). The data produced were analysed using deductive-inductive thematic analysis as some of the researcher’s codes and themes were directed by existing ideas and concepts referenced within the literature. A common criticism of thematic analysis is that the interpretation of the data by the researcher is subjective and will be influenced by their own ontology (Robson, 2002). The researcher remained vigilant of their own ontological stance to ensure that while a deductive approach was taken initially, alternative explanations were also examined, and the data were revisited to undertake an inductive level of analysis.
Data from each case were explored in turn according to research questions. Cross-case analysis of the main themes from each data source was used to establish cross-case comparisons (Yin, 2018)
Ethical Statement
The study was carried out in accordance with the Health and Care Professions Council’s (HCPC) general standards of conduct, performance and ethics (HCPC, 2016) and the specific research principles stipulated by the British Psychological Society (BPS) in its Code of Human Research Ethics (BPS, 2014). This study was approved by the host institution’s Ethics Review Committee (Ref: 2021-12731-20402). Given that the population used within the research is particularly vulnerable, several risk mitigations were specifically planned as part of the research design. For example, it was important that there was no indication from professionals involved with the families of placement instability and there were no current child protection or safeguarding concerns. An inclusion criterion and support and distress protocols were developed to ensure that any identified risks were managed appropriately.
Findings
Based on the analysis, a set of four main themes encapsulating key commonalities and differences between the three cases was generated: support, process of intervention, impact of intervention and meeting the needs of adoptive parents.
The themes and subthemes illustrate the factors that influenced the development and delivery of Theraplay® informed group interventions within the RAA by exploring these interventions from both professional and parental viewpoints.
The themes and subthemes are presented in the thematic map (Figure 2).
Support
This theme encompasses the support which was deemed valuable from professionals and peers. Peer support and the importance of finding connections with other adopters was frequently mentioned: What I didn’t expect … was the impact it would have on me, purely being with other adopted parents … I’ve never been, even in a virtual room, with any parents that got it … the first session I found incredibly emotional. (Parent X) What I could have benefited more from sooner was connection with other adopters … that was the pivotal point for me. (Parent Z) … it was great because she was able to support other families, advocate for them and empower them to ask for help. (Focus Group B) … one of the benefits of having an educational psychologist, the therapeutic social worker, and the social worker … is that you’re bringing together people with different skills and knowledge. (Focus Group B) It’s hard to separate the fact that I’ve also had the psychology alongside Theraplay®. I can’t say it’s just purely Theraplay® because it’s hard to pinpoint what I’ve taken from the psychologist, and perhaps merged with Theraplay®. I think we’re managing the way we are because of the combination. (Parent B)
Process Of Intervention
This theme explored the whole sequence of the Theraplay® informed intervention – the referral process through to the endings.
The referral process was discussed regarding how the parents were referred or signposted to the Theraplay® informed group. It was reported within all the focus groups that social workers would initially identify the family rather than the family self-referring. There were also comments suggesting that the referring social workers could be more aware of the intervention and its intended outcomes to ensure they were referring families who would benefit: I don’t think it’s a lack of need; I think it’s the system that we have about identifying families. Because adopters tend to be professional, well-educated, sometimes there’s a perception that they don’t need it. (Focus Group 2) We’re regional and across five areas. How do we ensure equal access to the programme … we’ve got a good venue now … but in terms of an equality of access, we should be moving around the region. (Focus Group 2) Over time I’ve started to think about … some occasions where it does not work out in a group situation. If a child is going through another type of assessment, like an autism assessment …being in a group situation could be very difficult. (Focus Group 2) I think it was essential for them [to be able to participate online]. We’ve so many families where only one parent is able to come, so it just helps the other parent to feel included. (Focus Group 3) … we’ve talked about the next groups, showing them a video of the inside of the hall, they can show the children as well, to get them prepared for the building and what it looks like. (Focus Group 1) When you try and factor in having a group of children with the same developmental stage, families that are the same geographical area, at the same stage of adoption, it becomes very difficult to get the perfect group or dynamic. (Focus Group 1) It’s really challenging work to deliver an intervention that meets everybody’s needs because there might be children that need to be regulated down and children that need to be regulated up, and how you manage that in a group is actually interesting. (Focus Group 1) A lot of it is capacity barriers, accessing the training … to do your Level 1 and group training is five days and there is a cost associated with that; whether the service can release you to do training and have the funding for you to do it, that’s another issue. (Focus Group 2) The issue is capacity because it’s intensive support, it requires a group leader and a facilitator. It’s people’s time, which is intense … it’s a lot of time when we’re short staffed. (Focus Group 1) It was useful because it was done in a very safe space … I think it was just a very warm place for everybody. (Parent Y) I think it’s been a bit of a light-heartedness to the quite difficult circumstances … Theraplay® activities are really helpful because they’re fun. (Parent X) How do you make most efficient use of the resources and the time that you have to meet the most number of children and families? … I’m really conscious about not using up too much of the ASF [Adoption Support Fund] money because they might need to access other things. (Focus Group 2) It probably would have been even better if we could have an online session at the end of the programme … We can have an opportunity to reflect on the learning from the six face-to-face sessions … when you’re there in person, all the kids are there, it’s hectic, it’s noisy, it’s fun, it’s playful but there’s not the opportunity to sit and think through things with parents. (Focus Group 1)
Impact Of The Intervention
This theme focused on the immediate impact on the parents and children but also on the relationships between dyads.
Parents shared that attending the Theraplay® informed intervention had changed their parenting style to a certain extent. It had given them a toolkit of strategies to use at home, and it had reminded them of other parenting approaches that they had either used with their own birth children or experienced when they were parented themselves: She loves ‘pop cheeks’. I mean the simplest thing in the world … I think what it’s taught me … it doesn’t have to be a puzzle for half an hour. It can literally be five minutes, a way of us just being … (Parent Y) I felt like they [the parents] were going through the motions and doing it all well, but by the end they could relax into it together and feel comfortable when things didn’t go well. (Focus Group 2) It broke the negative cycle I was in, and that was fundamental, because things would have been quite serious otherwise. Engaging with Theraplay® saved the placement, I think. (Parent X) Just seeing her progress in six weeks from a little girl that sat on my lap who didn’t do anything … to week six, copying everything [female name] did, talking to [female name] … leaving me and going under the parachute was massive in a short space of time. (Parent X) He loves the attention from us, and we love giving it to him … it’s definitely built my relationship with him, 100 percent … he’s a lot happier … we’re spending more quality time with him. (Parent Z) We wanted the message that all of us gave to [the] parents to be: this is just the start of your Theraplay® journey … (Focus Group 3) It would be really interesting, from a longitudinal perspective, to see where they’re at in a couple of years’ time. Look at the trajectory, what do they access, what support, what time. (Focus Group 2) As a general intervention it’s been deemed as an effective approach. We’ve had conversations about what the evidence base is for Theraplay®. Anecdotally from the feedback and evaluations we’ve done with our families over time, it’s been a really valued support. (Focus Group 2)
Meeting The Needs Of Adoptive Parents
This theme explores the reasons why Theraplay® informed interventions were chosen as a support for adoptive families within the RAA. The findings are from a professional viewpoint only and were analysed across the case studies.
There was a consensus among professionals that the theory behind Theraplay® seemed to match the needs of adoptive parents. Much of the Theraplay® informed intervention delivered was based upon developing attachment, building relationships and connection, and focusing on the principles of attunement: What we felt was missing from the offer was the opportunity to be together with families supporting them practically … Theraplay® is attachment-based and the goal for us was about strengthening those early bonds and relationships … it felt like a good fit. (Focus Group 1) For very young children or early placement, there’s not that many therapeutic interventions that involve the child. A lot of the time, we are working through the parent. (Focus Group 1) They might go to other community groups … often you’re asked about your birth story, and it can be really isolating … For a lot of adopters, it was meeting a need about being with other people who know where they’re at, have experienced similar things and are building their support networks. (Focus Group 1)
Discussion
This research aimed to explore a Theraplay® informed group with adoptive families by gathering the views from both professionals working in an RAA and adoptive parents. The findings are summarised below in relation to the three research questions. Limitations of the research and implications for professional practice are also considered.
The first research question focused on how attending a Theraplay® informed group supported adopted children and their families. Access to peer support was identified as a valued element of the intervention and featured within the findings. Dawson’s (2021) research stated that adopters can feel isolated or report a lack of support from friends and relatives as parenting an adopted child comes with unique challenges. This view is backed up by the research of Bonin and colleagues (2014), who found that informal support, such as peer-support groups or talking with other adopters, appeared to help adopters cope with the day-to-day challenges of parenting. Research conducted by Selwyn and Lewis (2020) discovered that parents found the most useful parts of attending training were the breaks and lunchtimes when they were able to form support networks. Parents within the current research highlighted the ability to connect with other adopters as a benefit of the group and noted that these relationships had continued outside of the Theraplay® informed group, with some leading to lasting friendships.
Having access to multidisciplinary professionals via the group was also deemed important to the adopters. It provided a safe space for them to be with their children while also enabling them to be led by a skilled adult with expertise in adoption and therapeutic work. Selwyn, Wijedasa and Meakings (2014) found that working in a multidisciplinary way was the best means to provide services to adoptive families and that increasing the work of psychologists within those teams would help to reduce family waiting times for support. The current research goes some way to support the hope of reducing waiting times for families, due not only to the multidisciplinary factor but also the nature of the group model. This model enables more families to access support in a timely manner with some families then going on to receive more targeted support.
Professional opinions on why Theraplay® informed group interventions were chosen as a support for adoptive families highlighted the importance of the theoretical underpinnings of Theraplay® and how this can support this population. Theraplay® is an attachment-based therapeutic intervention that helps children and adults to build healthy relationships (Francis, Bennion and Humrich, 2017). Norris and Lender (2020) propose that one of the hopeful goals of Theraplay® is to form a strengthened connection. Attachment theory has become a framework for understanding the difficulties experienced by adopted children (Zeanah, Berlin and Boris, 2011) with early disruptions in care or the potential of the adopted child to have experienced adverse childhood experiences, suggesting that it is unlikely the child has established a secure attachment with a primary caregiver. The multirelational traumas experienced by this vulnerable population would suggest that the development of the parent–child relationship is of paramount importance. Enhancing this relationship was a key finding within the current research that would tentatively indicate that a Theraplay® informed intervention does support strengthened connection within adoption. Moreover, it could be argued that attending a group intervention not only strengthens the parent–child connection but also the bonds between adopters. Although further research would help to strengthen the finding, this adds to research by Kerr and Cossar (2014) who suggest some evidence that early attachment-based interventions are beneficial for this population.
The implementation of the Theraplay® informed intervention within the RAA was adapted to meet the needs of adoptive families. Professionals shared the need to strike a balance between the therapeutic needs of the families and the public funding available for these types of interventions, such as access to the ASF. A recent scoping review identified several research studies that used a modified version of Theraplay® to flexibly meet the needs of the intended population (France, McIntosh and Woods, 2023).
A total of 29 sessions is recommended to facilitate Theraplay® dyadically, as set out within the practitioner’s guide (Norris and Lender, 2020). However, successes have been detailed in research where this number of sessions has not been possible (Eruyar and Vostanis, 2020; Weir et al., 2021). The success of group Theraplay® has also been delineated in research (Francis, Bennion and Humrich, 2017; Weaver et al., 2021). Group Theraplay® has been shown to be successful with adoptive families where it was used alongside additional sensory integration and mindfulness activities (Purrington et al., 2022). Within the current study, six Theraplay® informed sessions were delivered in a group model with family dyads, alongside four parent-only online sessions, which explained the theory and background to Theraplay®, creating a blended model. Parents in the study outlined the benefits of this blended model, such as the opportunity to ask questions of professionals and to discuss the intervention, as well as the online delivery enabling other parents/carers to attend who were not able to access the face-to-face sessions. The professionals in this study suggested that these online sessions were continually being adapted to meet the needs of the families but, overall, they were seen as an important part of the intervention by all participants. This highlights the importance of using practice-based evidence to continually adapt and amend the intervention delivered to best meet the needs of the families.
Within the findings there were no directly negative comments from parents regarding Theraplay® as an intervention. Comments were made suggesting that more sessions would have been beneficial or access to the intervention at an earlier point in their journey may have been useful, but regarding the application, learning and activities the comments were wholly positive. Enhancing connections, noticing positive moments and developing confidence are part of Theraplay® practice, and it is worth reflecting on whether this may have influenced the parental feedback.
Implications For Professional Practice
A review of the role of the EP was undertaken in 2002 which identified not only the levels in which they work (individual, group and organisational) but also the core functions of EPs (consultation, assessment, intervention, research and training) (SEED, 2002). Dunsmuir and Hardy (2016) posit that practitioner psychologists are more commonly accessing further training to deliver interventions to children and families. The role of the EP has shifted somewhat from the traditional focus on assessment to finding effective ways of supporting complex family situations through therapeutic work (Gaffney, 2010). EP work involves using and applying psychological research for early intervention to support families and children. Dunsmuir and Hardy (2016) acknowledge that owing to changes in the commissioning of EP services there has been an increase in demand for access to psychological therapies. With this in mind, Theraplay® is an intervention that is relevant to the work of EPs. Previous research has shown EP involvement in the delivery and evaluation of Theraplay® with some successful outcomes (Dodd, 2009; Francis, Bennion and Humrich, 2017).
The implications from this research for other RAAs would suggest the need to increase the capacity to deliver an attachment-based intervention such as Theraplay® in order to reach a greater number of families. While it is common for RAAs to have specialised social workers within their staffing, it may be less usual for EPs to be among their direct workforces. Fallon, Woods and Rooney (2010) suggest that the commissioning of EP services within children’s services enables their role to expand its contribution further, particularly as many EPs now work in a variety of specialised positions including within adoption. McGuiggan (2021) suggests that the EP’s role is to support children and families and not just schools and local authorities. It was noted that EP services should be prioritising more readily the offer of psychological services to vulnerable children, such as those who are adopted, and involving themselves further in home-based family interventions (McGuiggan, 2021). Furthermore, in the context of working within a multidisciplinary team, EPs have a part to play in supporting the learning of other professionals. Cort and Rowley (2015) suggest EPs are in a good position to offer supervision and training in delivering groups or working with vulnerable families to other professionals.
Despite previous research detailing the benefits of accessing therapeutic interventions for adoptive families, there are implications regarding capacity to deliver these interventions due to resourcing of staff and finance. One of the potential pitfalls of Theraplay® as an intervention is the costly nature of the training and ongoing supervision requirements needed to practise in line with The Theraplay® Institute requirements. The model delivered within this research required qualified EPs with at least Level 1 and group training to facilitate the group, with all facilitators continuing their training and supervision through the practicum available. Other practical difficulties such as location of families and availability of locations to hold the sessions would also need to be considered. Despite these barriers, Theraplay® is one of the only therapeutic interventions that involves both the parent and child. Other early placement support models involve the parent within psychoeducation but do not involve the child directly.
Limitations
The themes emerging from this research are viewed as specific to this RAA, although it is likely we would expect these findings to be relevant and useful to practice within other such agencies in their infancy in developing multidisciplinary teams.
The small sample size and the short-term nature of this research is a limitation. It would have been beneficial to interview more participants, but due to the timing of the groups and the case study design this was not possible. It would also have been useful to gather more longitudinal data.
Future Research
This research has highlighted much good practice within one RAA, and it would be beneficial to gather the views of other adoptive families who are also accessing Theraplay® informed group interventions across the UK in order to generalise the findings.
This study was an initial exploration into the practice with adoptive families. Further research examining a specific outcome measure for Theraplay® would enable practitioners to decipher whether the benefits noted were purely due to the Theraplay® informed intervention or due to its implementation alongside the multi-agency therapeutic alliance and peer support. Given this, it could be useful to comparatively explore the benefits of Theraplay® over an adoption-specific play group.
Looking more generally at adoption support, it might be beneficial to explore what other RAAs are currently offering as early placement support alongside what adoptive parents feel they need. As previously mentioned, taking a more longitudinal approach would also be worth considering.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research and writing of this article was funded by the Department for Education, UK Government, Initial Training in Educational Psychology (ITEP).