
Abstract
Compared to other teenagers, young care leavers tend to have poorer sexual/reproductive and mental health; mental health difficulties may increase risk for poor sexual/reproductive health. This systematic review addresses a gap in knowledge regarding the effectiveness of existing interventions that support care leavers’ sexual/reproductive health (e.g., contraception, pregnancy choices, early parenting). Eight published articles spanning six interventions were eligible. Interventions were associated with improvements in a range of sexual/reproductive health measures (e.g., sexual health knowledge; knowledge of where to get support; attitudes to sexual health practices), with some indicative improvements in self-esteem. However, some studies suggested these improvements may not be sustained. Interventions tended to include a broad age range, with limited programmes specifically aimed at care leavers. While some programmes focused on attitudes toward reproductive health and pregnancy (i.e., contraception), we identified no programme focusing on parenthood choice. We also identified no sexual/reproductive health programme that targeted or assessed associated mental health problems, despite evidence of associations between sexual health and mental health difficulties. Findings suggest that care leavers may benefit from specific sexual/reproductive health supports, but further evidence is needed. Findings also indicate a need for more holistic supports that integrate mental health supports with reproductive/sexual health and consider care leaver decision-making.
Plain Language Summary
Most children in the care system are placed with foster carers until the age of 18 years when they transition from being a looked after young person to a care leaver. Leaving care is considered to be a challenging period. Care leavers are more likely to face multiple challenges and are at increased risk for a range of multiple outcomes compared to the rest of the population. These include poor mental health, early pregnancy and parenthood and removal of their own children from their care. The aim of the present study was to systematically review evidence of existing interventions that support care leavers regarding sexual and reproductive health (e.g., contraception and pregnancy choices) and associated mental health, and to consider the effectiveness of such interventions.
We identified eight published articles spanning six interventions. Interventions were associated with improvements in a range of sexual/reproductive health measures (e.g., sexual health knowledge, knowledge of where to get support and attitudes to sexual health practices), with some improvements in self-esteem. However, some studies suggested that improvements may not be maintained.
Available intervention evidence recognises the importance of supporting sexual health for care-experienced youth; however, while several studies recognised the importance of focusing on attitudes to parenthood, none focused on parenthood choice. None assessed or incorporated mental health needs despite associations between mental and sexual health. Furthermore, few focused specifically on supports during a key transition (such as exiting the care system), despite evidence of increased risk during this period. Further evidence is needed to better address the needs of care-experienced youth.
Introduction
Prevalence Of Care Leavers And Context
The number of children in care in England and Wales has continued to rise steadily. Recent estimates (in 2022) suggest that 82,170 children were looked after, up 2% from the previous year, with 5,570 looked after children being unaccompanied asylum-seeking children (UASC), up 34% from the previous year (Department for Education, 2022). Most are placed with foster carers until the age of 18 years when they transition from being a looked after young person to a care leaver. Plans for this transition should begin at age 16 years (Butterworth et al., 2017). Leaving care is regarded as a challenging period. Care leavers are more likely to face multiple challenges and are at increased risk for a range of multiple outcomes compared to the rest of the population, including poor mental health, early pregnancy and parenthood and removal of their own children from their care (Häggman-Laitila, Salokekkilä and Karki, 2018).
Local authorities in the UK have a duty to prepare young people in their care for adult life (Wade, 2011): all care leavers should have a ‘pathway plan’ that, wherever possible, should be jointly prepared and agreed by the child and the authority (Children Leaving Care Act, 2000; Stein, 2019). However, a recent review suggested that many care leavers describe the process of leaving care as unprepared and unfocused, with no opportunity for them to participate in the decision-making regarding their own future (Häggman-Laitila, Salokekkilä and Karki, 2018). Furthermore, in a recent report of care leavers in England, almost one quarter (23%) of care leavers who responded to a survey did not feel any involvement in plans and decisions about their care, and a further one-third felt only ‘a little involved’ (UK Government, 2022). With regards to UASC arriving in the UK, many arrive in their teens so there is limited time to undertake assessments and identify provision needs while considering support plans for leaving care (Barrie and Mendes, 2011; Wade, 2011). It was estimated that only 12% of UASC aged 16 years and over had a pathway plan on file (Barrie and Mendes, 2011).
Evidence suggests that care leavers do not benefit from the same supports and resources as their non-care leaver counterparts (Gullo et al., 2021), often lacking support from family members and former carers (Häggman-Laitila, Salokekkilä and Karki, 2018). It has also been argued that unaccompanied migrant care leavers may be more vulnerable at this transition period, given their status as young people in care, as adolescents, as migrants and being unaccompanied (Gullo et al., 2021). It is therefore necessary to better understand effective interventions that may promote better, more positive outcomes in this group of young people.
Studies from the US, Australia, and Ireland highlight that looked after children are at increased risk of being exposed to a range of disadvantage and risk factors associated with sexual and reproductive health (Combs et al., 2022; Hyde et al., 2016a) including substance misuse, sexual exploitation, domestic and community violence, trauma, numerous placements and unstable living situations, as well as mental health challenges (Buttram, Pagano and Kurtz, 2019; Harmon-Darrow, Burruss and Finigan-Carr, 2020; Lieberman et al., 2014). Indeed, a history of previous abuse and neglect and subsequent mental health issues may lead to difficulties in navigating and negotiating sexual relationships (Purtell, Mendes and Saunders, 2020).
Sexual And Reproductive Health Of Care Leavers
Compared to other teenagers, young care leavers tend to have poor sexual and reproductive health (Combs et al., 2022), including poorer contraceptive use, increased rates of transmission of sexually transmitted infections (STIs) and HIV (Nixon, Elliott and Henderson, 2019). International evidence suggests that care leavers, including those in the UK, are also more likely to experience unintended early pregnancy/parenthood, are less likely to choose pregnancy termination, and more likely to experience the removal of children from their care (Buttram, Pagano and Kurtz, 2019; Chase et al., 2006; Combs et al., 2018b; Combs et al., 2022; Craine et al., 2014; Häggman-Laitila, Salokekkilä and Karki, 2018; Mezey et al., 2017; Purtell, Mendes and Saunders, 2020; Roberts et al., 2017; Vinnerljung, Franzén and Danielsson, 2007; Wall-Wieler et al., 2018).
While few studies consider whether pregnancies were wanted and/or intended (Ethier, 2022), it is important to recognise that early parenthood may be considered as a positive experience for some, and for others it may be a less positive choice (Mezey et al., 2017; Roberts et al., 2017). For example, evidence from the US and the UK highlights that early motherhood may be perceived as a way of rectifying earlier adverse experiences, providing stability and meeting emotional needs, a chance to be part of a family, and motivation and opportunity for achievement and responsibility (Aparicio, Pecukonis and O’Neale, 2015; Chase et al., 2006; Knight, Chase and Aggleton, 2006; Mezey et al., 2017; Radey et al., 2016). However, one recent US study of looked after children suggested that only 10% held pro-pregnancy attitudes, with over half expressing anti-pregnancy attitudes, and the remaining one-third holding ambivalent beliefs (Combs et al., 2018a). Studies from both the US (Combs et al., 2018b; Shpiegel and Cascardi, 2018) and the UK (Chase et al., 2006; Mezey et al., 2017; Sackler, 2021) highlight that early parenthood is also associated with a range of adverse socioeconomic and health outcomes, including mental health difficulties. Despite the challenging decisions associated with early parenthood, one study suggested that less than 50% of care-experienced young people who faced parenthood said they had received support to help make a decision about a pregnancy, and most reported pressure from professionals, carers or birth parents to have an abortion (Chase et al., 2006). While there is limited evidence regarding parenthood choice, more recent studies suggest that looked after children and care leavers receive little support and advice to support contraception and contraception choice (Dworsky and Courtney, 2010; Hyde et al., 2016a).
This evidence highlights the need to better understand supports for care leavers regarding contraception, pregnancy and parenting choice. The focus of the current review is on interventions that focus on these specific indicators of sexual/reproductive health.
Care Leavers’ Mental Health
Young people in the UK who are looked after (Rees, 2013) and care leavers (Stein and Dumaret, 2011) demonstrate the highest rates of mental ill health, but the poorest access to mental health services (Butterworth et al., 2017), with rates of mental illness up to six times greater compared to their non-care experienced peers (Butterworth et al., 2017). Care leavers are more likely to self-harm, commit suicide, exhibit risk-taking behaviours and have higher rates of psychopathology compared to non-care experienced peers (Butterworth et al., 2017; Häggman-Laitila, Salokekkilä and Karki, 2018; Harder et al., 2020). For example, it has been estimated that in the UK, 57% of young people living in foster care and 96% of those in residential care had some form of psychiatric disorder, compared to 15% of those living with their families (Stein and Dumaret, 2011). An early English study found that almost two-thirds of care leavers had thought about taking their own lives, with 40% having tried to do so at the time they were leaving care (Saunders and Broad, 1997, in Stein and Dumaret, 2011). Another UK study examining mental health of care leavers as they transitioned out of care (Dixon et al., 2006; 1997, in Stein and Dumaret, 2011) found that at baseline (approaching transition out of care), around 42% experienced emotional and behavioural difficulties. This study also provided evidence of an increase in mental health problems across the transition out of care: 12 to 15 months later, the proportion of care leavers reporting mental health problems doubled (from 12% to 24%) and 4% had made suicide attempts. Further research also suggests increases in mental health problems after leaving care, with a study in Scotland suggesting a fourfold rise (Dixon and Stein, 2005, in Stein and Dumaret, 2011). Furthermore, disadvantage appears to continue into adulthood, with evidence from a UK cohort study suggesting that 24% of those in care had depression by age 30 years compared to 12% of those not in care (Cameron et al., 2018).
UASC are also at increased risk of mental health difficulties, with the prevalence of psychological distress estimated to be approximately 40% to 50% in the UK (Ehntholt et al., 2018; Groark, Sclare and Raval, 2011; Wade, 2011). UASC experience a range of trauma prior to arrival in the UK (Ehntholt et al., 2018; Groark et al., 2011; Sirriyeh and Raghallaigh, 2018) or other host country (e.g., Australia: Barrie and Mendes, 2011; Ireland: Sirriyeh and Raghallaigh, 2018), and continue to experience high levels of stress and post-traumatic stress symptoms. Despite high levels of mental health difficulties, a UK study suggests that only a small proportion were in contact with mental health services (Sanchez‐Cao, Kramer and Hodes, 2013).
Care leavers may be reluctant to access mental health supports (Häggman-Laitila, Salokekkilä and Karki, 2018). Another UK study suggests that the process of leaving care can also exacerbate existing mental health difficulties (Butterworth et al., 2017), and this may be compounded by the fact that those receiving support from child and adolescent mental health services (CAMHS) may also additionally experience a move to adult services while transitioning out of care (Butterworth et al., 2017; Häggman-Laitila, Salokekkilä and Karki, 2018). This points to substantial and persistent unmet mental health needs of care- experienced youth, and a need to improve access to a range of services (Bunger et al., 2021; Harder et al., 2020).
Links Between Reproductive Health And Mental Health
There is a robust association between poor mental health and poor sexual/reproductive health behaviour (Patel et al., 2007): mental health problems (e.g., anxiety, depression and self-harm) are associated with unprotected sex and STIs in adolescents (Adan Sanchez et al., 2019; Bennett and Bauman, 2000; Gambadauro et al., 2018; Harmanci et al., 2023; Hipwell et al., 2011; Ramrakha et al., 2000) and pregnancy/early parenthood (Gambadauro et al., 2018). Where research has focused on looked after children and care leavers, evidence from the US and Australia again suggests a robust association between mental health difficulties and behaviours that increase risk for poorer sexual health outcomes and early pregnancy (Buttram, Pagano and Kurtz, 2019; Combs et al., 2022; Lieberman et al., 2014; Purtell, Mendes and Saunders, 2020; Stevens et al., 2011).
Considering the mechanisms through which mental health difficulties may impact on sexual and reproductive health can help to explain individual variation in risk, and thus provide insights into intervention and prevention targets. Evidence suggests that internalising problems may increase risk, at least in part, through low perceived self-efficacy/self-esteem, decreased assertiveness and reduced ability to negotiate safe sex (Aparicio et al., 2021; Patel et al., 2007). Mental health difficulties such as anxiety and depression may also influence sexual/reproductive health via substance use, which can lower inhibitions and impair decision-making (Aparicio et al., 2021; Bennett and Bauman, 2000; Harmanci et al., 2023; Ramrakha et al., 2000). Finally, looked after children may not be aware of the relationship between past trauma, mental health and sexual/reproductive health (Aparicio et al., 2021). Pre-care experiences and earlier experiences of trauma (e.g., abuse and neglect) increase risk for mental health difficulties and may lead to problems negotiating sexual relationships (Nixon, Elliott and Henderson, 2019; Purtell, Mendes and Saunders, 2020; Stevens et al., 2011). Care leavers may conflate sex with love and affection (Purtell, Mendes and Saunders, 2020). Looked after young people may also engage in behaviours associated with poorer sexual health outcomes as maladaptive coping strategies (e.g., to ‘numb emotions’ or feel social connections: Aparicio et al., 2021). It has also been suggested that with an accelerated transition to adulthood (compared to non-care leavers), care leavers may seek a partner and opt to have children (Purtell, Mendes and Saunders, 2020).
It is important to recognise that the converse may be observed, with sexual/reproductive health predicting subsequent mental health difficulties. For example, lack of condom use has been associated with increased anxiety symptoms; and number of sexual partners has been associated with elevated depression symptoms and substance use in a study of African American out-of-school youth (Turner et al., 2011). Other US studies suggest that if peers are aware of looked after children/care leavers contracting an STI, individuals may be teased or ostracised, with social isolation and rejection increasing risk for subsequent mental health problems (Aparicio et al., 2021). Early pregnancy and parenthood can also have considerable impacts on youth mental health (Craine et al., 2014). Evidence suggests that where UK care leavers enter parenthood, they are more likely than their non-care leaver counterparts to experience mental health problems (Mendes, 2009a; Roberts et al., 2017). Existing mental health problems can also make discussions regarding sexual/reproductive health more difficult for care-experienced young people (Albertson et al., 2018).
These findings highlight a complex bidirectional relationship between youth mental health and sexual health (Harmanci et al., 2023), demonstrating why a more holistic approach to care may be beneficial. Supporting mental health may reduce risk behaviours and support engagement with services; supporting reproductive/sexual health may reduce risk of subsequent mental health difficulties. This suggests a need to align mental health and sexual/reproductive health supports for adolescents, and particularly care leavers who are considered to be at greater risk. To date, evidence suggests that this may be insufficiently addressed, in part due to the discomfort of staff, foster carers and young people to discuss such topics (Aparicio et al., 2021). Discomfort may be linked to lack of trust with looked after children and care leavers anticipating judgement and rejection, and carers and staff concerns regarding approaching such topics in a trauma-informed and sensitive way (Aparicio et al., 2021).
Interventions And Supports For Sexual/Reproductive Health And Associated Mental Health
It is recognised that there is a disparity between the support needs and provision of care-experienced parents, with limited evidence regarding effective interventions for this population, including in the UK (Roberts et al., 2017). While looked after young people tend to engage in early sexual activity, and may therefore require support earlier in their development, evidence also suggests that supports are needed during the transition to becoming a care leaver (Purtell, Mendes and Saunders, 2020). Teenage pregnancy strategy interventions in the UK do not impact care leaver populations despite being highly successful in reducing teenage pregnancy incidence in the general population (Mezey et al., 2017), highlighting the need for targeted approaches. Yet there is currently a lack of evidence-based care leaver interventions to support contraception, pregnancy and parenthood, and associated mental health difficulties.
The aim of the present study was therefore to systematically review empirical evidence of existing interventions that support care leavers regarding sexual and reproductive health (e.g., contraception and pregnancy choices) and associated mental health, and to consider the effectiveness of such interventions. Care leaver mental health will be considered as an outcome (where assessed) in the context of reproductive health interventions, given the associations with reproductive health, and evidence that care-experienced youth are at increased risk of mental health difficulties. Where possible, we will examine any supports for UASC care leavers given the increased risk of adverse outcomes during this transition period for this group.
Methods
This systematic review (study protocol registered on PROSPERO 2022 CRD42022328405) was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2015).
Sources Of Information And Search Strategy
An electronic search was conducted through five e-databases: PubMed, Applied Social Sciences Index & Abstracts (ASSIA), Web of Science (WoS), Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Social Care Online (SCIE). The search strategy consisted of three key concepts: (1) Intervention, (2) Population and (3) Reproductive Health and Parenthood. The search was limited to English-language articles published from 1 January 2002 to 1 January 2023. Supplementary Table S1 demonstrates the building of the search query in Web of Science with keywords and synonyms. A similar approach was used for the other databases. In addition, we searched references from the included studies.
Eligibility And Selection Criteria
Inclusion criteria for the systematic review were (a) papers published in the English language; (b) publication within the last 20 years; (c) qualitative, quantitative and mixed methods papers; (d) papers reporting on studies undertaken in the last 20 years; (e) papers reporting on care leaver or/and foster care populations; (f) included participants at 14 to 25 years old; (g) papers focusing on contraception, pregnancy or/and parenting; and (h) existing interventions that support care leavers/foster care youth regarding contraception, pregnancy choices and early parenting.
LBJ and RS screened articles for title and abstract independently. Independent full-text screening was then conducted. At each stage any discrepancies were discussed until consensus was reached. Both authors remained blinded during the process (see Figure 1 for PRISMA diagram).
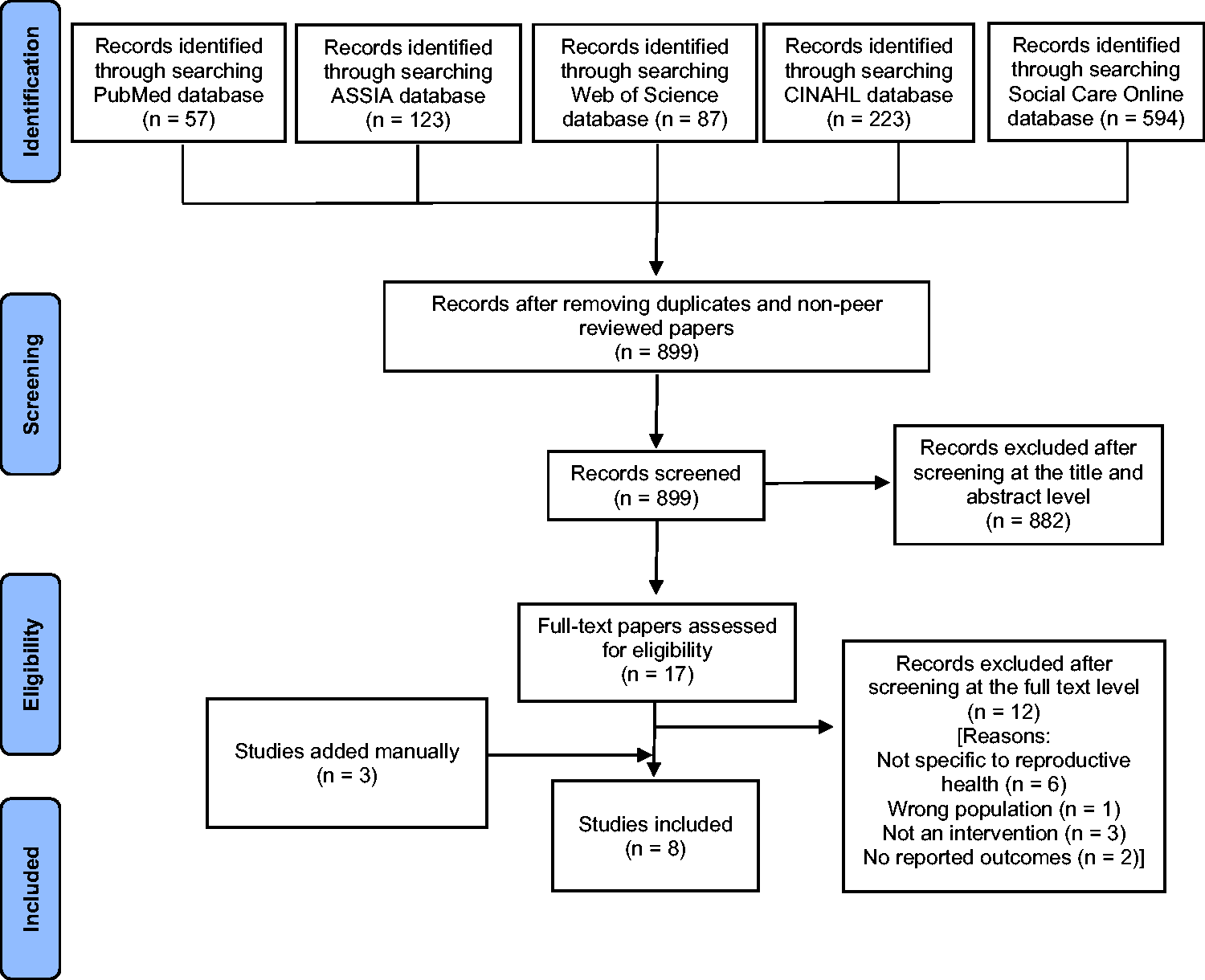
PRISMA diagram.
Data Extraction
We extracted core information pertaining to existing effective interventions that support care leavers regarding contraception, pregnancy choices, early parenting and associated mental health difficulties. We included studies that focused on sexual health knowledge, attitudes and/or behaviours in care-experienced youth. We considered the study design, methodology and intervention details. We also included country of intervention study given the different service contexts across nations. Where available we extracted information pertaining to associated mental health (intervention component and outcomes). Where available we also sought to include interventions specific to, or studies that included UASC care leavers. Feasibility and pilot studies were also included. Where reported we also included effect sizes (see Table 1).
Summary of interventions identified in systematic review.

Quality Assessment
To assess the quality of each study, we used the Quality Index (QI: Downs and Black, 1998). The QI is a 27-item checklist designed for use with both randomised controlled trials (RCTs) and non-randomised studies. Each item is rated as ‘yes’ (1), ‘no’ (0), or ‘unable to determine’ (0). The QI contains four subscales: reporting; external validity; internal validity (confounding and selection bias); and power. Items within each subscale are summed with higher scores indicating higher quality. The subscales can also be summed to give an indication of overall quality.
Results
A systematic search of five electronic databases: PubMed (n = 57), ASSIA (n = 123), Web of Science (n = 87), CINAHL (n = 223) and Social Care Online (n = 594), resulted in 1,084 articles. After excluding 185 articles which were duplicates or wrong publication type, 899 were eligible for review. Eight hundred and eighty-two articles were removed at the title and abstract stage, leaving 17 articles for full text review. Following full text screening, five papers were eligible to be included. We then reviewed references of eligible studies. We identified eight studies spanning six interventions (see Figure 1).
The six interventions were: (i) Heart to Heart Training; (ii) Smart teens Informing, Healing, Living, Empowering for Youth in or at-risk for foster care (SiHLE-YFC); (iii) Power Through Choices (PCT); (iv) Making Proud Choices (MPC); (v) Be Proud! Be Responsible!; and (vi) a peer mentoring programme (see Table 1 for a summary of studies). Three of the eight papers examined Power Through Choices, all from the same study (PCT; Green et al., 2017; Oman et al., 2016, 2018). Two papers examined Making Proud Choices (Combs et al., 2019; Taylor et al., 2020), one of which involved an adaptation of Youth in Out-of-Home Care (MPCOOH: Taylor et al., 2020). The second study allowed providers to select either Making Proud Choices or Be Proud! Be Responsible! (with Making Proud Choices being an extension of the Be Proud! Be Responsible! intervention) depending on the perceived needs of their specific population (Combs et al., 2019).
All studies were conducted in the US, with the exception of one UK study (Mezey et al., 2015). All programmes targeted care-experienced youth/looked after children with the exception of Heart to Heart training, which targeted foster carers (Ahrens et al., 2021). Power Through Choices (Green, 2017; Oman et al., 2016; 2018) targeted those in residential care which included those in the care system/child welfare (i.e., foster care) in addition to those in the juvenile justice system. We identified no interventions that reported inclusions of UASC care leavers, nor did we identify any interventions specifically targeting this group.
Two studies recruited approximately 50/50 male-female care-experienced youth (Ahrens et al., 2021; Boustani, Frazier and Lesperance, 2017), although one of these studies (Ahrens et al., 2021) targeted foster carers and 95% of their sample of caregivers was female. Three papers (Green et al., 2017; Oman et al., 2017, 2018), all from the same study and same intervention (Power Through Choices), recruited 78% males, likely due to the fact that most of the residential homes in the study were male-only. Conversely, one study (MPCOOH; Taylor et al., 2020) recruited 70% female care-experienced young people and another (Peer Mentoring; Mezey et al., 2015) recruited 100% females. Most studies included a broad age range, from 13 to 19 years (Ahrens et al., 2021; Boustani, Frazier and Lesperance, 2017; Combs et al., 2019; Green et al., 2017; Oman et al., 2016; 2018; Mezey et al., 2015), including those in care as well as those approaching the transition to care leaver. One study also included care leavers between the ages of 19 to 25 years as mentors in a Peer Mentoring programme (Mezey al., 2015). One study specifically focused on the period leaving care (age 18 to 23 years: Taylor et al., 2020).
With the exception of Peer Mentoring, the remaining interventions were education/curriculum based. Most were six-to-eight hours in total (Heart to Heart, Ahrens et al., 2021; Be Proud! Be Responsible!, Combs et al., 2019; Making Proud Choices, Taylor et al., 2020; Combs et al., 2019; SiHLE-YFC Boustani, Frazier and Lesperance, 2017), although delivery of session times varied. For example, Heart to Heart delivered the six-hour content in one day or two half-day sessions, whereas SiHLE-YFC (delivered content in four 90-minute sessions (see Table 1 for further details).
Assessment Of Study Quality And Risk Of Bias
We assessed four aspects of study quality (reporting; external validity; internal validity [confounding and selection bias]; and power) using the Quality Index. Scoring of each study using the QI can be found in Supplementary Table S2. We found that identified studies had clearly described studies and therefore scored well on study reporting. External validity may be less robust across all studies. Studies did not report on the representativeness of the sample compared to the population they were recruiting from, and few studies reported on whether those who participated were representative of the population from which they had been recruited. Participants were not able to be blinded to the intervention they received and, as all studies relied on self-report measures, it was also not possible to blind those measuring the intervention outcomes.
Internal validity varied between studies. Five studies were RCTs: Heart to Heart (Ahrens et al., 2021); Power Through Choices (Green et al., 2017; Oman et al., 2016; 2018); Peer Mentoring (Mezey et al., 2015). Of these, two studies first included a feasibility/pilot studies as an initial phase (Heart to Heart, Ahrens et al., 2021; Peer Mentoring, Mezey et al., 2015). The remaining three studies used pre-post assessments (Making Proud Choices/Be Proud! Be Responsible! (Combs et al., 2019); SiHLE-YFC (Boustani, Frazier and Lesperance, 2017); MPCOOH (Taylor et al., 2020), the last of which was a feasibility study. All studies took a longitudinal approach, but follow-up periods varied from one month (Boustani, Frazier and Lesperance, 2017) to 12 months (Green et al., 2017; Mezey et al., 2015; Oman et al., 2016; 2018).
Finally, sample sizes also varied across studies. Apart from three studies (all Power Through Choices: Green, 2017; Oman et al., 2016; 2018) which had a sample of over one thousand and demonstrated sufficient power to detect effects, most studies had small sample sizes with limited power. While one study reported a sample size of just over 800, 72 of the participants were from foster care, with the rest being recruited specifically from the juvenile justice system (Combs et al., 2019: Making Proud Choices and Be Proud! Be Responsible!). Furthermore, several studies identified challenges in recruitment and/or retention at follow-up (e.g., Boustani, Frazier and Lesperance, 2017; Mezey et al., 2015).
Intervention Effects
It should be noted that one study (Peer Mentoring, Mezey et al., 2015), as a pilot study did not aim to detect statistical intervention effects, but findings presented were indicative of possible intervention effects.
Five of the six interventions demonstrated significant improvements in sexual health knowledge (Heart to Heart, Ahrens et al., 2021; SiHLE-YFC, Boustani, Frazier and Lesperance, 2017; Power Through Choices, Oman et al., 2016; Green et al., 2017; MPCOOH, Taylor et al., 2020; MPC and Be Proud! Be Responsible!, Combs et al., 2019), with the Peer Mentoring programme not specifically assessing sexual health knowledge (Mezey et al., 2015). Three studies evaluating two interventions examined youth knowledge of where to get supports/birth control, with interventions suggesting positive impacts (Power Through Choices, Oman et al., 2016; Green et al., 2017; MPCOOH, Taylor et al., 2020).
Four interventions also demonstrated improvements in attitudes to sexual health practices such as condom use (SiHLE-YFC, Boustani, Frazier and Lesperance, 2017; Power Through Choices, Oman et al., 2016; MPCOOH, Taylor, et al., 2020). One of these studies found that intervention effects may impact on specific attitudes, with limited impacts on attitudes to teenage pregnancy and parenting (SiHLE-YFC, Boustani, Frazier and Lesperance., 2017). Two studies also suggested that attitudes to sexual health (e.g., about STIs and pregnancy) had diminished by follow-up (SiHLE-YFC, Boustani et al., 2017; MPCOOH, Taylor, et al., 2020). Another study suggested that while attitudes towards condom use and birth control did improve from pre- to post-test among youth, these effects were only observed in young people in juvenile justice settings but not foster care settings (MPC and Be Proud! Be Responsible!, Combs et al., 2019).
One intervention observed significant decreases in sexually risky behaviours (e.g., condom use, reported STIs and number of sexual partners: SiHLE-YFC, Boustani et al., 2017). Another (Power Through Choices) also suggested significant effects on behavioural intentions to use condoms and birth control (Power Through Choices, Oman et al., 2016, Green et al., 2017), although effects were not sustained at 12 months (Oman et al., 2018). The Power Through Choices intervention also demonstrated lower odds of being pregnant or getting someone pregnant compared to the control group (Power Through Choices, Oman et al., 2016; 2018). Similarly, a second intervention (Peer Mentoring) observed that no participants became pregnant in the year between baseline and the one-year follow-up, indicative of intervention effects (Mezey et al., 2015).
Two intervention studies demonstrated increases in self-esteem (Power Through Choices, Green et al., 2017; Oman et al., 2016; MPCOOH, Taylor et al., 2020), although again, effects may not be sustained with non-significant effects at follow-up (MPCOOH, Taylor, et al., 2020). A third intervention suggested data indicative of improved self-esteem (Peer Mentoring, Mezey et al., 2015).
Discussion
Overall, this review aimed to systematically examine empirical evidence of existing interventions that support care leavers regarding reproductive health (e.g., contraception, pregnancy/early parenthood choices) and associated mental health. Given that the transition out of care can begin earlier in development, we included youth from age 14 years. However, we identified few studies that focused on the transition out of care to support sexual and mental health. Indeed, only one study specifically focused on youth aged 18 to 23 years, aligned with transitioning out of care (Taylor et al., 2020), despite recommendations that a greater focus on support for transition out of care should be prioritised (Mezey et al., 2015).
We also aimed to examine whether these interventions included components addressing associated mental health difficulties. Indeed, recent research on care leaver wellbeing during lockdown suggests some of these problems have been exacerbated by the pandemic (Dadswell and O’Brien, 2022; Kelly et al., 2021), and that professionals providing help to care leavers would like interventions that can be implemented to support care leavers manage contraception, pregnancy and early parenthood and associated mental health issues. Whereas several reviews have considered specific interventions to support mental health (Hambrick et al., 2016) and resilience (Leve et al., 2012) in looked after children, there is a paucity of evidence specific to interventions and supports for care leavers’ mental health support needs (Häggman-Laitila, Salokekkilä and Karki, 2020). Indeed, none of the interventions identified included mental health components or assessed associated mental health difficulties. It was therefore not possible to examine the impacts of interventions on mental health, despite evidenced associations between mental health and sexual health in care leavers (Buttram, Pagano and Kurtz, 2019; Combs et al., 2022; Lieberman et al., 2014; Purtell, Mendes and Saunders, 2020). A recent review of interventions for care leavers in Australia suggested limited improvements in mental health post-care (O’Donnell et al., 2020). Interventions and supports for care leavers making the transition to adulthood (focusing on education, employment, housing) suggest weak evidence of the effectiveness of programmes (Häggman-Laitila, Salokekkilä and Karki, 2020; O’Donnell et al., 2020) and have limited focus on sexual and reproductive health and associated mental health problems.
Sexual health education, services and interventions are typically delivered through parents, schools or community organisations (Combs et al., 2022; Mezey et al., 2017), but accessing these systems may be more challenging for looked after young people who experience disruptions in their placements, family relationships, education and schools, and such supports may therefore not reach them or care leavers (Combs et al., 2022; Nixon et al., 2019; Purtell, Mendes and Saunders, 2020). Care-experienced youth report receiving limited education or information of birth control, with less than half knowing how to access services if required (Buttram, Pagano and Kurtz, 2019; Chase et al., 2006; Combs et al., 2022; Nixon, Elliott and Henderson, 2019; Stacey, 2015). Care-experienced youth may lack resources to discuss sensitive topics confidentially (Combs et al., 2022; Geiger and Schelbe, 2014; Harmon-Darrow, Burruss and Finigan-Carr, 2020). Furthermore, they have greater health needs but tend to have greater barriers to accessing medical care and health care information and therefore have less information regarding sexual and reproductive health (Combs et al., 2022). In addition, one study suggested that it was standard practice to share sensitive information about a looked after child or young person’s sexual health across a team, which was considered to be an invasion of privacy (Hyde et al., 2016b) and may exacerbate barriers to accessing sexual and reproductive health care. The interventions identified in this review may help to support care-experienced youth by bridging some of these barriers to sexual health services and education.
Foster carers are an under-utilised resource (Albertson et al., 2018). In the current review, we identified only one study targeting foster carers (Heart to Heart, Ahrens et al., 2021), which suggested improvements in sexual health knowledge (in foster carers), and improvements in carer–youth conflict and communication. Although the study did not examine whether the intervention impacted on looked after children and young people’s sexual and reproductive health attitudes or behaviours, existing evidence suggests that communication between parents and children about sexual relationships can have positive impacts on youth (e.g., delaying sexual activity and consistently using contraception; Mezey et al., 2017; Nixon, Elliott and Henderson, 2019; Widman et al., 2016). However foster carers may experience barriers to promoting sexual/reproductive health in looked after children: they can be uncertain about their role, or feel uncomfortable providing sex and relationship information, or lack knowledge or training (Aparicio et al., 2021; Harmon-Darrow, Burruss and Finigan-Carr, 2020; Mezey et al., 2017; Nixon, Elliott and Henderson, 2019). Sexual health training for foster carers can reduce these barriers and reduce unwanted pregnancies and STIs in youth (Ahrens, 2021; Albertson et al., 2018; Nixon, Elliott and Henderson, 2019).
While care leavers may have difficulties in establishing and maintaining social networks (Purtell, Mendes and Saunders, 2020; Sulimani-Aidan, 2018), limited evidence suggests that Peer Mentoring and social support may help them with a range of difficulties (Melkman and Benbenishty, 2018; Økland and Oterholm, 2022; Purtell, Mendes and Saunders, 2020; Sulimani-Aidan, 2018), including addressing some of the risk factors that looked after children and young people experience for teenage pregnancy (Mezey et al., 2017), but few studies have examined the role of social support interventions for care leavers (Økland and Oterholm, 2022). Furthermore, it has been suggested that mentoring may be most effective when combined with other programmes (e.g., minimum standard of income, housing, health care, education, employment or training), and more research is needed (Mendes, 2009b; Økland and Oterholm, 2022). Thus, although not specific to sexual/reproductive health supports, other supports have demonstrated impacts on some aspects of sexual/reproductive health. For example, it has been suggested that supportive housing could reduce STIs among care leavers (Häggman-Laitila, Salokekkilä and Karki, 2020). Results from Multidimensional Treatment Foster Care for adolescence (MTFC-A) trials in the US indicate effectiveness in reducing pregnancy rates in girls (Leve et al., 2012). MTFC-A is a multi-component intensive foster care training programme to provide positive adult support and mentoring, close supervision, and consistent limit setting for foster care youth. This suggests that a range of supports may be beneficial for care-experienced youth, and that holistic approaches targeting multiple risk factors could be helpful.
Overall, interventions focused on sexual/reproductive health, and provided evidence of intervention effects on improved knowledge of sexual health and where to get supports. Some interventions demonstrated improved attitudes to sexual health practices, although these were not necessarily sustained at follow-up. Some suggested a decrease in behaviours associated with poorer sexual health outcomes (e.g., reported condom use, reported STIs and number of sexual partners), and reductions in pregnancy. These studies suggest positive impacts of interventions on measures of sexual health in looked after children and young people. In line with previous studies, findings here highlight that professionals consider and distinguish between attitudes/intentions and behaviours – for example, it should not be assumed that young people who use contraception inconsistently have a desire to be pregnant (Combs et al., 2018a). Indeed, a recent study, not relying on retrospective reports, found that only 10% of foster care-experienced youth held pro-pregnancy attitudes, with over half holding anti-pregnancy attitudes and one-third expressing ambivalent views. While some care-experienced youth may view pregnancy positively, this does not necessarily indicate an intension or plan for pregnancy (Combs et al., 2018a). This suggests that there is a need to improve our understanding of young people’s attitudes and views to better meet their specific needs and challenges (including lack of information and resource) and better support care-experienced youth.
Supporting Mental Health In The Context Of Sexual/Reproductive Health Supports
While the association between mental health and sexual/reproductive health is increasingly recognised both in the general population (Adan Sanchez et al., 2019; Bennett and Bauman, 2000; Gambadauro et al., 2018; Harmanci et al., 2023; Hipwell et al., 2011; Patel et al., 2007; Ramrakha et al., 2000) and looked after children and care leaver groups (Buttram et al., 2019; Combs et al., 2022; Lieberman et al., 2014; Purtell, Mendes and Saunders, 2020; Stevens et al., 2011), understanding the mechanisms linked to the complex bidirectional processes is limited in the UK and Irish context (Harmanci et al., 2023). As noted above, we identified no interventions that included mental health components or assessed associated mental health difficulties, despite evidenced associations between mental health and sexual health. There is a need to support care leavers’ mental health; for example, regular ‘mental health MOTs’ throughout their adult life would ensure that care leavers receive appropriate support (Sackler, 2021). There is also a need to integrate mental health with existing youth programmes, including sexual/reproductive health interventions. Given the potential complex bidirectional processes (Harmanci et al., 2023), supporting mental health may reduce risk behaviours and support engagement with services; conversely, supporting reproductive/sexual health could reduce the risk of subsequent mental health difficulties. Aligning mental health and sexual/reproductive health supports would lead to a more holistic approach to supporting care leavers (Häggman-Laitila, Salokekkilä and Karki, 2020; Patel et al., 2007; Purtell and Mendes, 2016). Such holistic programmes should be based on the needs of care-experienced youth and should consider care leaver decision-making (Häggman-Laitila, Salokekkilä and Karki, 2020).
Providing a range of youth health and welfare programmes and services may be less stigmatising and more accessible to young people (Patel et al., 2007). For example, ‘Stand by Me’ (SBM, Purtell and Mendes, 2016) was developed as an holistic support for young care leavers in Australia, and was developed as an adaptation of the Personal Advisor (PA) model in the UK, to avoid siloed services and reduce gaps in support. More research is needed in this area to develop holistic models to support mental and sexual/reproductive health.
Limitations
It is important to acknowledge several potential limitations of the review of interventions.
First, we identified relatively few studies addressing sexual/reproductive health in looked after children or care leavers. Furthermore, no studies included assessments of mental health and so it was not possible to examine the impacts of interventions on associated mental health. It was also not possible to conduct some planned subgroup comparisons (e.g., by gender), as most studies did not examine whether intervention effects may differ by youth gender. We also could not examine any differences by age or transition (to care leaver status) as most studies included a wide age range which encompassed care and the approach to the transition to leaving care but did not examine whether effects differed during this transition period. Only one study (Making Proud Choices (MPC) For Youth in Out-of-Home Care (MPCOOH), Taylor et al., 2020) specifically considered youth as they exited care (age 18–23 years). We were also unable to examine whether effects differed by migrant status as no interventions specifically included UASC care leavers, nor did we identify any interventions specifically targeting this group.
Different search terms may have led to different studies being identified. In addition, the review focused on peer-reviewed published literature and there is a possibility of publication bias in locating programme evidence (studies reporting significant effects are more likely to be accepted for publication than those reporting non-significant or weaker effects). However, several of the identified interventions did involve randomisation to treatment and control group, providing support for the relevance of sexual health supports for care-experienced youth. In addition, different programmes had different follow-up periods and different levels of intensity, making it difficult to directly compare findings. It is also important to consider that some programmes included different populations or targets for intervention (foster carer, care-experienced youth, those in residential care including those in the juvenile justice system), and different populations may have different needs.
Notwithstanding these limitations, our review of programmes designed to support sexual health of care-experienced youth may reduce behaviours associated with poor sexual health outcomes and improve knowledge and attitudes regarding reproductive health (e.g., condom use). However, further work is needed to examine support needs that recognise and support care leaver decision-making, including parenting choice.
Conclusions
Overall, research findings of available intervention evidence recognise the importance of supporting sexual health for care-experienced youth; however, while several recognised the importance of focusing on attitudes to parenthood, none looked at parenthood choice. None presently incorporate mental health needs despite associations between mental and sexual health. Furthermore, few focused in particular on supports specifically during a key transition (exiting the care system), despite evidence of increased risk during this period. This review suggests the benefit of specific supports, but further evidence is needed to better address the needs of care-experienced youth.
Supplemental Material
sj-pdf-1-aaf-10.1177_03085759231212496 - Supplemental material for Interventions to support reproductive and mental health among care leavers: A systematic review
Supplemental material, sj-pdf-1-aaf-10.1177_03085759231212496 for Interventions to support reproductive and mental health among care leavers: A systematic review by Leanne Bogen-Johnston, Natalie Edelman and Ruth Sellers in Adoption & Fostering
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sellers was supported by an Economic & Social Research Council project grant award (ES/N003098/ 1). This research was funded by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration Kent, Surrey, Sussex (NIHR200179). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Supplemental Material
supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.